
Abstract
Studies aimed at understanding the pathology, genetics, and therapeutic response of vitiligo rely on asking a single question about ‘physician-diagnosed’ vitiligo on surveys to identify subjects for research. However, this type of self-reporting is not sufficient. Our objective was to determine if the patient-administered Vitiligo Screening Tool (VISTO) is a sensitive and specific instrument for the detection of vitiligo in an adult population. The VISTO consists of eight closed-ended questions to assess whether the survey participant has ever been diagnosed with vitiligo by a healthcare worker and uses characteristic pictures and descriptions to inquire about the subtype and extent of any skin lesions. 159 patients at the Brigham and Women’s Hospital dermatology clinic with or without a diagnosis of vitiligo were recruited. A board-certified dermatologist confirmed or excluded the diagnosis of vitiligo in each subject. 147 completed questionnaires were analyzed, 47 cases and 100 controls. The pictorial question showed 97.9 % sensitivity and 98 % specificity for diagnosis of vitiligo. Answering “yes” to being diagnosed with vitiligo by a dermatologist and choosing one photographic representation of vitiligo showed 95.2 % sensitivity and 100 % specificity for diagnosis of vitiligo. We conclude that VISTO is a highly sensitive and specific, low-burden, self-administered tool for identifying vitiligo among adult English speakers. We believe this tool will provide a simple, cost-effective way to confirm vitiligo prior to enrollment in clinical trials as well as for gathering large-scale epidemiologic data in remote populations. Future work to refine the VISTO is needed prior to use in genotype–phenotype correlation studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vitiligo is a common acquired disorder of depigmentation characterized by involvement of skin, hair and/or mucous membranes [3, 4, 6, 7]. It affects 0.1–8.0 % of the population in various regions of the world, with an estimated prevalence of ~1 % in Europe and the United States [1]. Vitiligo affects men and women equally and can present at any age, with half of patients developing the disease before age 20 [1]. The pathology of vitiligo is complex, considered at least in part an autoimmune condition [8, 9] that is influenced by multiple genes as well as environmental factors [1, 11, 13, 14].
To accurately study the disease, it is critical that the patient population being studied has a confirmed diagnosis of vitiligo. Often, the most common method for assessing a patient’s disease status on survey tools is through asking a single question about ‘physician-diagnosed’ vitiligo. This type of self-reporting may be insufficient when data are being collected for population-based, outcomes or genetic studies [5]. Such self-reporting could result in a biased sample of patients due to misunderstanding the survey question, underreporting, confusion with other pigmentary disorders, and/or lack of awareness of a diagnosis [5, 12]. Clinical diagnosis by a board-certified dermatologist is also used in genetic and other studies and is the current gold standard for diagnosing vitiligo. However, physically examining each study participant, though more accurate, is neither time nor cost effective in some cases. In the absence of a dermatologist, no validated tool exists that can confirm whether or not a patient has vitiligo as opposed to other hypo- or de-pigmenting skin conditions.
In addition, there are no validated tools that can identify vitiligo phenotypes in the absence of a dermatologist’s examination. These phenotypes may have unique genetic profiles and environmental risk factors that cannot currently be measured due to limitations in tools for identifying study participants. A tool that allows determination of vitiligo subtypes in remote study participants with limited access to a dermatologist could have broad implications for the understanding of vitiligo subtypes as well as improving approaches to treatment.
To address these concerns, we developed and pilot tested the Vitiligo Screening Tool (VISTO) as a means to confirm vitiligo diagnosis and determine phenotype in an outpatient clinic population. We believe such a tool can be useful both for pre-screening patients for clinical trials as well as for use in large-scale epidemiological work where studying remote populations with limited access to a dermatologist would otherwise be a limitation.
