
Abstract
Objective
The aim of this study was to investigate the association between the consumption of foods and drinks from different food processing categories using the NOVA classification and CRC risk among Moroccan adults.
Methods
1453 cases and 1453 matched controls aged at least 18 years and recruited from the 5 greater Moroccan regions were interviewed by trained investigators about their habitual diet using a standardized food frequency questionnaire (FFQ). Foods were categorized according to their degree of processing by the NOVA classification. Intakes of each food processing group were categorized into tertiles based on the distribution of controls with the lowest tertile considered as the reference category. Multivariable conditional logistic regression models were used to assess the association between each group and CRC risk (Odds Ratio (OR) and 95% Confidence Intervals (CI)), taking relevant confounders into account.
Results
High consumption of unprocessed or minimally processed foods (NOVA group 1) was significantly inversely (OR = 0.82, 95%CI = 0.72–0.93), while high consumption of ultra-processed foods and drink products (NOVA group 4) was significantly positively (OR = 1.40, 95% CI = 1.22–1.61) associated with CRC risk as compared to the lowest intake group. These results were similar for colon and rectum sub-sites.
Conclusion
This is the first study to evaluate the association between the NOVA classification groups and CRC risk in an African country. Our results suggest that the consumption of ultra-processed foods and drink products may be associated with an increased risk of developing CRC, but longitudinal studies are needed to confirm these results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of colorectal cancer (CRC) is strongly related with economic growth and human development in countries undergoing an epidemiological transition [1]. According to the global cancer observatory, the age-standardized incidence rate in North African countries was about 9.2 per 100 000 in 2018 [2]. Major risk factors for CRC are dietary and lifestyle behaviors [3], especially red and processed meat consumption, obesity and sedentary behavior [3, 4].
During the last decades, dietary habits have changed considerably in North African countries [5, 6]. The traditional diet has been replaced by a modern dietary pattern [7, 8]. This shift coincided with increased rates of non-communicable diseases (NCDs), including CRC [9].
Morocco is a North African low–middle-income country, passing through the third phase of its epidemiological transition [10] that was linked to rapid urbanization, and demographic growth. Dietary habits have changed considerably during the last decade, typically characterized by an increase in industrial processing of foods to make them more convenient and palatable. Recently, a new food classification system called NOVA was developed [11] with the aim to categorize all foods depending on the extent and purpose of food processing [11]. NOVA defines the following four food processing groups: unprocessed or minimally processed foods, processed culinary ingredients, processed foods, and ultra-processed foods (UPF) and drink products [12].
This nutrition transition with a steady increase in UPF consumption was accompanied by increased rates of NCDs [7]. Accumulating evidence suggests ultra-processed food intake is associated with obesity [13,14,15,16,17] and other adverse health outcomes [18, 19]. Several recent studies have examined the link between UPF consumption and obesity [20,21,22]. A high consumption of UPF is potentially related to gain in BMI and higher risks of overweight and obesity [17], and its indicators (abdominal obesity) [14]. According to a systematic review of prospective studies, higher BMI and WC levels were positively associated with CRC risk [23]. Analyses stratified by anatomical site revealed that higher BMI and WC levels increased the risk of colon (proximal colon and distal colon) and rectal cancer [23]. The main mechanisms that could explain the potential effect of obesity on the risk of cancer are higher levels of circulating insulin [24] and Insulin-like Growth Factors (IGFs) which promote cellular proliferation [25].
A recent study confirmed the association between a diet rich in processed meat and CRC risk in Morocco [26]. In the last years, processed foods have dominated the food supply in high-income countries and their consumption steadily increases in middle and low-income countries (LMICs) [12]. The industrial food processing procedures that use food additives, and often generate food processing compounds such as trans-fatty acids or acrylamide, together with the high energy content of these products are expected to affect human health [27]. In fact, a recent prospective study has indicated that UPF consumption is associated with higher overall cancer risk [28].
Little information is currently available about UPF and non-communicable diseases including lifestyle-related cancers, such as CRC in LMICs. To our knowledge, this study is the first to evaluate the association between the NOVA classification and CRC risk in Africa, based on a large Moroccan case–control study.
