
Abstract
Background
The evolution in total knee arthroplasty (TKA) includes the highly cross-linked polyethylene (HXLPE) which has been reported as an effective manner to reduce the wear of the polyethylene and the osteolysis. The purpose of the present study is to synthesize the results of comparative studies between HXLPE and conventional polyethylenes and determine their effect in primary TKA.
Methods
The US National Library of Medicine (PubMed/MEDLINE) and the Cochrane Database of Systematic Reviews were queried for publications utilizing the following keywords: “cross-linked”, “polyethylene”, “HXLPE”, “conventional”, “total knee arthroplasty”, “TKA”, “total knee replacement” and “TKR” combined with Boolean operators AND and OR.
Results
Ten studies met the inclusion criteria and were included in the present meta-analysis with 962,467 patients. No significant difference was found regarding the revision rate for any reason between the patients who received HXLPE and those with conventional liner (OR 0.67; 95% CI 0.39–1.18; I2: 97.7%). In addition, there was no difference regarding the radiolucent lines between the two types of liners (OR 0.54; 95% CI 0.20–1.49; I2: 69.4%). However, with data coming from seven studies enrolling a total of 411,543 patients, it was demonstrated that patients who received HXLPE were less likely to be revised due to aseptic loosening compared to the patients with conventional liners (OR 0.35; 95% CI 0.31–0.39; I2: 0.0%).
Conclusion
The present meta-analysis showed that regarding the overall revision rate and radiographic outcomes there was no significant difference between the two types of liners. On the other hand, the significantly less revision rate due to loosening supports the routine continued use of HXLPE in primary TKA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) remains a successful and durable procedure with its incidence growing in the United States (US). A recent study revealed a 46% increase in the rate of primary total hip arthroplasty (THA) and tripling of the rate of TKAs in a 13-year period [1]. It is estimated that more than 670,000 TKAs were performed in the United States in 2012 alone [2]. However, two of the most common indications for revision TKA historically have been polyethylene wear and osteolysis leading to aseptic loosening with conventional polyethylene [3].
As such, great effort has been given to improve the quality and longevity of polyethylene. In 1963, high density polyethylene was introduced as a way to improve component survival and wear profile [4]. Ultra-high molecular weight polyethylene (UHMWPE) has a high molecular weight, which is thought to result in increased longevity and less wear [5]. UHMWPE has been used in total joint arthroplasty in recent years after highly cross-linked polyethylene (HXPLE) was introduced to the arthroplasty market in the late 1990s [6]. Manufacturing of HXLPE is done by exposing UHMWPE to gamma radiation [7], which breaks up intramolecular bonds and produces free radicals that promote cross-linking across multiple polymer chains [6]. The increased cross-linking of PE chains dramatically improves wear resistance but correspondingly diminishes the toughness of the polyethylene [8, 9].
The use of HXLPE in THA has been shown to decrease liner wear and has demonstrated significantly less osteolysis in comparison to conventional polyethylene liners [10, 11]. The reported incidence of failure due to wear has seen a sharp decline over time, dropping from 12% of all causes of revision TKAs in 2002 to 2% in 2010 [12]. On the other hand, particle-induced osteolysis induced by microscopic debridement of polyethylene components can have significant implications earlier on. The polyethylene particles shed during this process have been well studied as inducers of osteoclasts and inflammatory mediators. These cause subsequent resorption of bone surrounding the implant, which can result in aseptic loosening requiring revision surgery [13, 14]. Aseptic loosening remains a major issue in revision TKA, with the Australian Orthopaedic Association National Joint Replacement Registry reporting it to have accounted for 25% of revision TKAs performed in 2019, which led all causes of revision [15]. Radiographically, aseptic loosening can be seen in the form of radiolucent lines that indicate widening of the bone-cement interface [16, 17].
Thus, promising results seen with osteolysis rates in THA have led to the use of HXLPE in TKA as well. However, its use in TKA has been questioned due to the unique biomechanical environment of the artificial knee joint, which is characterized by greater contact stresses and shear forces compared to the hip [18].
Therefore, the purpose of this meta-analysis was to compare the rates of revision for aseptic loosening, all-cause revision, and presence of radiolucent lines between conventional polyethylene and HXLPE in primary TKA. Our hypothesis was that the use of HXLPE would be associated with lower revision rates compared to conventional polyethylene, especially revision for aseptic loosening given its close association with osteolysis.
Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [19].
Search strategy and search eligibility criteria
A comprehensive search was systematically conducted in Medline/PubMed and Cochrane Central databases. The following terms were utilized in the search algorithm: “cross-linked”, “polyethylene”, “HXLPE”, “conventional”, “total knee arthroplasty”, “TKA”, “total knee replacement” and “TKR” combined with Boolean operators AND and OR. The search was performed by two independent investigators and was reupdated just before the final analyses on June 25, 2020. The detailed PICO (population, intervention, comparison, outcomes) format strategy applied to this clinical scenario is presented in Supplementary Table 1.
A study was included in this meta-analysis if it fulfilled the following predefined criteria: (i) randomized controlled trials (RCTs) or observational analyses comparing HXLPE versus conventional polyethylene in patients undergoing primary TKA, (ii) studies that reported quantitative clinical outcomes data, and (iii) studies published in English language.
The predefined exclusion criteria were: (1) single arm studies reporting only on HXLPE or conventional polyethylene, (2) studies including patients undergoing revision TKAs, (3) case series/case reports, (4) cadaveric, laboratory or animal studies, and v) secondary research articles (e.g., systematic reviews, meta-analyses, letters to the editor or commentaries).
Study selection
Two investigators (blinded for peer-review) assessed the titles and abstracts of all identified records independently. The same investigators independently screened the full texts of all potentially eligible studies, according to the inclusion criteria. Additionally, the references of the included studies were retrieved and manually reviewed to identify further eligible articles, according to the Snowball method. Investigators were blinded to each other throughout the study selection and data extraction processes. Any disagreements or discrepancies were resolved by consensus.
Data extraction and outcomes
Two investigators independently extracted the relevant data from the eligible studies. All disagreements were resolved after discussion and the final decision was reached by consensus. Data were retrieved from all eligible studies in a predefined Microsoft Excel spreadsheet and included study characteristics (first author, year of publication, country of origin, enrollment period), number of patients in each group, sex, age, body mass index (BMI), follow-up duration and polyethylene type used. The primary outcome measure was total number of revision surgeries, and the secondary outcome measures were revisions due to loosening and report of a radiolucent line.
Risk of bias assessment
Risk of bias was assessed in the included studies by two investigators with the Cochrane tool for RCTs and the ROBINS-I (Risk Of Bias in Non-randomized Studies – of Interventions) tool for nonrandomized studies [20, 21]. The Cochrane tool evaluates the following areas: adequate sequence generation, allocation concealment, blinding, baseline characteristics imbalance, patients lost to follow-up, measurement of data, and attrition bias. The following domains for the nonrandomized eligible studies were evaluated: confounding, selection of participants, departure from intended intervention, missing data, measurement of outcomes, and selective reporting. Any discrepancies in quality assessment were resolved via consensus.
Statistical synthesis and analysis
Continuous variables were estimated as mean ± standard deviation (SD), while categorical variables were reported with absolute and relative frequencies. Odds ratios (ORs) with the corresponding 95% confidence intervals (CIs) were synthesized for the outcomes, using a random effects model. Heterogeneity was assessed with the I2 statistic. I2 greater than 75% indicated statistically significant heterogeneity [22]. A forest plot was used to graphically display the effect size in each study and the pooled estimates. A p value < 0.05 was considered statistically significant. STATA 14.1 (StataCorp LLC, College Station, Texas, USA) was used as statistical software.