Materials and methods
Creation and design
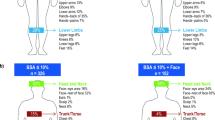
Through a Delphi process involving general dermatologists, outcomes researchers and vitiligo experts, we designed the VISTO as a brief, one-page self-administered questionnaire to confirm the diagnosis and extent of vitiligo (Fig. 1). Modeled after the validated Psoriasis Screen Tool [2], the VISTO consists of 8 questions asking about the type of healthcare worker who gave the participant his/her diagnosis, age of diagnosis, ethnicity, extent of lesions, and effect of lesion appearance on daily life. Participants are asked to choose one of four pictures labeled Fig. 2a–d to represent vitiligo subtypes of segmental (Fig. 2b) versus non-segmental vitiligo including acrofacial (Fig. 2a), generalized (Fig. 2c), and universal vitiligo (Fig. 2d). These four subtypes were chosen because they are the most common in adult populations. Question 7 asks subjects to self-identify how much of their body surface area is involved with disease.

VISTO (VItiligo Screening Tool): a self-administered one-page screening questionnaire

a Photographs of acrofacial vitiligo for use on VISTO. b Photographs of segmental vitiligo for use on VISTO (photographs courtesy of Amit Pandya, MD). c Photographs of vitiligo vulgaris for use on VISTO. d Photographs of vitiligo universalis for use on VISTO
Scoring and scoring algorithms
VISTO contains four questions requiring a “yes” or “no” response. These, along with pictorial question 6, were evaluated for their ability to confirm a diagnosis of vitiligo. We also developed a scoring algorithm under the assumption that a participant who answers “yes” to question 3 (dermatologist-diagnosed vitiligo) and chooses one of the pictorial phenotypes in question 6 would be given a diagnosis of vitiligo based on the hypothesis that being diagnosed by a dermatologist and having characteristic skin lesions would likely represent a true diagnosis of vitiligo. In addition, the primary dermatologist seeing vitiligo patients completed questions 6 and 7 of the VISTO for each vitiligo patient. These data were used to validate patients’ ability to self-report disease phenotype and extent as compared to a dermatologist.
Study population
Institutional review board approval was obtained. All patients 18 years of age and older, of any gender and any ethnicity who visited the dermatology outpatient clinic at Brigham and Women’s Hospital between 18 July 2011 and 21 February 2014 were eligible to receive the VISTO. Consecutive patients with known vitiligo were recruited from a specialty clinic for vitiligo. Non-vitiligo patients were recruited from general dermatology clinics without regard to reason for visit. The VISTO was given to subjects in patient rooms before or after their visit with their dermatologist. A total of 159 questionnaires were administered and 158 were collected: 58 from subjects with confirmed vitiligo, 100 from subjects without vitiligo, and 1 patient without vitiligo declined to participate. The VISTO is being validated only in English initially. We obtained data for gender and age on all participants and data for diagnoses for all non-vitiligo controls by searching patients’ medical records.
Statistical analysis
The population for analysis included eligible participants who self-administered the questionnaire and completed the entire questionnaire. Of the 58 cases recruited, 47 completed the entire questionnaire and were included in this analysis. The primary outcome measure was participant responses to VISTO. These responses were used to determine the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of individual questions as well as our scoring algorithm. Secondary outcome measures included sensitivity and specificity of self-reported phenotype and body surface area involvement as compared to the treating dermatologist. A principle component and factor analysis was also performed to assess the psychometric properties of the tool.
Results
Demographics
159 patients were approached to participate in this study. Of these, 1 control subject declined, and 11 cases did not fully complete the questionnaire. The remaining 147 completed responses were included in this analysis. The non-vitiligo group had more female and more Caucasians than the vitiligo group, but this difference was not statistically significant (Table 1). Non-whites constituted 51.1 % of vitiligo patients. The mean age of diagnosis for vitiligo patients was 29.8. Half of vitiligo cases reported having been diagnosed by a non-dermatologist physician. 24.4 % of vitiligo patients reported being diagnosed by a nurse practitioner or physician’s assistant. 93.5 % of vitiligo patients reported having been diagnosed by a dermatologist. None of the non-vitiligo patients reported having been diagnosed with vitiligo by a dermatologist or non-dermatologist health care provider.