Methods
Study population
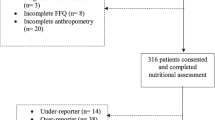
The detailed protocol of our case–control study was published before [29]. In summary, we invited 1555 newly diagnosed cases and 2000 matched controls. CRC cases and controls were individually matched on age (± 5 years), sex, and center. The ratio of CRC cases to controls was 1:1. All cases were recruited from five Moroccan university hospitals located at Rabat, Casablanca, Oujda, Fez, and Marrakech. Controls were recruited among healthy subjects accompanying other patients especially outpatients and visitors, from the same local population and in the same hospitals as the cases. Of those who were invited, 97.5% (1516/1555) of the cases and 75.8% (1516/2000) of the controls were willing to participate. Exclusion criteria prior to starting statistical analysis included: participants with unspecified primary cancer (n = 7), cases with old biopsies (six cases), participants with missing dietary data, because the FFQ was not completed (n = 10), duplicate records (n = 2), unmatched records (n = 8) and participants with the lowest and highest 1% of the distribution of the ratio between energy intake and energy requirement (n = 30), according to the exclusion criteria used in the EPIC study. We finally included 1453 newly diagnosed cases and 1453 matched controls for statistical analyses. The ethical committee of Fez has approved the study protocol.
Data collection
Socio-demographic characteristics (age, sex, marital status, area of residency, educational level, and monthly family income), and lifestyle indicators (such as tobacco consumption, and physical activity that included usual daily physical activity, and leisure-time) were collected by trained interviewers.
To assess usual dietary habits of the past year, in cases before complaints occurred, participants were questioned during a face-to-face interview using a validated semi-quantitative food frequency questionnaire, taking into account seasonal variations [30]. Participants’ answers were converted into average daily intake per day according to the frequency and portion size of each food item. Energy and nutrient intakes were calculated by matching the foods consumed with a recently compiled food composition table (FCT) for the Moroccan population [31]. The Moroccan FCT was completed using an indirect approach based on existing FCTs, in particular Moroccan and Tunisian FCTs for traditional foods. Additional information on modern foods was gathered from other databases, such as the Food Composition Table for African countries, the French Food Composition Table (CIQUAL) and the United States Department of Agriculture Nutrient Database (USDA).
NOVA classification
We classified all food items derived from our Moroccan FFQ into one of the four food groups according to the NOVA classification [11].
Group 1 includes unprocessed or minimally processed foods namely, grains, legumes, starchy roots and tubers, poultry, fish and seafood, eggs, milk and traditional dairy products (natural fermented milk such as raib, lben, and jben), meat prepared without additives or synthetic compounds (beef, lamb, rabbit, pork, camel, kebab), traditionally prepared meat (kaddid, khlii), fresh fruits and vegetables.
Group 2 includes processed culinary ingredients namely salted butter, sugar, syrup, honey, and vegetables oils.
Group 3 includes processed foods namely freshly made breads, canned fish, fruits in syrup, cheeses, dried and salted meats, and alcoholic drinks.
Group 4 includes UPF namely carbonated drinks, sweets, packaged snacks, ice-cream, chocolate, candies (confectionery), cookies (biscuits), pastries, cakes, and cake mixes, industrially processed fruit drinks, processed meat, and pre-prepared pizza.
We classified each food into one of the four cited groups, and calculated the total consumption of each NOVA group as the sum of all foods within each group in grams per day. In addition, the energy intake derived from each NOVA group was then calculated for each participant by summing energy intake from each classified food in each NOVA group. In addition, the sum of NOVA group 1 + 2 was also analyzed as foods of NOVA group 2 are typically consumed with foods from NOVA group 1.
Each NOVA group was categorized into tertiles based on the distribution of controls (daily consumption by gram and kcal) with the lowest tertile considered as the reference category.
As a matter of sensitivity analyses, the (ultra-) processed NOVA categories (NOVA groups 3 and 4) have also been calculated without considering alcoholic drinks.
