
Abstract
Background
Closed reduction and pinning is the accepted treatment choice for dislocated supracondylar humeral fractures in children (SCHF). Rates of open reduction, complications and outcome are reported to be dependent on delay of surgery. We investigated whether delay of surgery had influence on the incidence of open reduction, complications and outcome of surgical treatment of SCHFs in the authors’ institution.
Methods
Three hundred and forty-one children with 343 supracondylar humeral fractures (Gartland II: 144; Gartland III: 199) who underwent surgery between 2000 and 2009 were retrospectively analysed. The group consisted of 194 males and 149 females. The average age was 6.3 years. Mean follow-up was 6.2 months. Time interval between trauma and surgical intervention was determined using our institutional database. Clinical and radiographical data were collected for each group. Influence of delay of treatment on rates of open reduction, complications and outcome was calculated using logistic regression analysis. Furthermore, patients were grouped into 4 groups of delay (<6 h, n = 166; 6–12 h, n = 95; 12–24 h, n = 68; >24 h, n = 14) and the aforementioned variables were compared among these groups.
Results
The incidence of open procedures in 343 supracondylar humeral fractures was 2.6 %. Complication rates were similar to the literature (10.8 %) primarily consisting of transient neurological impairments (9.0 %) which all were fully reversible by conservative treatment. Poor outcome was seen in 1.7 % of the patients. Delay of surgical treatment had no influence on rates of open surgery (p = 0.662), complications (p = 0.365) or poor outcome (p = 0.942).
Conclusions
In this retrospective study delay of treatment of SCHF did not have significant influence on the incidence of open reduction, complications, and outcome. Therefore, in SCHF with sufficient blood perfusion and nerve function, elective treatment is reasonable to avoid surgical interventions in the middle of the night which are stressful and wearing both for patients and for surgeons.
Level of evidence
III (retrospective comparative study).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fracture of the elbow represents one of the most common fractures during childhood. Among these the incidence of supracondylar humeral fracture (SCHF) is 60–80 % [1–3]. It is the most common fracture in the age group under 7 years and the second most common fracture after 7 years [4].
Closed reduction and pin fixation is generally accepted as the treatment modality of choice for displaced fractures [5–8]. However, due to insufficient closed reduction, conversion rates to open surgery are known to reach 70 % according to the literature [9–12].
Complication rates are reported to range from 5 to 30 %, mainly consisting of transient nerve disorders, or poor outcome caused by loss of range of motion or cubitus varus; found in 0–15 % [10, 13–15].
There is some debate about the timing of the treatment of displaced supracondylar fractures. Proponents of an emergent treatment claim reduced risks of perioperative complications, easier reducibility with avoidance of opening the fracture site, and earlier hospital discharge as potential benefits [3, 16–24]. Other authors could not substantiate these possible advantages, as they found no increase in the need for open reduction or other complications with selective delay in treating these injuries [25–35].
Due to the known higher complication rates of surgery at nighttime we prefer to avoid operative interventions after midnight when possible [36–40]. The purpose of this study was to evaluate the influence of delay of surgical treatment of SCHF in children based on a retrospective analysis.
We raised the following questions: does delay of surgery in SCHF influence the rates of conversion to open surgery, complications or poor outcome?
Materials and methods
Data from patients treated for supracondylar fractures between 2000 and 2009 was retrieved from our institutional database. For retrospective anonymous evaluation of data, institutional review board approval was not necessary.
Fractures were classified by evaluating the radiographs at admission according to the Gartland classification [41].
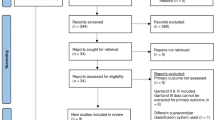
Out of 721 children suffering supracondylar humeral fractures, 352 had Gartland type I fractures or Gartland type II fractures with slight dorsal extension and were treated conservatively either by immobilisation in a cast or a Blount sling. 26 patients had to be excluded due to open fractures (n = 9), incomplete documentation (n = 8), Y-fractures (n = 8) and pathologic fractures (n = 1).