Results
Literature search and eligible studies
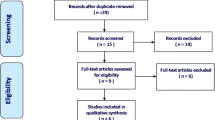
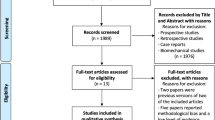
The literature search yielded 189 potentially relevant records, after duplicates were removed. After screening titles and abstracts, 43 articles were retrieved for full-text evaluation. Inclusion and exclusion criteria were then applied to full-texts and 33 studies were excluded for the following reasons: (a) studies with no HXLPE group, (b) secondary review papers and (c) studies including patients undergoing revision TKAs. Ten studies met the predetermined eligibility criteria and were included in this meta-analysis. The PRISMA flowchart was applied to illustrate the step-by-step selection process (Fig. 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) search flow diagram
Characteristics of the eligible studies and patients
Three RCTs [23,24,25], two observational prospective [26, 27] and five observational retrospective [6, 28,29,30,31] studies were included in this meta-analysis. A total of 962,467 patients, who underwent primary TKA with the use of either HXLPE (12.9%, N = 124,653) or conventional polyethylene (87.1%, N = 838,152) were enrolled. The mean overall duration of follow-up was 4.9 ± 1.6 years, ranging from 2 to 7 years. four studies [24, 27, 28, 30] reported separate follow-up durations for both polyethylene types, with similar mean follow-ups of 4.6 years for HXLPE and 5.02 years for conventional polyethylene. The mean patient age was 68.7 ± 5.1 (range: 60–78) years and 27.4% of the included patients were male. Significant baseline characteristics of all patients enrolled are summarized in Table 1. No study was assessed as having high risk of bias, while a detailed assessment of risk of bias for the included studies is available in Supplementary Table 2. The vast majority of the preoperative diagnosis was osteoarthritis (99.7%, N = 411,695/412,884). In two studies, [6, 27] the preoperative diagnosis is not mentioned.
All-cause Revision TKA
All 10 eligible studies [6, 23,24,25,26,27,28,29,30,31], enrolling a total of 962,467 patients, reported data on total number of revision TKAs needed during their follow-up period. The random effects model meta-analysis demonstrated no significant difference between HXLPE and conventional polyethylene group (OR 0.67; 95% CI 0.39–1.18; I2: 97.7%; P: 0.165) (Fig. 2).

Forest plot comparing total revision rates in the utilization of HXLPE and conventional polyethylene
Revision TKA for Aseptic Loosening
Data about revision TKAs due to prosthesis loosening were provided by seven studies [23,24,25,26, 28, 30, 31], enrolling a total of 411,543 patients. Patients in HXLPE group were less likely to undergo revision operation due to loosening compared to the conventional polyethylene group (OR 0.35; 95% CI 0.31–0.39; I2: 0.0%; P < 0.001) (Fig. 3).

Forest plot comparing revision rates for loosening in the utilization of HXLPE and conventional polyethylene
Radiolucent Lines
A total of 4 studies [24, 28,29,30], including 1495 patients, recorded the presence or absence of a radiolucent line. Results showed no superiority between HXLPE and conventional polyethylene in terms of this variable (OR 0.54; 95% CI 0.20–1.49; I2: 69.4%; P: 0.235) (Fig. 4). In two of the studies [29, 30] radiolucencies greater than 1 mm were taken into consideration whereas in one study [24], the threshold was greater than 2 mm. Additionally, another study [28] did not note a specific definition for radiolucency.

Forest plot comparing radiolucent lines in the utilization of HXLPE and conventional polyethylene
Discussion
Despite the success and effectiveness of TKA, aseptic loosening and osteolysis are major complications affecting long-term survival of the prostheses. This meta-analysis demonstrates that although the overall revision rates between HXLPE and conventional polyethylene were statistically similar, patients with a conventional polyethylene were more likely to be revised due to loosening. Wear of the polyethylene component in TKA continues to serve as a concern for surgeons since the particles created as a result of the wear can induce osteolysis and subsequently result in aseptic loosening, which remains a leading cause of revision TKA [15, 32]. Evidence has shown that particles generated from HXLPE are fewer due to the gamma or electron beam radiation, which increases the number of cross-links between the polymer chain [11, 33].
In THA, there have been some concerns about the biological response to polyethylene wear particles stemming from HXLPE. However, in a recent meta-analysis [34], which included 14 studies, eight of which were RCTs, it was shown that HXLPE is a more reliable choice relative to conventional liners in regards to revision rates, osteolysis, and polyethylene wear. More specifically, the authors concluded that the use of HXLPE was more effective in reducing the revision incidence caused by wear with a risk reduction of 91%, which theoretically demonstrates that HXLPE may decrease revision rates by reducing polyethylene wear and associated osteolysis [35].