Statistical analysis
For descriptive statistics, mean ± standard deviation (SD) and percentages were used. To compare cases and controls, we used t test for paired samples for continuous variables and chi-squared (χ2) for categorical variables.
The normality of the distribution of NOVA food groups was evaluated by computing the Kolmogorov–Smirnov test. Log-transformations have been used to improve normality; however, all nutritional variables were not normally distributed, even after log-transformation. Thus, the analyses were performed without log-transformation using the Wilcoxon signed-rank test.
Conditional logistic regression analyses were used to compute odds ratios and associated 95% confidence intervals (CI) and to estimate the association between each NOVA group (daily consumption in grams and kilocalories) and CRC risk overall and by anatomic location (colon, rectum separately). A brut model (unadjusted odds ratio) was used as well as a multivariable model adjusted for potential confounders, which included age (years), education level (illiterate, primary, secondary, higher), smoking status (never smoker, ex-smoker and current smoker), family history of CRC (yes, no), energy intake (except for consumption calculated in gram), and physical activity (based on 10% change in the OR). Each NOVA class was mutually adjusted for the other classes.
Statistical analyses were performed with SPSS software (Statistic Package for Social Sciences) version 20.
Results
Characteristics of the study population, including intake of NOVA classified food groups are shown in Table 1. Cases were more likely to be smokers and to have a higher occurrence of family history of CRC compared to controls. No statistical differences were observed between cases and controls for marital status and energy intake. Concerning the NOVA classification, means of unprocessed foods and processed culinary ingredients and of fiber intake were higher among controls than among cases. In addition, cases show a higher daily intake of processed and UPF and drink products compared to controls.
As shown in Table 2, compared with the lowest tertile, controls in the highest tertile of UPF intake tended to be more frequently male, younger, with more family history of cancer and a moderate physical activity level. Additionally, they had higher intakes of energy, carbohydrates and lipids.
Table 3 presents the unadjusted and adjusted OR and confidence intervals for colon, rectal and overall CRC for each NOVA classification group (g/day). An increase in the consumption of unprocessed or minimally processed foods (NOVA group 1) decreased the risk of colon cancer (ORT3 vs. T1 = 0.82, 95%CI = 0.69–0.99), rectal cancer (ORT3 vs. T1 = 0.81, 95%CI = 0.68–0.99) and CRC overall (ORT3 vs. T1 = 0.82, 95%CI = 0.72–0.93) when comparing high intakes (third tertile) versus low intakes (first tertile). A significant inverse association was also observed between the high category of group 1 and group 2 (sum) and rectal cancer and overall CRC risk (see Table S1). A positive association was observed between a high consumption of UPF and drink products (NOVA group 4) and risk of colon cancer, rectal cancer, and CRC overall, (OR = 1.36, 95%CI = 1.12–1.66; OR = 1.44, 95%CI = 1.18–1.76; OR = 1.40, 95% CI = 1.22–1.61, respectively) when comparing high intakes (third tertile) versus low intakes (first tertile).
As shown in Table S2, a positive association was also observed between total energy intake of ultra-processed foods and overall CRC risk after adjustment for confounding factors (OR T3 vs. T1 = 1.16, 95%CI = 1.01–1.33) when comparing high versus low intakes.
Discussion
The present case–control study investigated associations between food processing categories, presented as the four NOVA classification groups, and CRC risk. Our results indicated that after adjustment for potential confounding factors, a high consumption of unprocessed and minimally processed foods (NOVA group 1) may play a protective role against risk of colon cancer, rectal cancer and CRC overall. Conversely, a statistically significant increase in overall CRC risk and the different subtypes was seen for higher consumption of UPF and drink products (NOVA group 4). To our knowledge, this is the first case–control study performed in a LMIC that evaluated the association between the NOVA classification groups and overall and anatomic subtypes of CRC.
Except for one French cohort study [28], no other studies to date have evaluated associations between the NOVA classification groups and CRC risk. This prospective French study concluded that high consumption of UPF (highest versus lowest quartile) tended to increase the risk of CRC, although the association was not statistically significant [28].