Finally 343 fractures in 341 children were treated operatively and could be included in the study.
Surgical technique
Prophylactic i.v. antibiotics were dispensed preoperatively and the anaesthetist ensured fully relaxation of the patient. Gentle manual traction disengaged the fracture fragments. Adequate mobilisation of the fragments was rechecked by fluoroscopy. Since most of the extension-type fractures were posteromedially displaced with intact medial periosteum correction was performed in the frontal plane first followed by a flexion manoeuver by pushing the olecranon forward with the thumb to correct the sagittal deformity. Full forearm pronation gave additional stability and closed the gap of the lateral ruptured periosteum. Then fixation was performed with two or three K wires (1.6–2.0 mm) either from the radial side or in a cross fashion. The K wires were not buried under the skin but left outside to enable removal in the outpatient clinic after radiographic consolidation at 4–5 weeks. For posterolateral dislocation of extension-type fractures the forearm was flexed and supinated to close the medial gap due to the ruptured periosteum on the medial side. In rare cases of flexion-type injuries the elbow was extended while a pro- or supination force was applied. If sufficient closed reduction was impossible or fixation by Kirschner wire was not stable enough a radial external fixateur was used [42].
The postoperative management protocol included a long-arm cast in 90 degree flexion of the elbow and neutral to slight supination position of the forearm for 4 weeks.
The cast was removed and healing of the fracture was proved by an anterior–posterior and lateral X-ray of the elbow. If consolidation was sufficient, K wires were removed under analgesia or analgosedation and free range of motion was allowed without activity against resistance or lifting of heavy weight for additional 4 weeks. Contact sports were prohibited until 8 weeks postoperatively. In uneventful cases, the primary physician took care of further follow-up.
If a radial external fixateur was employed no additional cast immobilisation was necessary. Removal of the fixateur was usually performed in the outpatient clinic after consolidation of the fracture 4–5 weeks postoperatively comparable to the K wire removal. The further rehabilitation followed according to the before-mentioned algorithm after K wire fixation.
Clinical records were screened for the time interval between trauma and surgery, type of reduction (open vs. closed), duration of the procedure itself, postoperative hospitalisation, complications and the need for reoperation. The neurological and vascular status before and after surgery were documented. Outcome was measured according to the Flynn criteria [43]. These define a poor outcome in case of a cubitus varus of more than 15° or motion loss of more than 15°.
Radiographic evaluation included the classification of the fracture according to the Gartland classification [41] as well as Baumann’s angle after bony healing which was measured by drawing a line perpendicular to the longitudinal axis of the humeral shaft and a line following the physeal line of the lateral condyle [44]. Values of 75° ± 7° were considered normal.
Our 0-hypothesis was that delay of treatment caused significant higher rates of open reduction, complications and poor outcome according to Flynn‘s criteria.
Logistic regression analyses were used to analyse the effect of delay of treatment on the three outcome variables. Recall bias regarding the exact time of injury might cause imprecise delay of treatment data. To mitigate this, the cohort was broken down into four groups (<6 h, n = 166; 6–12 h, n = 95; 12–24 h, n = 68; >24 h, n = 14) and the outcome variables were compared among these groups using Chi-squared test; Fisher’s exact test was used when frequency was <5. Two-tailed Student’s t test and one-way ANOVA were used for comparison of continuous data. Each analysis was separately performed for all fractures, grade II fractures, and grade III fractures.
A p value <0.05 was considered statistically significant. Statistical analysis was performed with SPSS 22.0 (SPSS Institute, Chicago, IL, USA).
Results
No difference in demographics, postoperative follow-up period, duration of procedure, and duration of postoperative hospital stay was found among the delay groups (Table 1). Baumann’s angle was found to significantly different among the groups and post hoc analysis showed that this difference was caused by a higher value in the <6 h group as compared to the 6–12 h group (p = 0.004) whereas no difference was found among all other groups (p > 0.05). However, as this difference was only 1.7 degrees with both the sub 6-h group and the 6–12 h group being within normal limits, the clinical relevance was negligible. Of note, higher proportions of Gartland grade III fractures were found in the earlier treatment groups (p < 0.01).