Non-vitiligo participants presented with the following diagnoses: 18 for nevus evaluation, 8 for actinic keratoses, 8 for acne, 7 for non-melanoma skin cancer, 7 for seborrheic keratoses, 7 for eczematous dermatitis, 7 for alopecia, 6 for verruca, 6 for psoriasis, 4 for tinea versicolor, 4 for benign neoplasms (milia, lipoma, dermatofibroma), 3 for rosacea, 2 for vascular conditions (livedo reticularis, chilblains), 2 for cheilitis, 2 for arthropod bites, 2 for dermatitis not otherwise specified, 1 for irritant dermatitis, 1 for lichen planus, 1 for seborrheic dermatitis, 1 for interstitial granuloma annulare, 1 for pruritus, 1 for cutaneous candidiasis, and 1 for earlobe repair.
In terms of disease phenotype, 40.4 % of vitiligo subjects self-reported having the acrofacial pattern (Table 1). 6.4 % self-reported having a segmental pattern. 44.7 % reported having a generalized pattern consistent with vitiligo vulgaris. Finally, 6.4 % responded as having universal vitiligo. 98 % of non-vitiligo subjects responded “not-applicable” or circled none of the answer choices in question 6. Only two non-vitiligo subjects chose a response, one choosing Fig. 2b representing the segmental phenotype and the other choosing Fig. 2c representing generalized vitiligo. Of vitiligo subjects, 27.7 % self-reported having only a few spots that could be covered by one or two palms. 19.2 % reported having scattered spots that could be covered by 5–10 palms. 14.9 % reported having many spots covered by 11–20 palms. The vast majority of controls reported having no or little vitiligo or left this question blank.
Sensitivity and specificity
Table 2 details the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of specific questions in VISTO to diagnose vitiligo. Answering that the diagnosis of vitiligo had been made by a dermatologist had 93.5 % sensitivity, 100 % specificity, 100 % PPV and 97.1 % NPV. Choosing a phenotype for question 6, which asked participants to choose one pictorial phenotype out of 4, had 97.9 % sensitivity and 98 % specificity for the diagnosis of vitiligo. The PPV was 95.8 % and the NPV was 99 %. Evaluating each phenotype specifically, while the sensitivities were lower for each pictorial phenotype individually, the specificity remained very high (99–100 %) as did the PPV (75–100 %). Furthermore, the cumulative sensitivities of each phenotype totaled 100 %. Evaluating reported body surface area (BSA) involvement, responding as having at least a few spots involving one or two palms of the hand showed 100 % sensitivity, 96.7 % specificity, 95.9 % PPV and 100 % NPV for the diagnosis of vitiligo.
Our scoring algorithm was also analyzed. Looking at whether participants self-reported being diagnosed with vitiligo by a dermatologist on question 3 and also selected a phenotype from the photographs in question 6 showed 95.2 % sensitivity, 100.0 % specificity, 100.0 % PPV and 98.0 % NPV. Exploratory factor analysis was then done to analyze the patterns of individual responses (as shown in Online Resource 1). Five items had eigenvalues greater than 1, and one item had an eigenvalue greater than 3.
Exploratory factor analysis
Table 3 details the factor loadings which reveal several interesting findings. Factor 1 shows that subjects who tended to be diagnosed by a healthcare provider also tended to choose Fig. 2a (acrofacial vitiligo) and report that they have scattered spots covered by 5–10 palms. Factor 2 shows that subjects responding as having been diagnosed by a dermatologist or nurse practitioner also tended to choose having vitiligo vulgaris (Fig. 2c) and reports having many spots covering 11–20 palms. Factor 3 similarly shows that subjects who chose Fig. 2d representing universal vitiligo also tended to report having extensive vitiligo covering more than 20 palms worth of body surface area. Factor 4 shows that patients who self-reported having segmental vitiligo (Fig. 2b) reported having only a few spots covered by one or two palms. Factor 5 shows that subjects who reported having scattered spots covering three or four palms did not specifically choose any other answer choices.
Question 8 regarding impact of vitiligo on patients’ quality of life was difficult to analyze due to the low number of cases. However, from the available data, there was no significant correlation between impact on quality of life and self-reported disease phenotype or body surface area involved.
