
Abstract
Objective
To report dietary sugars consumption and their different types and food sources, in European adolescents.
Methods
Food consumption data of selected groups were obtained from 1630 adolescents (45.6% males, 12.5–17.5 years) from the HELENA study using two nonconsecutive 24-h recalls. Energy intake, total sugars and free sugars were assessed using the HELENA-DIAT software. Multiple regression analyses were performed adjusting for relevant confounders.
Results
Total sugars intake (137.5 g/day) represented 23.6% and free sugars (110.1 g/day), 19% of energy intake. Girls had significantly lower intakes of energy, carbohydrates, total sugars and free sugars. 94% of adolescents had a consumption of free sugars above 10% of total energy intake. The main food contributor to free sugars was ‘carbonated, soft and isotonic drinks,’ followed by ‘non-chocolate confectionary’ and ‘sugar, honey, jam and syrup.’ Older boys and girls had significantly higher intakes of free sugars from ‘cakes, pies and biscuits.’ Free sugars intake was negatively associated with low socioeconomic status for ‘non-chocolate confectionary’ and ‘sugar, honey and jam’ groups; with low maternal educational level for carbonated and ‘soft drinks,’ ‘sugar, honey and jam,’ ‘cakes and pies’ and ‘breakfast cereals’ groups; and with high paternal educational level for ‘carbonated and soft drinks’ and ‘chocolates’ group.
Conclusions
The majority (94%) of studied adolescents consumed free sugars above 10% of daily energy intake. Our data indicate a broad variety in foods providing free sugars. Continued efforts are required at different levels to reduce the intake of free sugars, especially in families with a low educational level.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The effects on health of free sugars or non-milk extrinsic sugars (NMES) (caloric sweeteners added in the processing or preparation of food and beverages) have been highlighted in the recent years [1]. In 1989, the Committee on Medical Aspects of Food Policy (COMA) classified sugars, mainly for health educational purposes, into intrinsic and extrinsic sugars [2]. Extrinsic sugars were classified as those sugars which were not located within the cellular structure of food and were further divided into milk sugars and NMES. The term NMES was mainly adopted by the UK, although ‘free sugars’ were accepted by the World Health Organization (WHO), and defined as all mono- and disaccharides added to foods by the manufacturer, cook and consumer, plus sugars naturally present in honey, syrup and unsweetened fruit juice. Under this definition, lactose when naturally present in milk and milk products is excluded [3, 4]. There is currently no common European recommendation for sugar intake. However, reducing the amount of sugar consumed is one of the most important dietary interventions to improve nutrition in children and adolescents; for instance, WHO [5–7] recommends that the consumption of free sugars should not exceed 10% of total daily energy intake.
The term ‘free sugars’ is, however, synonymous with the term NMES, and these terms are adopted in research worldwide [8]. In fact, old reports of the COMA (1989, 1991) and more recent studies [9] recommended that NMES consumption should be reduced and contribute no more than 10% or 60 g/day, to energy intake, as recommendations for free sugars [8]. Moreover, studies investigating total and different types of sugars used different terms to describe their intake, depending on the country in which the studies were done. But recent publications declare that it is recommended that the definition for ‘free sugars’ should be adopted in the UK too, instead NMES [10].
The increased consumption of free sugars has been linked to a low overall diet quality, as food rich in free sugars used to provide little nutrition value apart from supplying energy [11, 12]. The consumption of free sugars has been associated with cardiovascular diseases [13] and increased risk of type 2 diabetes [14] in adults. In children and adolescents, free sugars intake was also associated with the development of excess body weight and obesity [15–17], with high levels of low-density lipoproteins and triglycerides [18] and increased homeostasis model assessment-insulin resistance index (HOMA-IR) [19]. In addition, free sugars are the most important dietary cause of caries in children, adolescents and adults [20].