Ultra-processing is a complex set of industrial processes and added ingredients and additives, where the types and extent of processing and the types and amounts of added compounds vary greatly from product to product. In addition, food processing increases the palatability of foods by several biological and chemical mechanisms, stimulating overconsumption [32]. Several hypotheses could explain negative health effects of UPF. According to the literature, UPF is rich in energy, sodium, added fat, and sugar while often poor in all beneficial and nutritious components such as dietary fiber, calcium, vitamin D and magnesium [33, 34]. The detrimental components including added fat, sodium and sugar could induce alterations to the intestinal microbiota [34,35,36]. The intestinal microbiota has been identified as a key player in several diseases such as CRC, inflammatory bowel disease, and obesity [37]. There is some evidence that perturbations in microbiota composition and activity contribute to the development of CRC in inflammatory bowel disease patients by triggering and maintaining colonic mucosal inflammation [37]. Inflammation in the large intestine can be triggered by abnormal bacterial microflora or homeostasis, resulting in mucosal damage and, eventually, the development of neoplastic lesions [38, 39]. In addition, UPF may be rich in additives; while for some additives, carcinogenic properties have been suggested [40, 41], other additives such as emulsifiers, saccharin, and maltodextrin are frequently non-absorbed and thus will likely directly interact with the microbiota in ways that promoted chronic intestinal inflammation or increased bacterial translocation [42, 43]. Also, food processing components like trans-fatty acids and acrylamide, typically generated during industrial processing may play a mutagenic role [44].
Recent evidences have highlighted effect of UPF on the telomere length and DNA damage. A Spanish study concluded that higher consumption of UPF was associated with the risk of having shorter telomeres, which are markers of biological age that may be affected by dietary factors through oxidation and inflammation mechanisms [45]. Another study showed that higher consumption of UPF is associated with greater DNA damage, which was calculated using urinary levels of 8-hydroxy-2'-deoxyguanosine, as biomarker of oxidative DNA damage [46].
In our study, CRC cases (15.8%) were more obese than controls (8.7%). A large body of evidence from meta-analyses, systematic review, and prospective studies has shown that CRC risk is associated with overweight and obesity [23, 47, 48]. In the NutriNet-Santé cohort study, including 110 260 adults followed in France for 10 years (2009–2019), authors concluded that UPF consumption is positively associated with the risk of overweight (HR for 10% absolute increase: 1.11, (95% CI: 1.08–1.14) and obesity (HR for 10% absolute increase: 1.09, (95% CI: 1.05–1.13) after adjusting for all confounding factors [17]. The mechanisms that underpin the link between obesity and CRC are unknown. The most studied factors are the insulin/insulin-like growth factor (IGF) axis and adipokines (adiponectin and leptin) [23]. A new study assessed global sales trends for UPF and sweetened sugar beverages (SSB) and their associations with the prevalence of overweight and obesity found that sales of UPF and SSB have a significant impact on BMI changes, namely predicted obesity [49]. Sales were highest in high-income countries but they were increasing more rapidly in low- and lower–middle-income countries [49].
Our study results, reported in this publication, demonstrate that a high consumption of unprocessed or minimally processed foods may have a protective effect against CRC risk. This finding could potentially be explained by the high fiber intake observed in controls and by the composition of unprocessed foods that are typically rich in folic acid, selenium, magnesium and with higher omega-3 PUFA to omega-6 PUFA ratio and with a lower energy content [50]. In addition, the absence of chemicals (such as additives and processing contaminants) in the unprocessed foods may potentially also explain this inverse relationship with CRC risk. Although the mechanisms by which unprocessed foods may exert a protective effect against CRC risk are suggested to be due to the anti-carcinogenic or antioxidant effects of dietary fibers and phenolic compounds, respectively [51, 52]. Hypothetically, also unprocessed dairy products, such as raw milk, may be decreasing cancer risk as these contain higher levels of multifunctional cytokines such as TGF-β2 and TGF-β1 isoforms which play a principal role in the development of the mucosal human immune system [53, 54]. In addition, an inverse association for traditionally processed meat products (a component of the unprocessed food group) was reported recently in relation to CRC risk [26]. An experimental study tried to explain the mechanisms behind the protective effect of traditionally processed meat and how these may reduce polyps related to CRC risk [55]. They concluded that traditionally processed meat products could potentially be redesigned towards functional prebiotic foods for preventing CRC risk in humans [55].