38 (10.8 %) patients had documented neurological symptoms preoperatively affecting the median nerve in 16 cases, the ulnar nerve in seven cases, the radial nerve in five cases and mixed paresthesia in nine patients. These patients were treated according to the routine surgical protocol as mentioned above. All neurological symptoms resolved after surgery. There was no difference in the delay of treatment between the patients with and without preoperative neurological impairment (Table 2).
Nine (2.6 %) out of 343 fractures underwent open reduction. Indication for open reduction was entrapment of the joint capsule in five cases. In four patients the surgical report did not mention what impeded closed reduction. All open reductions were performed in patients with a type III fracture while all type II fractures could be reduced by closed means.
Complications occurred in 37 (10.8 %) patients including 31 (9.0 %) postoperative nerve disorders, one early reoperation and five pin tract infections. The postoperative neurological symptoms affected the ulnar nerve in 17 cases, the median nerve in seven cases, and the radial nerve in seven cases. All nerve disorders resolved completely in the first weeks following surgery. Due to insufficient fracture reduction, one patient required early revision during initial hospital stay. This revision was performed by closed reduction. All patients suffering from Pin tract infections were treated successfully with antibiotics; osteomyelitis was not encountered. Thirty of these complications occurred in type III fractures (15.1 %) and seven in type II fractures (4.9 %). There was no significant difference in rate of complications between closed or open reduction of Gartland III fractures (28 out of 190 vs. 1 out of 9, p = 0.613).
Poor outcome according to Flynn criteria was seen in six patients. Five patients had mild cubitus varus. Another patient had significant loss of range of motion. Four patients with grade III fractures and two patients with grade II fractures had poor outcome. No patient required a correction osteotomy after a mean follow-up of 2.4 years.
Logistic regression analyses revealed that a higher patient age at time of surgery was associated with a higher risk for complications in the entire cohort and in grade III fractures (p = 0.040, odds ratio 1.146, 95 % confidence 1.001–1.305 for entire cohort; p = 0.035, odds ratio 1.171, 95 % confidence 1.011–1.356 in grade III fractures). Otherwise, no prognostic factor for necessary open reduction or poor outcome was found and the delay of treatment had no influence on either of the three outcome variables (Table 3).
No difference in rates of open reduction, complications, and poor outcome was found when comparing the patients treated before and after 6, 12 and 24 h (Table 4).
Discussion
Timing of the treatment of displaced supracondylar humeral fractures (SCHF) is controversially discussed in literature.
Proponents of emergent treatment claim reduced risks of perioperative complications, easier reducibility with avoidance of opening the fracture site, and earlier hospital discharge [3, 16–24] as potential benefits. Walmsley reported higher rates of conversion to open reduction when treatment of SCHF was delayed more than 8 h in 171 patients with Gartland type III fractures. In this series, 11 % of the early treated and 33 % of the delayed treated patients underwent open reduction. In a study by Yildirim et al. rates of open reduction even increased to 74 % when treatment was performed 15–32 h after trauma and 100 % when delay was 32 h or more [12]. A systematic review by Loizou et al. [24] including five studies found a significantly higher rate of open reduction of 22.9 % when postponing treatment of Gartland type III fractures. However, these series’ showed very high rates of open reduction compared to our series with 4.5 %.
In a multicenter study Ramachandran identified 11 patients who developed a compartment syndrome after closed, low-energy SCHF. The authors assumed that the delay in surgical treatment of 22 h could have contributed to the complications in these patients [22].