Previous national and local studies investigating adolescents’ diet already revealed that the percentage of total daily energy intake coming from free sugars ranged between 14 [21, 22] and 21% [23, 24] in Europe. Studies outside Europe showed higher values: 16–26% [25–29]. Concerning consumption trends, in the USA an increased consumption of caloric sweeteners was found, between 1962 and 2000 (from 74- to 83-kcal/day of caloric sweeteners). Of this increase, 80% comes from sugar-sweetened beverages [30]. However, recent studies in the USA [31] showed that between 1999–2000 and 2007–2008, the absolute intake of added sugars decreased from 100.1 to 76.7 g/day and the percentage of total energy from added sugars also decreased from 18.1 to 14.6%, because of a reduction in soda consumption.
Recent national and local studies showed that ‘soft drinks,’ ‘confectionary’ and ‘biscuits and cakes’ are the main sources of free sugars in Europe [23]. Several studies in US adolescents showed that ‘soft drinks’ were the largest source of added sugars, followed by ‘confectionary,’ ‘sugar,’ ‘cakes and biscuits’ and ‘dairy desserts’ [28, 31]. Studies in Australia reported that ‘sugar-sweetened beverages,’ ‘cakes, biscuits, pastries and batter-based products,’ and ‘sugar and sweet spreads’ were the top three contributors of added and free sugars [4, 32].
However, little is known about actual consumption of free sugars and their main food sources in European adolescents. The purpose of this study was to provide estimates of free sugars consumption among European adolescents and to analyze the main sources of these.
Methods
Study design
The Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) cross-sectional study (HELENA-CSS) is an European Union—funded project on lifestyle and nutrition among adolescents from ten European cities [Athens, Heraklion (Greece), Dortmund (Germany), Ghent (Belgium), Lille (France), Pécs (Hungary), Rome (Italy), Stockholm (Sweden), Vienna (Austria), and Zaragoza (Spain)] [33]. The underlying aim of HELENA-CSS was to obtain standardized, harmonized, and reliable data from a sample of adolescents on a range of nutrition and health-related parameters [34], such as dietary intake, anthropometry, physical activity, physical fitness, hematological and biochemical indices [33].
The HELENA-CSS inclusion criteria were age from 12.5 to 17.5 years, not participating simultaneously in another clinical trial, and free of any acute infection during the week before inclusion [35]. The sample size was estimated according to the mean BMI (nutritional status index showing the largest variability) and variance values, for each sex and age stratum. This procedure enabled us to adequately describe all the variables included in the study. For the sample size calculation, a confidence level of 95% and an error of ±0.3 were assumed [36]. The final sample was estimated to be 3500 adolescents. From October 1, 2006, through December 31, 2007, a total of 3528 adolescents (46.9% boys) were recruited [37]. Study recruitment was conducted at schools. To guarantee that the heterogeneity of social background of the population would be represented, schools were randomly selected after stratification on school zone or district. Up to three classes from two grades were selected per school. All the adolescents within selected classrooms were invited to participate. Only adolescents from classrooms where more than 70% of the individuals consented to participate were included. If participation rates fell below 70%, the class was excluded and another class (in the same age group) was invited from the same school. The response rate for the schools and classes differed importantly between countries [with Austria having the lowest participation rate (57% of schools) and France the highest (92% of schools)]. The global participation rate for pupils within the participating classes also differed importantly between countries (ranging from 61% for France to 85% for Germany). Within the participating classes, participation rates (by definition ≥70%) ranged from 79.2% in France to 98.1% in Hungary [35]. Sampling and recruitment procedures are described in detail elsewhere [35].
The study was approved by Research Ethics Committees in each involved city, and written informed consent was obtained from participating adolescents and their parents [38].