Major strengths in the present study are our large sample size, the high participation rate and the spread over the five different greater university hospitals that receive a significant proportion of the Moroccan population. Therefore, we consider our results representative of both, CRC patients and the general population. Furthermore, some potential limitations of this study should be mentioned. Our FFQ specially adapted to the Moroccan diet captures the usual intake of foods over a longer period of time. Differential recall bias, may be expected when the diet is influenced by gastro-intestinal complaints of the cases. To overtake this limitation, trained interviewers were recruited to ensure the proficient completion of FFQ administration and probing for more details whenever needed.
Conclusion
In conclusion, our study shows that higher consumption of unprocessed or minimally processed foods may have protective effects against CRC risk. In contrast, UPF and drinks are showing a positive association with overall CRC risk and with its different subtypes. Further research should examine the mechanisms involved to allow targeted prevention strategies (e.g. reformulation of industrial foods). Nutritional education programs are urgently needed to prevent CRC risk in LMICs.
Data sharing and data accessibility
Under the ethical committee policy of the University of Fez, data involving participants or patients cannot be publicly shared. Individual requests for further information on the study can be sent to the corresponding author.
Abbreviations
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CIQUAL:
-
French Food Composition Table
- CRC:
-
Colorectal cancer
- FCT:
-
Food composition table
- FFQ:
-
Food frequency questionnaire
- IARC:
-
International Agency for Research on Cancer
- IGFs:
-
Insulin-like growth factors
- LMIC:
-
Low- and middle-income countries
- NCDs:
-
Non-communicable diseases
- SD:
-
Standard deviation
- SSB:
-
Sugar-sweetened beverages
- UPF:
-
Ultra-processed foods
- USDA:
-
United States Department of Agriculture Nutrient Database
References
Bray F, Ferlay J, Soerjomataram I et al (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424. https://doi.org/10.3322/caac.21492
The Global Cancer Observatory Colorectal Cancer. Globocan 2018
Gunter MJ, Alhomoud S, Arnold M et al (2019) Meeting Report from the joint IARC-NCI international cancer seminar series: a focus on colorectal cancer. Ann Oncol. https://doi.org/10.1093/annonc/mdz044
World Cancer Research Fund International, American Institute for Cancer Research (2018) Diet, nutrition, physical activity and colorectal cancer-revised
Golzarand M, Mirmiran P, Jessri M et al (2012) Dietary trends in the Middle East and North Africa: an ecological study (1961 to 2007). Public Health Nutr 15:1835–1844. https://doi.org/10.1017/S1368980011003673
Belahsen R (2014) Nutrition transition and food sustainability. Proc Nutr Soc 73:385–388. https://doi.org/10.1017/S0029665114000135
World Health Organization (2018) Noncommunicable diseases (NCD) country profiles
El Rhazi K, Nejjari C, Romaguera D et al (2012) Adherence to a Mediterranean diet in Morocco and its correlates: cross-sectional analysis of a sample of the adult Moroccan population. BMC Public Health 12:345. https://doi.org/10.1186/1471-2458-12-345
Fondation Lalla Salma Prévention et Traitement des Cancers (2016) Registre des Cancers de la Région du Grand Casablanca 2008–2012. Edition 2016. [Internet]. Available from https://www.contrelecancer.ma/site_media/uploaded_files/RCRGC.pdf
Chadli S, Taqarort N, El Houate B, Oulkheir S (2018) Epidemiological transition in Morocco (1960–2015). Med Sante Trop 28:201–205. https://doi.org/10.1684/mst.2018.0800