The use of HXLPE in primary TKA remains controversial. The manufacturing process to produce crosslinking lowers the mechanical properties, making the polyethylene potentially more susceptible to fracture or catastrophic failure [8, 9]. In vitro studies have demonstrated reduced fracture toughness and crack propagation of highly cross-linked specimens compared with conventional polyethylene [36, 37]. It has been claimed that the additional irradiation and thermal stabilization comes with potential risks for reduced strength and fatigue resistance [38, 39]. Several case reports or case series throughout the literature describe HXLPE tibial post fracture, which is an uncommon but severe complication [38, 40,41,42]. Diamond et al. [41] reported five fracture cases from a series of 955 TKAs with an estimated post fracture frequency of 0.5%. However, the failure mechanism still remains unclear and most likely involves multiple factors like patient’s weight and activity and HXLPE material [43]. It should be noted that there are also cohort studies that presented no polyethylene post fractures [23, 28, 29, 43]. In our meta-analysis we did not have enough data available to synthesize and compare fracture or failure rates. Large scale studies with long-term follow-up are warranted to document these complications.
Moreover, the free radicals generated may lead to in vivo oxidation [44]. Because of this, there has been interest in adding Vitamin E, an antioxidant, to polyethylene liners. In vitro studies have confirmed that Vitamin E-infused polyethylene imparts higher oxidative resistance, but definitive clinical superiority has yet to be established [45, 46]. Only two studies in this review mentioned the use of Vitamin E-infused polyethylene, with one finding no difference in implant survival compared to HXLPE [26] and the other not reporting separate outcomes for Vitamin E-infused and non-infused HXLPE [31]. In the present meta-analysis, there was no difference in radiolucency between the two different types of liners, but no data directly comparing the wear rate between HXLPE and conventional liners was reported.
There are in vitro studies [47, 48] aimed at identifying the superiority of HXLPE use in TKA. In 2002, Muratoglu et al.[47] published an in vitro study simulating a tight posterior cruciate ligament balance during stair climbing. The authors compared the conventional polyethylenes with highly cross-linked ones and found that the performance of the highly cross-linked polyethylene inserts during this rigorous examination was identical to that of un-aged conventional polyethylene. Another in vitro study [48] evaluated the hypothesis of higher wear rates with highly cross-linked polyethylenes compared to unirradiated polyethylene tibial inserts. The authors conclude that during in vivo use, scratches that are generated on the femoral components are likely to produce a higher wear rate with both cross-linked and conventional polyethylene when compared to a smooth femoral component, but that this wear rate was likely to be higher with conventional polyethylene.
In a large retrospective study published from the Australian Orthopaedic Association National Joint Replacement Registry [49], Lewis et al. tried to examine if the revision rates for wear of TKA with different polyethylene types was improved with evolution of the implants. The authors report that only the Scorpio posterior stabilized (PS) to Triathlon PS comparison demonstrated any improvement in survivorship for both HXLPE and UHMWPE, compared to the comparison between Scorpio cruciate retaining (CR) to Triathlon CR, Genesis II PS to Legion PS, and Genesis II CR to Legion CR, which showed increased survival only with the use of UHMWPE.
In a previous meta-analysis published in 2016 [32], comparing HLXPE with conventional polyethylene, the authors did not find statistically significant differences between these two different types of polyethylenes. The present meta-analysis includes four additional studies, three of which were published after 2016. Additionally, the study population is a lot larger than the previous meta-analysis. Our analysis revealed a statistically significant reduction in revision due to aseptic loosening with the use of HXLPE inserts relative to the conventional ones (OR 0.35; 95% CI 0.31–0.39; I2: 0.0%; P < 0.001).
The findings of this meta-analysis should be interpreted in the context of the following limitations. First, six of the included studies were not RCTs, which limits the external validity of our results due to potential selection bias. Second, rates of polyethylene post fractures, revisions specifically for wear, and osteolysis were not reported in any studies, preventing direct assessment of these outcomes. However, aseptic loosening, which is closely associated with osteolysis, was included and revealed a significant difference between the HXLPE and conventional polyethylene groups. We were also unable to assess publication bias for outcomes of interest due to the fact that < 10 studies were synthesized for each outcome [50]. Finally, not having access to patient-level data prevented further analysis of clinical outcomes or adverse events, other than those reported in the results section.