Data collection
Dietary assessment
Dietary consumption was assessed using the self-administered, computerized 24-h recall, named HELENA Dietary Assessment Tool (HELENA-DIAT), based on the Young Adolescents’ Nutrition Assessment software, developed and validated in Flemish adolescents. To assess the relative validity and acceptability of the computerized 24-h recall, food and nutrient intakes assessed with the 24-h recall were compared with food records (study 1) and 24-h dietary recall interviews (study 2). HELENA-DIAT proved to agree well with both standard methods in categorizing subjects in consumers and no consumers [κ (study 1) = 0.48–0.92; κ (study 2) = 0.38–0.90]. Spearman’s correlations for energy and nutrient intakes ranged between 0.44 and 0.79 for study 1 and between 0.44 and 0.86 for study 2. In the tests to investigate whether HELENA-DIAT agreed with the other methods in ranking portions/amounts in consumers, results only were fair to moderate for most of the food groups (weighted κ study 1 = 0.11–0.55; study 2 = 0.04–0.73) [39]; this tool was improved and culturally adapted to the nine participating European countries. The HELENA-DIAT tool has been evaluated and shown to be a good method to collect detailed dietary information from adolescents, and it was well received by the study participants [40].
The European Food Consumption Survey Method (EFCOSUM) project found the repeated 24HR to be a suitable method to obtain population means and distributions [41]. The adolescents completed the 24HR twice (within 2 weeks) during school time, after a short introduction by researchers; both times, trained field workers, including a dietitian, were present in the classroom to help the adolescent if necessary. HELENA-DIAT used special techniques to support and enhance respondents’ memory and used series of portion size photos of standard dishes/foods, which allowed detailed description and quantification of the foods and recipes consumed [42]. The participant could select from about 400 predefined food items and was free to add non-listed foods and eaten amounts could be reported in grams or household measures [43]. This tool is based on six meal occasions referring to the day before the interview and organized as breakfast, morning snack, lunch, afternoon snack, evening meal and evening snack [43]. Every participant was asked to fill in the HELENA-DIAT on arbitrary non-consecutive days, twice in a time span of 2 weeks, to achieve information closer to the habitual intake. The recalls thus comprised dietary intake information about weekdays and weekend days [43].
To avoid difficulties in obtaining comparable measures across countries using different country-specific food composition tables, data of the HELENA-DIAT were linked to the German Food Code and Nutrient Data Base [BLS (Bundeslebensmittelschlüssel), version II.3.1, 2005] to calculate energy and nutrient intake [44]. This food composition database contained the largest number of nutrients and food items, approximately 12,000 coded foods, menus and menu components with up to 158 nutrients available for each product.
The usual dietary intake of nutrients and foods, also including occasionally consumed foods, was estimated by the multiple source method (MSM) [45]. The MSM calculates dietary intake for individuals first and then constructs the population distribution based on the individual data. With this method intake, data were adjusted taking into account both between and within individual variability of the dietary intake [46]. After applying the MSM method, dietary data were analyzed for average energy intake in kilocalories (kcal) and kilojoules (kJ), carbohydrates, saccharides (monosaccharides and disaccharides), total sugars, free sugars in grams (g), and percentages of energy from carbohydrates, total sugars and free sugars. As analytical data for lactose were available, free sugars content was calculated by subtracting the lactose of the total sugars, based on the methodology by steps for estimating added sugar content of foods of Louie et al. [47].
Foods were grouped in order to determine the relative importance of dietary sources of total sugars and free sugars. Of the total food groups, nine were selected, as they contained free sugars: (1) carbonated, soft, isotonic drinks including non-alcoholic wine, non-alcoholic beer; (2) fruit and vegetable juices; (3) non-chocolate confectionary; (4) sugar, honey, jam and syrup; (5) chocolate; (6) desserts and puddings milk based (including ice cream); (7) cakes, pies, biscuits; (8) breakfast cereals; and (9) other sources (all other food groups).
Whereas sugars in unsweetened fruit juices were classified as natural sugars in 1980, they are, by definition, free sugars. Our results are also including free sugars added to fruit juices [23, 48].
Total daily energy intake was used to exclude potentially implausible recalls [49] by comparing it with basal metabolic rate (BMR) estimated using the equations of Schofield [50]. Using the approach of Goldberg et al. [51], and assuming a standard physical activity level (PAL) of 1.55 and considering two independent recall days, adolescents were classified as under-reporters (ratio of energy intake to BMR <0.99) and over-reporters (ratio of energy intake to BMR >2.40).