Monteiro CA, Cannon G, Levy R et al (2016) NOVA. The star shines bright [Food classification Public health]. World Nutr 7:28–38
Monteiro CA, Moubarac J-C, Cannon G et al (2013) Ultra-processed products are becoming dominant in the global food system. Obes Rev 14(Suppl 2):21–28. https://doi.org/10.1111/obr.12107
Juul F, Martinez-Steele E, Parekh N et al (2018) Ultra-processed food consumption and excess weight among US adults. Br J Nutr 120:90–100. https://doi.org/10.1017/S0007114518001046
Rauber F, Chang K, Vamos EP et al (2021) Ultra-processed food consumption and risk of obesity: a prospective cohort study of UK Biobank. Eur J Nutr 60:2169–2180. https://doi.org/10.1007/s00394-020-02367-1
de Mendonça RD, Pimenta AM, Gea A et al (2016) Ultraprocessed food consumption and risk of overweight and obesity: the University of Navarra Follow-Up (SUN) cohort study. Am J Clin Nutr 104:1433–1440. https://doi.org/10.3945/ajcn.116.135004
Canhada SL, Luft VC, Giatti L et al (2020) Ultra-processed foods, incident overweight and obesity, and longitudinal changes in weight and waist circumference: the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Public Health Nutr 23:1076–1086. https://doi.org/10.1017/S1368980019002854
Beslay M, Srour B, Méjean C et al (2020) Ultra-processed food intake in association with BMI change and risk of overweight and obesity: a prospective analysis of the French NutriNet-Santé cohort. PLoS Med 17:e1003256. https://doi.org/10.1371/journal.pmed.1003256
Srour B, Fezeu LK, Kesse-Guyot E et al (2019) Ultra-processed food intake and risk of cardiovascular disease: prospective cohort study (NutriNet-Santé). BMJ 365:l1451. https://doi.org/10.1136/bmj.l1451
de Mendonça RD, Lopes ACS, Pimenta AM et al (2017) Ultra-processed food consumption and the incidence of hypertension in a mediterranean cohort: the Seguimiento Universidad de Navarra Project. Am J Hypertens 30:358–366. https://doi.org/10.1093/ajh/hpw137
Livingston AS, Cudhea F, Wang L et al (2021) Effect of reducing ultraprocessed food consumption on obesity among US children and adolescents aged 7–18 years: evidence from a simulation model. BMJ Nutr Prev Health. https://doi.org/10.1136/bmjnph-2021-000303
Machado PP, Steele EM, Levy RB et al (2020) Ultra-processed food consumption and obesity in the Australian adult population. Nutr Diabetes 10:1–11. https://doi.org/10.1038/s41387-020-00141-0
Cordova R, Kliemann N, Huybrechts I et al (2021) Consumption of ultra-processed foods associated with weight gain and obesity in adults: a multi-national cohort study. Clin Nutr 40:5079–5088. https://doi.org/10.1016/j.clnu.2021.08.009
Ma Y, Yang Y, Wang F et al (2013) Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS ONE 8:e53916. https://doi.org/10.1371/journal.pone.0053916
Gallagher EJ, LeRoith D (2020) Hyperinsulinaemia in cancer. Nat Rev Cancer 20:629–644. https://doi.org/10.1038/s41568-020-0295-5
Ottaiano A, De Divitiis C, Capozzi M et al (2018) Obesity and cancer: biological links and treatment implications. Curr Cancer Drug Targets 18:231–238. https://doi.org/10.2174/1568009617666170330125619
Deoula SM, El Kinany K, Huybrechts I et al (2019) Consumption of meat, traditional and modern processed meat and colorectal cancer risk among the Moroccan population: a large-scale case-control study. Int J Cancer 146:1333–1345. https://doi.org/10.1002/ijc.32689
Nicoli MC, Anese M, Parpinel M (1999) Influence of processing on the antioxidant properties of fruit and vegetables. Trends Food Sci Technol 10:94–100. https://doi.org/10.1016/S0924-2244(99)00023-0
Fiolet T, Srour B, Sellem L et al (2018) Consumption of ultra-processed foods and cancer risk: results from NutriNet-Santé prospective cohort. BMJ. https://doi.org/10.1136/bmj.k322