Recent studies comparing results dependent on treatment delays of 8 h [26–28, 35, 45], 12 h [29, 31, 32, 34] or 21 h [13] are in line with our study. These studies did not find differences in rates of open reduction [13, 26–29, 31, 32, 34], nerve injuries [28, 29, 31, 34, 45], unsatisfactory outcome [13, 26], infections [28, 29, 31, 34], vascular complications [29], duration of surgical procedure [26], duration of postoperative hospitalisation [26] and quality of reduction measured by multiple radiological parameters [35]. However, some of these studies do not present separate analyses of Gartland type III fractures [28, 34, 45].
Regarding Gartland type II fractures even longer delays seem acceptable as Larson et al. [33] did not report an increased rate of complications when postponing treatment for more than 24 h. Silva et al. reported about 42 Gartland type II fractures treated surgically with a delay of more than 7 days without necessity of open reductions and identical final carrying angle and range of motion compared to 101 fractures treated within 7 days [46].
Consistent to our findings several series had higher rates of severe fractures in the early treated group [28, 31, 34, 45], indicating that more severe fractures tend to be treated more urgently. Accordingly, Garg et al. [31] found a trend to a steady decrease in morbidity and complication rates with increased time to surgery and they described this to a possible selection bias caused by expeditious treatment of more severe fractures.
Further prognostic factors including the level of the fracture and the patient age at time of surgery have been proved important. Kang et al. [47] revealed that fractures below the humeral isthmus are associated with poor outcome after surgical treatment. Commonly used classification systems as the classifications according to Gartland [41], Baumann [48], Lagrange and Rigault [49] or the AO Pediatric Comprehensive Classification of Long Bone Fractures [50] do not lay stress on the fracture level and therefore do not detect this prognostic factor. In the study of Kang age over 10 years at time of surgery was associated with poor outcome and with low-level fractures. In the presented study the influence of the patient’s age was confirmed as this was the only prognostic factor for a higher rate of complications to be found in the logistic regression analysis.
Our results showed no influence of delay of surgical treatment of more than 6, 12 or 24 h regarding need for open reduction, complications and poor outcome. The strength of the study is the high number of patients involved compared to most of the studies dealing with this topic.
This study has some limitations: the main limitation of the study is its retrospective design, which is more susceptible to bias compared to a prospective study design. The higher proportion of type III fractures in the earlier treatment groups might reflect such a bias, as surgeons possibly decided to treat type III fractures more urgent than type II fractures.
Another limitation might be the short follow-up time. The average follow-up in our study is 6 months. This is comparable to other publications dealing with the outcome of SCHF. As mentioned above all patients were followed until neurological symptoms had fully recovered. Since varus malalignment is a consequence of poor reduction or loss of reduction it can be noted immediately postoperatively. The same applies for vascular compromise [7]. Therefore, we believe that a longer period of follow-up would not change the quality of the results of this study.
The purpose of this study is not to generally support delayed treatment of supracondylar humeral fractures. The authors are aware that in particular cases e.g. in open fractures or severe dislocation with uncontrollable pain or absent distal perfusion surgery has to be performed immediately.
Fortunately, most patients suffer a closed injury and show a normal neurovascular examination on the affected extremity without risk for skin breakdown due to fracture fragments. Usually, if immobilized in a cast, pain management is unproblematic. Since many supracondylar humeral fractures happen in the late afternoon, immediate surgery often is not possible for lack of instant availability of an operation room and the surgery has to be executed after midnight. For the surgeon and the treatment team as well as for the patient (e.g. long time without eating and drinking) this situation is wearing. Under these circumstances we recommend delayed surgical treatment in an elective fashion on the following day.
Conclusion
In the presented retrospective study delay of treatment of SCHF in children, did not have significant influence on rates of open reduction, complications, and poor outcome, respectively. Therefore, in SCHF in children with intact distal perfusion and intact nerve function an elective treatment is reasonable to avoid surgical interventions in the middle of the night which are stressful and wearing both for patients and surgeons.