Socioeconomic status
Family Affluence Scale (FAS) Information on family socioeconomic status (SES) can be difficult to collect from young people because they do not know or are not willing to reveal such information. The FAS was originally designed to be a supplementary measure to the traditional socioeconomic indicators of parental occupation [51]. The FAS data were collected by means of a self-reported questionnaire [52]. This scale was used in the present study as an index of family well-being, and it is based on the concept of material conditions of the family. Adolescents selected a set of items which reflected family expenditure and consumption [53]. This scale includes four questions answered by the adolescent in a questionnaire: (1) Do you have your own bedroom? (2) How many cars are there in your family? (3) How many PCs are there in your home? (4) Do you have internet access at home?
In this study, low, medium and high FAS status were defined based on the final score obtained from the four questions, after giving a numerical value to each possible answer in the four questions: low (from 0 to 2), medium (from 3 to 5) and high (from 6 to 8) [54].
Parental educational level
Parental educational level (maternal and paternal educational level) data were collected using the SES self-questionnaire and adapted in each country from the International Standard Classification of Education (ISCED) in primary education (ISCED level 0 or 1; score = 1); lower secondary education (ISCED level 2; score = 2); higher secondary education (ISCED level 3 or 4; score = 3); tertiary education (ISCED level 5 or 6; score = 4). For the purposes of the present study, we merged the two lower levels into one group (i.e., ‘primary education and lower secondary education’) and obtained three groups: low (the lowest parental educational level), medium and high (the highest) [55].
Participants
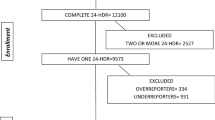
Of the 3528 recruited adolescents, 1188 (33.7%) adolescents were excluded from the analysis based on incomplete or implausible intake in the 24HRs (Fig. 1). For the present analysis, data on nutritional intake from Heraklion (Greece) and Pecs (Hungary) could not be included because of incomplete data.

Flowchart of the participants included in the analysis
Using the approach of Goldberg et al. [51], 527 (22.5%) adolescents were considered as under-reporters and 183 (7.8%) adolescents were considered as over-reporters and were excluded. The final sample with sufficient and plausible dietary data on energy and nutrient intakes was 1630 adolescents (45.6% males and 54.4% females).
Sensitivity analyses were conducted (testing different possibilities: including/excluding children with one or two repeated 24-HDR, including/excluding over-reporters, under-reporters). When including only children with one repeated 24 dietary recall, estimates became unstable due to the sample size. In the other cases, results remained nearly unchanged compared with the results given in this study.
Statistical methods
For the descriptive analyses, mean intakes and standard deviation (SD) for continuous data are presented. Tests for normality were performed, using a Kolmogorov–Smirnov test. Mean daily intake (g) of free sugars and total sugars (g) from various dietary sources consumed by boys and girls were tested and Student’s t tests were used to compare means by sex. Mean daily intake (g) of free sugars from various dietary sources consumed by boys and girls, stratified by age groups (<15 and ≥15 years), was studied [36], and Student’s t tests were used to compare means of free sugars intake by age groups.
Multiple linear regression analysis was conducted in order to determine the association of free sugars intake from selected food groups with FAS and parental educational level after adjusting for sex, age and total energy intake. Food groups entered in the model were those found to be significantly associated with FAS and parental educational level in the univariate analysis (FAS and parental educational level were entered as dummy variables, and medium level of both variables was taken as the reference level). The results are presented as β coefficients and 95% confidence intervals. For the food sources analyses, per capita and per consumer analysis were done. Per capita analysis included all subjects with plausible data from 24-h recalls, and it represents the mean intake of the population. Per consumer analysis included only subjects who reported the consumption of a certain food item in the food groups tested. p values <0.05 from two-sided hypotheses are considered as statistically significant. The SPSS statistical software package version 18.0 (SPSS Inc., Chicago, IL, USA) was used to conduct all statistical analyses.