Conclusion
In this meta-analysis of over 900,000 primary TKAs, the use of HXLPE was found to be associated with a similar overall rate of revision compared to conventional polyethylene. Furthermore, there was no difference in the presence or absence of radiolucent lines a mid-term follow-up. Notably, analysis of comparative data for 411,543 patients showed that the use of HXLPE was associated with a lower rate of revision for prosthetic aseptic loosening. This data support the routine continued use of HXLPE in primary TKA.
References
Kurtz S (2005) Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J Bone Jt Surg Am 87:1487. https://doi.org/10.2106/JBJS.D.02441
Sneag DB, Bogner EA, Potter HG (2015) Magnetic resonance imaging evaluation of the painful total knee arthroplasty. Semin Musculoskelet Radiol 19:40–48. https://doi.org/10.1055/s-0034-1396766
Sharkey PF, Lichstein PM, Shen C et al (2014) Why are total knee arthroplasties failing today–has anything changed after 10 years? J Arthroplasty 29:1774–1778. https://doi.org/10.1016/j.arth.2013.07.024
Gunston FH (1971) Polycentric knee arthroplasty: prosthetic simulation of normal knee movement. J Bone Joint Surg Br 53-B:272–277. https://doi.org/10.1302/0301-620X.53B2.272
Bracco P, Bellare A, Bistolfi A, Affatato S (2017) Ultra-high molecular weight polyethylene: influence of the chemical, physical and mechanical properties on the wear behavior. Rev Mater 10:791. https://doi.org/10.3390/ma10070791
Partridge TCJ, Baker PN, Jameson SS et al (2020) Conventional versus highly cross-linked polyethylene in primary total knee replacement: a comparison of revision rates using data from the national joint registry for England, Wales, and Northern Ireland. J Bone Jt Surg 102:119–127. https://doi.org/10.2106/JBJS.19.00031
Kurtz SM (2009) UHMWPE Biomaterials Handbook: Ultra High Molecular Weight Polyethylene in Total Joint Replacement and Medical Devices. Academic Press
Ries MD, Pruitt L (2005) Effect of cross-linking on the microstructure and mechanical properties of ultra-high molecular weight polyethylene. Clin Orthop 440:149–156. https://doi.org/10.1097/01.blo.0000185310.59202.e5
Lachiewicz PF, Geyer MR (2011) The use of highly cross-linked polyethylene in total knee arthroplasty. J Am Acad Orthop Surg 19:143–151. https://doi.org/10.5435/00124635-201103000-00003
Bragdon CR, Doerner M, Martell J et al (2013) The 2012 John Charnley Award: clinical multicenter studies of the wear performance of highly crosslinked remelted polyethylene in THA. Clin Orthop 471:393–402. https://doi.org/10.1007/s11999-012-2604-0
Mall NA, Nunley RM, Zhu JJ et al (2011) The incidence of acetabular osteolysis in young patients with conventional versus highly crosslinked polyethylene. Clin Orthop 469:372–381. https://doi.org/10.1007/s11999-010-1518-y
Calliess T, Ettinger M, Hülsmann N et al (2015) Update on the etiology of revision TKA–evident trends in a retrospective survey of 1449 cases. Knee 22:174–179. https://doi.org/10.1016/j.knee.2015.02.007
Wooley PH, Schwarz EM (2004) Aseptic loosening. Gene Ther 11:402–407. https://doi.org/10.1038/sj.gt.3302202
Abu-Amer Y, Darwech I, Clohisy JC (2007) Aseptic loosening of total joint replacements: mechanisms underlying osteolysis and potential therapies. Arthritis Res Ther 9(Suppl 1):S6. https://doi.org/10.1186/ar2170
2019 - AOANJRR. https://aoanjrr.sahmri.com/annual-reports-2019. Accessed 10 Sep 2020
Guha AR, Debnath UK, Graham NM (2008) Radiolucent lines below the tibial component of a total knee replacement (TKR)–a comparison between single-and two-stage cementation techniques. Int Orthop 32:453–457. https://doi.org/10.1007/s00264-007-0345-6
Zweymüller KA, Schwarzinger UM, Steindl MS (2006) Radiolucent lines and osteolysis along tapered straight cementless titanium hip stems: a comparison of 6-year and 10-year follow-up results in 95 patients. Acta Orthop 77:871–876. https://doi.org/10.1080/17453670610013150