References
Beaty JH (2003) Elbow fractures in children and adolescents. Instr Course Lect 52:661–665
Houshian S, Mehdi B, Larsen MS (2001) The epidemiology of elbow fracture in children: analysis of 355 fractures, with special reference to supracondylar humerus fractures. J Orthop Sci 6(4):312–315. doi:10.1007/s0077610060312
Otsuka NY, Kasser JR (1997) Supracondylar Fractures of the Humerus in Children. J Am Acad Orthop Surg 5(1):19–26
Cheng JC, Lam TP, Shen WY (1995) Closed reduction and percutaneous pinning for type III displaced supracondylar fractures of the humerus in children. J Orthop Trauma 9(6):511–515
Omid R, Choi PD, Skaggs DL (2008) Supracondylar humeral fractures in children. J Bone Joint Surg Am 90(5):1121–1132. doi:10.2106/JBJS.G.01354
Pirone AM, Graham HK, Krajbich JI (1988) Management of displaced extension-type supracondylar fractures of the humerus in children. J Bone Joint Surg Am 70(5):641–650
Ponce BA, Hedequist DJ, Zurakowski D, Atkinson CC, Waters PM (2004) Complications and timing of follow-up after closed reduction and percutaneous pinning of supracondylar humerus fractures: follow-up after percutaneous pinning of supracondylar humerus fractures. J Pediatr Orthop 24(6):610–614 00004694-200411000-00002 [pii]
Reynolds RA, Jackson H (2005) Concept of treatment in supracondylar humeral fractures. Injury 36(Suppl 1):A51–A56. doi:10.1016/j.injury.2004.12.013
Colaris JW, Horn TM, van den Ende ED, Allema JH, Merkus JW (2008) Supracondylar fractures of the humerus in children. Comparison of results in two treatment periods. Acta Chir Belg 108(6):715–719
von Laer L, Gunter SM, Knopf S, Weinberg AM (2002) Supracondylar humerus fracture in childhood—an efficacy study. Results of a multicenter study by the Pediatric Traumatology Section of the German Society of Trauma Surgery–II: costs and effectiveness of the treatment. Unfallchirurg 105(3):217–223
Weinberg AM, Marzi I, Gunter SM, Wessel L, Riedel J, von Laer L (2002) Supracondylar humerus fracture in childhood—an efficacy study. Results of a multicenter study by the Pediatric Traumatology Section of the German Society of Trauma Surgery–I: epidemiology, effectiveness evaluation and classification. Unfallchirurg 105(3):208–216
Yildirim AO, Unal VS, Oken OF, Gulcek M, Ozsular M, Ucaner A (2009) Timing of surgical treatment for type III supracondylar humerus fractures in pediatric patients. J Child Orthop 3(4):265–269. doi:10.1007/s11832-009-0189-2
Bales JG, Spencer HT, Wong MA, Fong YJ, Zionts LE, Silva M (2010) The effects of surgical delay on the outcome of pediatric supracondylar humeral fractures. J Pediatr Orthop 30(8):785–791. doi:10.1097/BPO.0b013e3181f9fc03
Farley FA, Patel P, Craig CL, Blakemore LC, Hensinger RN, Zhang L, Caird MS (2008) Pediatric supracondylar humerus fractures: treatment by type of orthopedic surgeon. J Child Orthop 2(2):91–95. doi:10.1007/s11832-008-0089-x
O’Hara LJ, Barlow JW, Clarke NM (2000) Displaced supracondylar fractures of the humerus in children. Audit changes practice. J Bone Joint Surg Br 82(2):204–210
Giannini S, Maffei G, Girolami M, Ceccarelli F (1983) The treatment of supracondylar fractures of the humerus in children by closed reduction and fixation with percutaneous Kirschner wires. Ital J Orthop Traumatol 9(2):181–188
Jacobs RL (1967) Supracondylar fracture of the humerus in children. IMJ Ill Med J 132(5):696–701