Sidi Deoula M, Huybrechts I, El Kinany K et al (2020) Behavioral, nutritional, and genetic risk factors of colorectal cancers in Morocco: protocol for a multicenter case-control study. JMIR Res Prot 9:e13998
El Kinany K, Garcia-Larsen V, Khalis M et al (2018) Adaptation and validation of a food frequency questionnaire (FFQ) to assess dietary intake in Moroccan adults. Nutr J 17:61. https://doi.org/10.1186/s12937-018-0368-4
Khalis M, Garcia-Larsen V, Charaka H et al (2020) Update of the Moroccan food composition tables: towards a more reliable tool for nutrition research. J Food Compos Anal 87:103397. https://doi.org/10.1016/j.jfca.2019.103397
Luiten CM, Steenhuis IH, Eyles H et al (2016) Ultra-processed foods have the worst nutrient profile, yet they are the most available packaged products in a sample of New Zealand supermarkets. Public Health Nutr 19:530–538. https://doi.org/10.1017/S1368980015002177
da Louzada MLC, Baraldi LG, Steele EM et al (2015) Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Prev Med 81:9–15. https://doi.org/10.1016/j.ypmed.2015.07.018
Cediel G, Reyes M, da Costa Louzada ML et al (2018) Ultra-processed foods and added sugars in the Chilean diet (2010). Public Health Nutr 21:125–133. https://doi.org/10.1017/S1368980017001161
Suez J, Korem T, Zeevi D et al (2014) Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 514:181–186. https://doi.org/10.1038/nature13793
Martínez Steele E, Baraldi LG, da Louzada MLC et al (2016) Ultra-processed foods and added sugars in the US diet: evidence from a nationally representative cross-sectional study. BMJ Open 6:e009892. https://doi.org/10.1136/bmjopen-2015-009892
Flemer B, Lynch DB, Brown JMR et al (2017) Tumour-associated and non-tumour-associated microbiota in colorectal cancer. Gut 66:633–643. https://doi.org/10.1136/gutjnl-2015-309595
Keku TO, Dulal S, Deveaux A et al (2015) The gastrointestinal microbiota and colorectal cancer. Am J Physiol Gastrointest Liver Physiol 308:G351-363. https://doi.org/10.1152/ajpgi.00360.2012
Sansonetti PJ, Medzhitov R (2009) Learning tolerance while fighting ignorance. Cell 138:416–420. https://doi.org/10.1016/j.cell.2009.07.024
Chang X, Zhang Y, Tang M, Wang B (2013) Health effects of exposure to nano-TiO2: a meta-analysis of experimental studies. Nanoscale Res Lett 8:51. https://doi.org/10.1186/1556-276X-8-51
IARC (413AD) Carbon black, titanium dioxide, and talc
Partridge D, Lloyd KA, Rhodes JM et al (2019) Food additives: assessing the impact of exposure to permitted emulsifiers on bowel and metabolic health—introducing the FADiets study. Nutr Bull 44:329–349. https://doi.org/10.1111/nbu.12408
Naimi S, Viennois E, Gewirtz AT, Chassaing B (2021) Direct impact of commonly used dietary emulsifiers on human gut microbiota. Microbiome 9:66. https://doi.org/10.1186/s40168-020-00996-6
Mehta BM (2015) Nutritional and toxicological aspects of the chemical changes of food components and nutrients during heating and cooking. In: Cheung PCK, Mehta BM (eds) Handbook of food chemistry. Springer, Berlin, Heidelberg, pp 897–936
Alonso-Pedrero L, Ojeda-Rodríguez A, Martínez-González MA et al (2020) Ultra-processed food consumption and the risk of short telomeres in an elderly population of the Seguimiento Universidad de Navarra (SUN) Project. Am J Clin Nutr 111:1259–1266. https://doi.org/10.1093/ajcn/nqaa075
Edalati S, Bagherzadeh F, AsghariJafarabadi M, Ebrahimi-Mamaghani M (2021) Higher ultra-processed food intake is associated with higher DNA damage in healthy adolescents. Br J Nutr 125:568–576. https://doi.org/10.1017/S0007114520001981
Liu P-H, Wu K, Ng K et al (2019) Association of obesity with risk of early-onset colorectal cancer among women. JAMA Oncol 5:37–44. https://doi.org/10.1001/jamaoncol.2018.4280