Results
The sample characteristics and mean daily intake of energy, carbohydrates and sugars for boys, girls and all subjects in the eight survey centers in Europe participating in HELENA study are presented in Table 1. Mean total energy intake was 8675 (SD 1387) kJ/day for girls and 10,968 (SD 1929) kJ/day for boys. Total sugars intake [137.5 (SD 49.7) g/day] represented 23.6 (SD 6.8)% of energy intake. Free sugars [110.1 (SD 48.8) g/day] represented 19 (SD 6.5)% of energy intake. Girls had significantly (p < 0.001) lower intakes of energy, carbohydrates, total sugars, free sugars and significantly lower percentage of energy from carbohydrates, compared with boys. The percentage of adolescents having free sugars consumption above 10% of total energy intake was 94%.
Figure 2a, b shows the mean daily intake of total sugars and free sugars from the selected food groups (as percentage of sugars intake) for boys and girls. The main contributor to free sugars was ‘sweetened beverages’: ‘carbonated/soft drinks’ + ‘fruit and vegetables juices’ (26%); the contribution of ‘carbonated, soft, isotonic drinks’ was 14.4%, followed by ‘confectionary non-chocolate’ (13.5%) and ‘sugar, honey, jam and syrup’ (13.3%). Mean intake of free sugars per capita and per consumer of all studied food groups was significantly lower in girls, compared with boys (Table 2).

a Mean and standard deviation, daily intake of total sugars from the selected food groups (percentage contribution to total sugars intake and SD in brackets) for boys and girls. b Mean and standard deviation, daily intake of free sugars from the selected food groups (percentage contribution to total sugars intake and SD in brackets) for boys and girls. Asterisk sweetened beverages: carbonated/soft drinks + fruit and vegetable juices
When examining by age groups, intakes of free sugars of all studied food groups were significantly higher in older boys and girls than in younger ones in per consumer analysis, but results were only significant in the case of ‘cakes, pies and biscuits’ group in per capita analysis (Table 3).
Table 4 illustrates the results of the multiple linear regression model using the free sugars intake from ‘carbonated and soft drinks,’ ‘confectionary non-chocolate’ group and ‘sugar, honey and jam,’ ‘chocolate,’ ‘cakes and pies’ and ‘breakfast cereals’ groups as dependent variable and the levels of FAS and parental education (from mother and father) as independent variable, after adjusting for sex, age and total energy intake.
The results of this analysis indicate that adolescents with a low FAS had a less intake of free sugars from ‘confectionary non-chocolate’ and ‘sugar, honey and jam’ groups, than those with a medium FAS. Adolescents with a low maternal educational level had a higher intake of free sugars from ‘carbonated and soft drinks,’ ‘sugar, honey and jam,’ ‘cakes and pies and breakfast cereals’ groups, than those with a medium maternal educational level. And adolescents with a high paternal educational level had less intake of free sugars from ‘carbonated and soft drinks’ and the ‘chocolates’ groups, than those with a medium paternal educational level.
Discussion
First of all, we found in the literature that studies investigating total and types of sugars used different indicators to describe their intake, depending on the organization or the country in which the studies were done. The main indicators used were: total daily sugar intake (g), total daily sugar intake as % of energy [23–25], NMES [23], added sugars [21, 22, 25, 26, 31], added sweeteners [28], simple sugars [29], caloric sweeteners [30], free sugars daily intake (g) and free sugars intake as % of energy [17]. For the last indicators, the proportion of the population, but not the mean intake, was described. This variability in terminology across countries meant that comparisons were limited to within countries [56].
Our findings provide an overview of the intakes and food sources of sugars in general, and free sugars in particular, of a large sample of urban European adolescents. In our study, free sugars accounted for 19 (6.5)% of energy intake, higher than the recommended 10% of energy [5–7], but within the observed range in other studies mentioned in the introduction section.