Analysis of self-reported disease characteristics
Table 4 compares how subjects self-identified their vitiligo phenotype via the pictures on the survey to how a dermatologist characterized their vitiligo phenotype. Of the 19 subjects who chose picture A (acrofacial), 12 were diagnosed the same by their dermatologist. 66.7 % who selected picture B (segmental) had segmental vitiligo. It should be noted, however, that only three subjects had dermatologist-diagnosed segmental vitiligo. Of subjects who chose picture C (generalized), 85.7 % were diagnosed with generalized vitiligo by the dermatologist. The only subject with universal vitiligo did not choose the corresponding phenotype picture; however, the n is too small to determine whether subjects with universal vitiligo can be identified through the VISTO. Overall, taking only into account respondents who selected an option on question 6, 80 % of subjects were able to correctly self-identify phenotype. Including all respondents, 69.6 %of subjects accurately self-identified phenotype. In summary, patients did not appear to be highly accurate in choosing the picture that characterizes their dermatologist’s phenotype diagnosis.
The same analysis was performed to evaluate patients’ ability to self-report BSA involvement as compared to the treating dermatologist, and we found that self-report did not reliably correlate with dermatologist estimates of BSA involved (data not shown here).
Discussion
Validation of vitiligo diagnosis is critical for improving the reliability of epidemiological studies. Current studies of this nature rely on a single question about ‘physician-diagnosed’ vitiligo on a survey to identify relevant subjects. It is not clear that this information is enough to support outcomes research. The tool presented here is the first validated questionnaire which can allow subjects to self-report a diagnosis of vitiligo with very high specificity and sensitivity using individual questions and combinations of questions.
The value of VISTO as a screening tool is primarily for use in pre-screening patients for participation in clinical trials as well as for use in performing large-scale epidemiologic studies. Use of VISTO is expected to be more cost effective and time efficient for large population-based studies as compared to having an in-person diagnosis by a dermatologist. While the tool may still miss some cases of disease, it has a very high specificity, making it valuable as a screening tool. Improving the ability to identify those with vitiligo living in various regions can help determine the true prevalence of vitiligo in large populations. It also has potential to improve the reliability of studies that aim to identify risk factors and outcomes associated with the disease.
Our scoring algorithm, looking at whether participants had been diagnosed with vitiligo by a dermatologist on question 3 and also selected a phenotype from the photographs in question 6, had very high specificity for confirming vitiligo. This algorithm showed 95.2 % sensitivity and 100.0 % specificity, suggesting that VISTO is an excellent and very reliable screening tool. Selecting a phenotype from the photographs was also highly predictive of vitiligo diagnosis, with a sensitivity of 100 % and specificity of 99 %. However, this may be falsely elevated due one major study limitation that only four of the non-vitiligo patients had another disorder of depigmentation or hypopigmentation (tinea versicolor). Further validation of VISTO involving more controls with disorders of hypopigmentation would be very useful since these subjects may select a picture on the VISTO that resembles their pattern of skin depigmentation or hypopigmentation, despite the fact that they do not have vitiligo. However, one would expect that patients with a different pigmentation disorder would respond that they have not been diagnosed with vitiligo by a dermatologist. This would rule them out of algorithm I; thus, including both questions 3 and 6 in the algorithm is more reliable.
The accuracy of subjects to self-report phenotype and BSA involvement was not as high as would be desired, limiting the use of VISTO for genome-wide association studies. This can be improved in future versions of VISTO by adding improved photographs of each phenotype and clearer descriptive terms under each photograph. It should also be noted that only three participants had dermatologist-diagnosed segmental vitiligo and only one had dermatologist-diagnosed universal vitiligo. Thus, this study limitation makes it difficult to draw conclusions about how well the VISTO can identify patients with these phenotypes. Furthermore, future iterations of VISTO could include presence of poliosis as well as less common phenotypes including occupational vitiligo and mucosal vitiligo to better capture a variety of phenotypes. Another limitation is that the study was conducted in a hospital-based dermatology clinic with patients who have access to a dermatologist. The sensitivity of algorithm I may decrease in rural or other populations that do not have access to a dermatologist because many patients may answer “no” to question 3 (dermatologist diagnosis of vitiligo).