Garcia H, Song M (2019) Early-life obesity and adulthood colorectal cancer risk: a meta-analysis. Rev Panam Salud Publ 43:e3. https://doi.org/10.26633/rpsp.2019.3
Eaton J (2020) Country level sales of ultra-processed foods and sugar-sweetened beverages predict higher BMI and increased prevalence of overweight in adult and youth populations. Curr Dev Nutr 4:825. https://doi.org/10.1093/cdn/nzaa053_030
Pietrzyk Ł (2017) Food properties and dietary habits in colorectal cancer prevention and development. Int J Food Prop 20:2323–2343. https://doi.org/10.1080/10942912.2016.1236813
Kunzmann AT, Coleman HG, Huang W-Y et al (2015) Dietary fiber intake and risk of colorectal cancer and incident and recurrent adenoma in the prostate, lung, colorectal, and ovarian cancer screening trial12. Am J Clin Nutr 102:881–890. https://doi.org/10.3945/ajcn.115.113282
Song M, Chan AT, Sun J (2019) Influence of the gut microbiome, diet, and environment on risk of colorectal cancer. Gastroenterology 158:322–340. https://doi.org/10.1053/j.gastro.2019.06.048
Sozańska B (2019) Raw cow’s milk and its protective effect on allergies and asthma. Nutrients 11:469. https://doi.org/10.3390/nu11020469
Puddu P, Valenti P, Gessani S (2009) Immunomodulatory effects of lactoferrin on antigen presenting cells. Biochimie 91:11–18. https://doi.org/10.1016/j.biochi.2008.05.005
Fernández J, Ledesma E, Monte J et al (2019) Traditional processed meat products re-designed towards inulin-rich functional foods reduce polyps in two colorectal cancer animal models. Sci Rep 9:1–17. https://doi.org/10.1038/s41598-019-51437-w
Acknowledgements
Many thanks to Lalla Salma Foundation, Prevention and Treatment of Cancers (FLSC) and Moroccan Society of Diseases of the Digestive System (SMMAD) for the financing of this study. Many thanks also to all contributors to this work in the Five University Hospitals centers; the directors of UHCs: Fez (Pr. Ait Taleb K), Casablanca (Pr. Afif My H); Rabat (Pr. Chefchaouni Al Mountacer C); Oujda (Pr. Daoudi A); and Marrakech (Pr. Nejmi H). The heads of medical services and their teams: Casablanca (Pr. Benider A; Pr Alaoui R; Pr. Hliwa W; Pr. Badre W, Pr. Bendahou K, Pr. Karkouri M.), Rabat (Pr. Ahallat M; Pr. Errabih I; Pr. El Feydi AE; Pr. Chad B; Pr. Belkouchi A; Pr. Errihani H; Pr. Mrabti H; Pr. Znati K), Fez (Pr. Nejjari C; Pr Ibrahimi SA; Pr. El Abkari M; Pr. Mellas N; Pr. Chbani L; Pr. Benjelloun MC), Oujda (Pr. IsmailiZ; Pr. Chraïbi M; Pr. Abda N, Pr. Abbaoui S) and Marrakech (Pr. Khouchani M; Pr. Samlani Z; Pr. Belbaraka R; Pr. Amine M).
Funding
Not applicable. All participants voluntarily agreed to take part.
Author information
Authors and Affiliations
Contributions
KE and IH conceived the study idea, its design, and led the analyses and interpretation of the data, the writing of the original draft. KR conceived the study idea, its design, and led the analyses and interpretation of the data and supervised the drafting. EK contributed to the conception and the design of the study and to the review and the editing. HAB, MD, ZH, AE contributed to the conception, the design of the study and the data acquisition.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval and consent to participate
Ethical approval was obtained from the ethical committee of University Hospital Center of Fez.
Consent for publication
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
El Kinany, K., Huybrechts, I., Hatime, Z. et al. Food processing groups and colorectal cancer risk in Morocco: evidence from a nationally representative case–control study. Eur J Nutr 61, 2507–2515 (2022). https://doi.org/10.1007/s00394-022-02820-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-022-02820-3