Minkowitz B, Busch MT (1994) Supracondylar humerus fractures. Current trends and controversies. Orthop Clin North Am 25(4):581–594
Paradis G, Lavallee P, Gagnon N, Lemire L (1993) Supracondylar fractures of the humerus in children. Technique and results of crossed percutaneous K-wire fixation. Clin Orthop Relat Res 297:231–237
Segal D (1979) Pediatric orthopedic emergencies. Pediatr Clin North Am 26(4):793–802
Walmsley PJ, Kelly MB, Robb JE, Annan IH, Porter DE (2006) Delay increases the need for open reduction of type-III supracondylar fractures of the humerus. J Bone Joint Surg Br 88(4):528–530. doi:10.1302/0301-620X.88B4.17491
Ramachandran M, Skaggs DL, Crawford HA, Eastwood DM, Lalonde FD, Vitale MG, Do TT, Kay RM (2008) Delaying treatment of supracondylar fractures in children: has the pendulum swung too far? J Bone Joint Surg Br 90(9):1228–1233. doi:10.1302/0301-620X.90B9.20728
Keon-Cohen BT (1966) Fractures at the elbow. J Bone Joint Surg Am 48(8):1623–1639
Loizou CL, Simillis C, Hutchinson JR (2009) A systematic review of early versus delayed treatment for type III supracondylar humeral fractures in children. Injury 40(3):245–248. doi:10.1016/j.injury.2008.07.031
Carmichael KD, Joyner K (2006) Quality of reduction versus timing of surgical intervention for pediatric supracondylar humerus fractures. Orthopedics 29(7):628–632
Leet AI, Frisancho J, Ebramzadeh E (2002) Delayed treatment of type 3 supracondylar humerus fractures in children. J Pediatr Orthop 22(2):203–207
Iyengar SR, Hoffinger SA, Townsend DR (1999) Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: a comparative study. J Orthop Trauma 13(1):51–55
Mehlman CT, Strub WM, Roy DR, Wall EJ, Crawford AH (2001) The effect of surgical timing on the perioperative complications of treatment of supracondylar humeral fractures in children. J Bone Joint Surg Am 83-A(3):323–327
Gupta N, Kay RM, Leitch K, Femino JD, Tolo VT, Skaggs DL (2004) Effect of surgical delay on perioperative complications and need for open reduction in supracondylar humerus fractures in children. J Pediatr Orthop 24(3):245–248 00004694-200405000-00001 [pii]
Sibinski M, Sharma H, Bennet GC (2006) Early versus delayed treatment of extension type-3 supracondylar fractures of the humerus in children. J Bone Joint Surg Br 88(3):380–381. doi:10.1302/0301-620X.88B3.17181
Garg S, Weller A, Larson AN, Fletcher ND, Kwon M, Schiller J, Browne R, Copley L, Ho C (2014) Clinical characteristics of severe supracondylar humerus fractures in children. J Pediatr Orthop 34(1):34–39. doi:10.1097/BPO.0b013e31829c0046
Kronner JM Jr, Legakis JE, Kovacevic N, Thomas RL, Reynolds RA, Jones ET (2013) An evaluation of supracondylar humerus fractures: is there a correlation between postponing treatment and the need for open surgical intervention? J Child Orthop 7(2):131–137. doi:10.1007/s11832-013-0482-y
Larson AN, Garg S, Weller A, Fletcher ND, Schiller JR, Kwon M, Browne R, Copley LA, Ho CA (2014) Operative treatment of type II supracondylar humerus fractures: does time to surgery affect complications? J Pediatr Orthop 34(4):382–387. doi:10.1097/bpo.0000000000000124
Mayne AI, Perry DC, Bruce CE (2014) Delayed surgery in displaced paediatric supracondylar fractures: a safe approach? Results from a large UK tertiary paediatric trauma centre. Eur J Orthop Surg Traumatol Orthop Traumatol 24(7):1107–1110. doi:10.1007/s00590-013-1292-0