The proportion of adolescents consuming more than 10% of energy from free sugars was 94%. The consumption of free sugars is higher in boys than in girls. Free sugars were provided in similar proportions by the different food groups. Both, ‘carbonated, soft and isotonic drinks’ and ‘fruit juices’ are providing 26.7% of the total free sugars consumption. Similar food contributors to free sugars intake were observed in other studies [4, 23, 28, 31, 32].
It was also observed that the contribution of the various sources of sugars did not change through the years: several studies demonstrated, like ours, that soft drinks were the largest source of free sugars. Cavadini et al. [57] also reported that soft drinks consumption nearly tripled in boys and more than doubled in girls, from 1965 to 1996.
In addition, compared with research in the USA and elsewhere, the high levels of free sugars provided by sweetened milk beverages (including chocolate milk and flavored yogurt drinks all with added sugar) and fruit juice intake seem to be typical for European adolescents [58].
As in the HELENA adolescents, most studies involving boys and girls showed higher intakes of total sugars and added sugars or free sugars in boys than in girls [4, 23, 24, 28]; also, it can be observed in the different studies that older children and adolescents have the highest amount of total and free sugars intake, both in grams as in percentage of total energy intake [23, 24, 28, 31].
However, not all studies showed differences of total and free sugars intake by social class [27], or only differences in girls [23]. In the present study, parental educational level (maternal and paternal) was chosen as a traditional socioeconomic indicator, and FAS was included as supplementary measure of SES to reflect family expenditure, consumption and changes in technological developments (personal computers) across countries. Car ownership, bedroom occupancy, computer ownership and use of internet are among the items currently used by a wide range of contemporary surveys [59]. Overall, adolescents with high FAS participating in this study showed higher consumption of free sugars from ‘non-chocolate confectionary’ and ‘sugar, honey and jam’ groups.
Only two studies were found reporting sugar intake and FAS. They were, however, old studies reporting dietary trends among schoolchildren during the 1990s. Children with lower FAS scores were found to consume more soft drinks and high-sugar foods compared with children with higher FAS score [60, 61].
A study in the Netherlands [62] showed that children of low and mid-low educated mothers were significantly more likely to consume excessive amounts of sugar-containing beverages compared with children of high-educated mothers. Parental feeding practices, parental consumption of sugar-containing beverages, and children’s television time partly explained these associations.
In a study with Norwegian adolescents [63, 64], differences in perceived availability of both sugar-sweetened beverages (SSB) and fruit and vegetables on the basis of parental education were found, whereas the differences in intake were significant only for SSB. In another study in Canada [65], students whose parents completed college or university were less likely to consume SSB daily.
As expected, in our study, low parental educational level was positively associated with high intakes of free sugars. However, we found high intake of free sugars in high FAS level adolescents. These results could be in part explained because parental education and FAS are different indicators of socioeconomic status. In fact, FAS include different dimensions, like the use of internet and the acquisition in the recent years of more luxury devices (like mobiles, computers, laptops.). It has been observed that low SES groups are using more the mobile phone, spending more money on applications and installing more applications overall [66, 67].
The described differences of sugars intake in the different countries and studies may be a result of a combination of factors. The observed differences could be a consequence of variations in data collection methods, food grouping, inclusion or not of misreporters, selection of food composition databases and local and national policies: in the different studies we examined, the data were collected using different methods [4, 22–29, 31]; only few studies provided a complete list of sources of total and free sugars [23, 28, 31], but they were using different food groups; the food composition and other databases used to analyze data were different too, or not revealed in the study [4, 24, 27, 28, 31]; in several countries there is a public health and food industry effort to advice people to reduce the consumption of sugars, whereas in other countries there is a need to improve this fact. For example, in the USA, the decrease in added sugars has been driven by a reduction in soda consumption (sweetened beverages). In 2001, US states started to adopt legislation regulating access to SSB in public schools, and as result, between 2004–2005 and 2009–2010, the number of beverage calories delivered to schools decreased by 88% [31].