Sakellariou VI, Sculco P, Poultsides L et al (2013) highly cross-linked polyethylene may not have an advantage in total knee arthroplasty. HSS J® 9:264–269. https://doi.org/10.1007/s11420-013-9352-x
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Higgins JPT, Altman DG, Gøtzsche PC et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928. https://doi.org/10.1136/bmj.d5928
Sterne JA, Hernán MA, Reeves BC et al (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919. https://doi.org/10.1136/bmj.i4919
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560. https://doi.org/10.1136/bmj.327.7414.557
Kim Y-H, Park J-W (2014) Comparison of highly cross-linked and conventional polyethylene in posterior cruciate-substituting total knee arthroplasty in the same patients. JBJS 96:1807–1813. https://doi.org/10.2106/JBJS.M.01605
Kindsfater KA, Pomeroy D, Clark CR et al (2015) In vivo performance of moderately crosslinked, thermally treated polyethylene in a prospective randomized controlled primary total knee arthroplasty trial. J Arthroplasty 30:1333–1338. https://doi.org/10.1016/j.arth.2015.02.041
Lachiewicz PF, Soileau ES (2016) Is there a benefit to highly crosslinked polyethylene in posterior-stabilized total knee arthroplasty? a randomized trial. Clin Orthop Relat Res 474:88–95. https://doi.org/10.1007/s11999-015-4241-x
Boyer B, Bordini B, Caputo D et al (2018) Is cross-linked polyethylene an improvement over conventional ultra-high molecular weight polyethylene in total knee arthroplasty? J Arthroplasty 33:908–914. https://doi.org/10.1016/j.arth.2017.10.005
Meneghini RM, Lovro LR, Smits SA, Ireland PH (2015) Highly cross-linked versus conventional polyethylene in posterior-stabilized total knee arthroplasty at a mean 5-year follow-up. J Arthroplasty 30:1736–1739. https://doi.org/10.1016/j.arth.2015.05.009
Hodrick JT, Severson EP, McAlister DS et al (2008) Highly crosslinked polyethylene is safe for use in total knee arthroplasty. Clin Orthop 466:2806–2812. https://doi.org/10.1007/s11999-008-0472-4
Minoda Y, Aihara M, Sakawa A et al (2009) Comparison between highly cross-linked and conventional polyethylene in total knee arthroplasty. Knee 16:348–351. https://doi.org/10.1016/j.knee.2009.01.005
Takemura S, Minoda Y, Sugama R et al (2019) Comparison of a vitamin E-infused highly crosslinked polyethylene insert and a conventional polyethylene insert for primary total knee arthroplasty at two years postoperatively. Bone Jt J 101-B:559–564. https://doi.org/10.1302/0301-620X.101B5.BJJ-2018-1355.R1
de Steiger RN, Muratoglu O, Lorimer M et al (2015) Lower prosthesis-specific 10-year revision rate with crosslinked than with non-crosslinked polyethylene in primary total knee arthroplasty: 386,104 procedures from the Australian Orthopaedic Association National Joint Replacement Registry. Acta Orthop 86:721–727. https://doi.org/10.3109/17453674.2015.1065046
Yu B, Yang G, Wang W et al (2016) Cross-linked versus conventional polyethylene for total knee arthroplasty: a meta-analysis. J Orthop Surg 11:39. https://doi.org/10.1186/s13018-016-0374-1
Jacobs CA, Christensen CP, Greenwald AS, McKellop H (2007) Clinical performance of highly cross-linked polyethylenes in total hip arthroplasty. JBJS 89:2779–2786. https://doi.org/10.2106/JBJS.G.00043
Shi J, Zhu W, Liang S et al (2019) Cross-linked versus conventional polyethylene for long-term clinical outcomes after total hip arthroplasty: a systematic review and meta-analysis. J Invest Surg. https://doi.org/10.1080/08941939.2019.1606370
Tsukamoto M, Mori T, Ohnishi H et al (2017) Highly cross-linked polyethylene reduces osteolysis incidence and wear-related reoperation rate in cementless total hip arthroplasty compared with conventional polyethylene at a mean 12-year follow-Up. J Arthroplasty 32:3771–3776. https://doi.org/10.1016/j.arth.2017.06.047