Murnaghan ML, Slobogean BL, Byrne A, Tredwell SJ, Mulpuri K (2010) The effect of surgical timing on operative duration and quality of reduction in Type III supracondylar humeral fractures in children. J Child Orthop 4(2):153–158. doi:10.1007/s11832-010-0240-3
Chacko AT, Ramirez MA, Ramappa AJ, Richardson LC, Appleton PT, Rodriguez EK (2011) Does late night hip surgery affect outcome? J Trauma 71(2):447–453. doi:10.1097/TA.0b013e3182231ad7 (Discussion 453)
Eastridge BJ, Hamilton EC, O’Keefe GE, Rege RV, Valentine RJ, Jones DJ, Tesfay S, Thal ER (2003) Effect of sleep deprivation on the performance of simulated laparoscopic surgical skill. Am J Surg 186(2):169–174
Kelz RR, Freeman KM, Hosokawa PW, Asch DA, Spitz FR, Moskowitz M, Henderson WG, Mitchell ME, Itani KM (2008) Time of day is associated with postoperative morbidity: an analysis of the national surgical quality improvement program data. Ann Surg 247(3):544–552. doi:10.1097/SLA.0b013e31815d7434
Ricci WM, Gallagher B, Brandt A, Schwappach J, Tucker M, Leighton R (2009) Is after-hours orthopaedic surgery associated with adverse outcomes? A prospective comparative study. J Bone Joint Surg Am 91(9):2067–2072. doi:10.2106/JBJS.H.00661
Rothschild JM, Keohane CA, Rogers S, Gardner R, Lipsitz SR, Salzberg CA, Yu T, Yoon CS, Williams DH, Wien MF, Czeisler CA, Bates DW, Landrigan CP (2009) Risks of complications by attending physicians after performing nighttime procedures. JAMA 302(14):1565–1572. doi:10.1001/jama.2009.1423
Gartland JJ (1959) Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet 109(2):145–154
Slongo T, Schmid T, Wilkins K, Joeris A (2008) Lateral external fixation—a new surgical technique for displaced unreducible supracondylar humeral fractures in children. J Bone Joint Surg Am 90(8):1690–1697. doi:10.2106/JBJS.G.00528
Flynn JC, Matthews JG, Benoit RL (1974) Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years’ experience with long-term follow-up. J Bone Joint Surg Am 56(2):263–272
Baumann E (1960) Zur Behandlung der Knochenbrüche am Ellbogengelenk. Langenbecks Arch Chir 295(1):300–304
Cashman JP, Guerin SM, Hemsing M, McCormack D (2010) Effect of deferred treatment of supracondylar humeral fractures. Surgeon 8(2):71–73. doi:10.1016/j.surge.2009.10.011
Silva M, Wong TC, Bernthal NM (2011) Outcomes of reduction more than 7 days after injury in supracondylar humeral fractures in children. J Pediatr Orthop 31(7):751–756. doi:10.1097/BPO.0b013e31822f16e5
Kang S, Kam M, Miraj F, Park SS (2015) The prognostic value of the fracture level in the treatment of Gartland type III supracondylar humeral fracture in children. Bone Joint J 97-B(1):134–140. doi:10.1302/0301-620x.97b1.34492
Baumann E (1965) Spezielle Frakturen-und Luxationslehre: Ellbogen/Bearb. von Ernst Baumann. Thieme, Stuttgart
Lagrange J, Rigault P (1962) Les fractures de l’extrémité inférieure de l’humérus de l’enfant. Rev Chir Orthop 48:334–414
Slongo TF, Audige L (2007) Fracture and dislocation classification compendium for children: the AO pediatric comprehensive classification of long bone fractures (PCCF). J Orthop Trauma 21(10 Suppl):S135–S160 00005131-200711101-00020 [pii]
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Schmid, T., Joeris, A., Slongo, T. et al. Displaced supracondylar humeral fractures: influence of delay of surgery on the incidence of open reduction, complications and outcome. Arch Orthop Trauma Surg 135, 963–969 (2015). https://doi.org/10.1007/s00402-015-2248-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2248-0