This study has some limitations. Firstly, the HELENA-CSS study is not fully representative of the European population [36, 64], but providing information on urban adolescents living in selected cities. Food consumption data were acquired by self-reported questionnaires, and therefore a social bias must be considered. Nevertheless, our 24-h recall method has been tested and validated, indicating acceptable accuracy [40]. Another limitation is the fact that the 24-h recalls were all completed during school days (about the dietary intake of the previous day) and thus did not include information about the adolescents’ diet on Fridays and Saturdays or on holidays.
A particular strength of our study is the sample size, the geographical spread over eight European cities and the large and culturally diverse sample of the adolescents. The sample consists of adolescents assessed using highly standardized and validated procedures. Another strength is the use of the MSM taking into account both between- and within individual variability of the dietary intake data. The exclusion of misreporters identified using a published method [51], improved the quality of the data, although the exclusion can be a limitation and might have induced selection bias since the misreporters (especially overreporters) might have a special food choice or eating behavior.
Conclusions
This study provides important information about sugar intake patterns among European adolescents. The majority (94%) of European adolescents was found to consume high amounts of sugars (i.e., % of energy from free sugars above 10%). The main contributor to free sugars intake was ‘carbonated, soft, isotonic drinks’ (14.4%), followed by ‘non-chocolate confectionary’ (13.5%) and ‘sugar, honey, jam and syrup’ (13.3%). Our data indicate that adolescents consume free sugars via a broad variety of foods. Continued and coordinated efforts are required at a national, community and individual level to reduce the intake of free sugars.
References
Te Morenga L, Mallard S, Mann J (2012) Dietary sugars and body weight: systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 15(346):e7492. doi:10.1136/bmj.e7492
Department of Health (1991) Dietary reference values for food energy and nutrients in the United Kingdom. Report on health and social subjects, No. 41. HMSO, London
Farajian P, Risvas G, Panagiotakos DB, Zampelas A (2016) Food sources of free sugars in children’s diet and identification of lifestyle patterns associated with free sugars intake: the GRECO (Greek Childhood Obesity) study. Public Health Nutr 19(13):2326–2335
Louie JC, Moshtaghian H, Rangan AM, Flood VM, Gill TP (2015) Intake and sources of added sugars among Australian children and adolescents. Eur J Nutr. doi:10.1007/s00394-015-1041-8
World Health Organization (WHO) (1990) Diet, nutrition and the prevention of chronic diseases. Report of a WHO Study Group, WHO Technical Report Series No. 797. WHO, Geneva
World Health Organization/Food and Agricultural Organization (WHO/FAO) (2003) Diet in the prevention of chronic diseases, Technical Report Series No. 916. WHO/FAO, Geneva
World Health Organization (WHO) (2015) Guideline: sugars intake for adults and children. World Health Organization, Geneva
Kelly SA, Summerbell C, Rugg-Gunn AJ, Adamson A, Fletcher E, Moynihan PJ (2005) Comparison of methods to estimate non-milk extrinsic sugars and their application to sugars in the diet of young adolescents. Br J Nutr 94(1):114–124
Sheiham A (2001) Dietary effects on dental diseases. Public Health Nutr 4(2B):569–591
SACN Carbohydrates and Health Report (2015) Public health England. SACN: reports and position statements. ISBN: 9780117082847
Alexy U, Sichert-Hellert W, Kersting M (2003) Associations between intake of added sugars and intakes of nutrients and food groups in the diets of German children and adolescents. Br J Nutr 90:441–447