Bradford L, Baker D, Ries MD, Pruitt LA (2004) Fatigue crack propagation resistance of highly crosslinked polyethylene. Clin Orthop 429:68–72. https://doi.org/10.1097/01.blo.0000150124.34906.34
Cole JC, Lemons JE, Eberhardt AW (2002) Gamma irradiation alters fatigue-crack behavior and fracture toughness in 1900H and GUR 1050 UHMWPE. J Biomed Mater Res 63:559–566. https://doi.org/10.1002/jbm.10335
Hambright D, Watters T, Kaufman A et al (2010) Fracture of highly cross-linked all-polyethylene patella after total knee arthroplasty. J Knee Surg 23:237–240. https://doi.org/10.1055/s-0031-1271890
Asano T, Akagi M, Clarke IC et al (2007) Dose effects of cross-linking polyethylene for total knee arthroplasty on wear performance and mechanical properties. J Biomed Mater Res B Appl Biomater 83B:615–622. https://doi.org/10.1002/jbm.b.30835
Jung KA, Lee SC, Hwang SH, Kim SM (2008) Fracture of a second-generation highly cross-linked UHMWPE tibial post in a posterior-stabilized scorpio knee system. Orthopedics 31:1137–1139. https://doi.org/10.3928/01477447-20081101-10
Diamond OJ, Howard L, Masri B (2018) Five cases of tibial post fracture in posterior stabilized total knee arthroplasty using prolong highly cross-linked polyethylene. Knee 25:657–662. https://doi.org/10.1016/j.knee.2018.05.005
Lee W, Wee L (2019) Highly crosslinked polyethylene tibial post fracture in the unafflicted limb of a patient with unilateral lower limb poliomyelitis: a case report. Malays Orthop J 13:42–44. https://doi.org/10.5704/MOJ.1903.008
Kim Y-H, Park J-W (2020) Long-term assessment of highly cross-linked and compression-molded polyethylene inserts for posterior cruciate-substituting TKA in young patients: a concise follow-up of a previous report*. J Bone Jt Surg 102:1623–1627. https://doi.org/10.2106/JBJS.20.00261
Muratoglu OK, Bragdon CR, O’Connor DO et al (2001) A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties. Recipient of the 1999 HAP Paul Award. J Arthroplasty 16:149–160. https://doi.org/10.1054/arth.2001.20540
Kurtz SM, Dumbleton J, Siskey RS et al (2009) Trace concentrations of vitamin E protect radiation crosslinked UHMWPE from oxidative degradation. J Biomed Mater Res A 90:549–563. https://doi.org/10.1002/jbm.a.32122
Gigante A, Bottegoni C, Ragone V, Banci L (2015) Effectiveness of vitamin-E-doped polyethylene in joint replacement: a literature review. J Funct Biomater 6:889–900. https://doi.org/10.3390/jfb6030889
Muratoglu OK, Bragdon CR, O’Connor DO et al (2002) Aggressive wear testing of a cross-linked polyethylene in total knee arthroplasty. Clin Orthop. https://doi.org/10.1097/00003086-200211000-00015
Muratoglu OK, Burroughs BR, Bragdon CR et al (2004) Knee simulator wear of polyethylene tibias articulating against explanted rough femoral components. Clin Orthop. https://doi.org/10.1097/01.blo.0000143801.41885.8b
Lewis PL, Graves SE, Steiger RN, de et al (2020) Does knee prosthesis survivorship improve when implant designs change? findings from the australian orthopaedic association national joint replacement registry. Clin Orthop 478:1156–1172. https://doi.org/10.1097/CORR.0000000000001229
Sterne JAC, Sutton AJ, Ioannidis JPA et al (2011) Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 343:d4002. https://doi.org/10.1136/bmj.d4002
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The senior author is a paid consultant of Depuy Synthes, Intellijoint Surgical and EOS Imaging. The rest of the authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gkiatas, I., Karasavvidis, T., Sharma, A.K. et al. Highly cross-linked polyethylene in primary total knee arthroplasty is associated with a lower rate of revision for aseptic loosening: a meta-analysis of 962,467 cases. Arch Orthop Trauma Surg 142, 1177–1184 (2022). https://doi.org/10.1007/s00402-021-03887-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-03887-z