The survey was not reliable in terms of patients being able to self-report how much body surface area is covered by vitiligo lesions. Patients may have misunderstood this question or may not be as good at determining their body surface area covered by lesions. However, the “no or very little vitiligo” was predictive in that 0.0 % of the cases selected this option, proving that VISTO can be effective as a screening tool. The data from the visual analog scale inquiring about how much subjects’ vitiligo impacted their quality of life were difficult to interpret due to a low number of cases. Future iterations of VISTO would remove this question as it was not relevant to confirming diagnosis. In general, there was no notable correlation seen between impact on overall quality of life and phenotype or body surface area involvement. However, it has been seen before in the literature that BSA involvement may not always correlate with perceived impact on quality of life [10].
Regarding future directions, further studies are needed to validate the VISTO’s reliability in a non-hospital-based setting, including in more rural settings or areas where there is less access to a dermatologist. Including more controls with other pigmentary disorders would be critical as well. Online validation of the tool would also be very useful. Improving the ability of VISTO to allow patients to more accurately self-report phenotype and also adding less common phenotypes to question 6 would be very important to use VISTO for genotype–phenotype correlation studies and is something which the authors are planning. In addition, while it has currently been validated in English only, the VISTO language is simple and can easily be translated for use in other countries. The VISTO’s ability to validate a vitiligo diagnosis provides promising implications for improving epidemiological studies.
References
Alikhan A, Felsten LM, Daly M et al (2011) Vitiligo: a comprehensive overview part I. Introduction, epidemiology, quality of life, diagnosis, differential diagnosis, associations, histopathology, etiology, and work-up. J Am Acad Dermatol 65:473–491
Dominguez PL, Assarpour A, Kuo H et al (2009) Development and pilot-testing of a psoriasis screening tool. Br J Dermatol 161:778–784
Ezzedine K, Lim HW, Suzuki T et al (2012) Revised classification/nomenclature of vitiligo and related issues: the vitiligo global issues consensus conference. Pigment Cell Melanoma Res 25(3):E1–E13
Gawkrodger DJ, Omerod AD, Shaw L et al (2008) Guideline for the diagnosis and management of vitiligo. Br J Dermatol 159:1051–1076
Gelfand JM, Stern RS, Nijsten T et al (2005) The prevalence of psoriasis in African Americans: results from a population-based study. J Am Acad Dermatol 52:23–26
Halder RM, Chappell JL (2009) Vitiligo update. Semin Cutan Med Surg 28(2):86–92
Hann SK, Park YK, Chun WH (1997) Clinical features of vitiligo. Clin Dermatol 15:891–897
LePoole IC, Luiten RM (2008) Autoimmune etiology of generalized vitiligo. Curr Dir Autoimmun 10:227–243
LePoole IC, Das PK, van den Wijngaard RM et al (1993) Review of the etiopathomechanism of vitiligo a convergence theory. Exp Dermatol 2:145–153
Lilly E, Lu PD, Borovicka JH et al (2013) Development and validation of a vitiligo-specific quality-of-life instrument (VitiQoL). J Am Acad Dermatol 69(1):e11–e18
Mason CP, Gawkrodger DJ (2005) Vitiligo presentation in adults. Clin Exp Dermatol 30:344–345
Naldi L, Colombo P, Placchesi EB et al (2004) Study design and preliminary results from the pilot phase of the PraKtis study: self-reported diagnoses of selected skin diseases in a representative sample of the Italian population. Dermatology 208:38–42
Spritz RA (2012) Six decades of vitiligo genetics: genome-wide studies provide insights into autoimmune pathogenesis. J Invest Dermatol 132:268–273
Spritz RA (2011) The genetics of vitiligo. J Invest Dermatol 131(E1):E18–E20
Acknowledgments
The authors would like to thank Cara Joyce for her help in statistical analysis and Dr. Sasha Girouard for her help in database creation.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sheth, V.M., Gunasekera, N.S., Silwal, S. et al. Development and pilot testing of a vitiligo screening tool. Arch Dermatol Res 307, 31–38 (2015). https://doi.org/10.1007/s00403-014-1515-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00403-014-1515-1