Marshall TA, Eichenberger Gilmore JM, Broffitt B, Stumbo PJ, Levy SM (2005) Diet quality in young children is influenced by beverage consumption. J Am Coll Nutr 24:65–75
Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB (2014) Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med 174(4):516–524. doi:10.1001/jamainternmed.2013.13563
Malik VS, Popkin BM, Bray GA, Després JP, Willett WC, Hu FB (2010) Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: a meta-analysis. Diabetes Care 33(11):2477–2483. doi:10.2337/dc10-1079
Libuda L, Kersting M (2009) Soft drinks and body weight development in childhood: is there a relationship? Curr Opin Clin Nutr Metab Care 12(6):596–600. doi:10.1097/MCO.0b013e32833189f6
Council on School Health; Committee on Nutrition (2015) Snacks, sweetened beverages, added sugars, and schools. Pediatrics 135(3):575–583. doi:10.1542/peds.2014-3902
Ambrosini GL, Johns DJ, Northstone K, Emmett PM, Jebb SA (2016) Free sugars and total fat are important characteristics of a dietary pattern associated with adiposity across childhood and adolescence. J Nutr 146:778–784
Welsh JA, Sharma A, Cunningham SA, Vos MB (2011) Consumption of added sugars and indicators of cardiovascular disease risk among US adolescents. Circulation 123:249–257. doi:10.1161/CIRCULATIONAHA.110.972166
Kondaki K, Grammatikaki E, Jiménez-Pavón D, De Henauw S, González-Gross M, Sjöstrom M, Gottrand F, Molnar D, Moreno LA, Kafatos A, Gilbert C, Kersting M, Manios Y (2013) Daily sugar-sweetened beverage consumption and insulin resistance in European adolescents: the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr 16(3):479–486. doi:10.1017/S1368980012002613
Sheiham A, James WP (2015) Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res 94(10):1341–1347. doi:10.1177/0022034515590377
Lyhne N, Ovesen L (1999) Added sugars and nutrient density in the diet of Danish children. Scand J Nutr 43:4–7
Kersting M, Sichert-Hellert W, Alexy U, Manz F, Schoch G (1998) Macronutrient intake of 1 to 18 year old German children and adolescents. Z Ernahrungswiss 37:252–259
Rugg-Gunn AJ, Fletcher ES, Matthews JN, Hackett AF, Moynihan PJ, Kelly S, Adams J, Mathers JC, Adamson A (2007) Changes in consumption of sugars by English adolescents over 20 years. Public Health Nutr 10(4):354–363
Strain JJ, Robson PJ, Livingstone MBE, Primrose ED, Savage JM, Cran GW, Boreham CA (1994) Estimates of food and micronutrient intake in a random sample of Northern Ireland adolescents. Br J Nutr 72:343–352
George JH, Brinstone SC, Paulin JM, Aitkin EG (1993) What do young adolescent New Zealanders eat? Nutrient intake of a nationwide sample of form 1 children. N Z Med J 106:47–51
Nicklas TA, Myers L, Beech B, Berenson GS (1999) Trends in dietary intake of sugars of 10-year-old children from 1973 to 1988: the Bogalusa heart study. Nutr Res 19:519–530
Muñoz KA, Krebs-Smith SM, Ballard-Barbish R, Cleveland LE (1997) Food intake of US children and adolescents compared with recommendations. Pediatrics 100:323–329
Guthrie JF, Morton JF (2000) Food sources of added sweeteners in the diets of Americans. J Am Diet Assoc 100:43–48
Shatenstein B, Ghadirian P (1996) Nutrient patterns and nutritional adequacy among French-Canadian children in Montreal. J Am Coll Nutr 15:264–272
Popkin BM, Nielsen SJ (2003) The sweetening of the world’s diet. Obes Res 11:1325–1332
Welsh JA, Sharma AJ, Grellinger L, Vos MB (2011) Consumption of added sugars is decreasing in the United States. Am J Clin Nutr 94(3):726–734. doi:10.3945/ajcn.111.018366
Lei L, Rangan AM, Flood VM, Louie JC (2016) Dietary intake and food sources of added sugar in the Australian population. Br J Nutr 115(5):868–877
Moreno LA, González-Gross M, Kersting M, Molnár D, de Henauw S, Beghin L, Sjöström M, Hagströmer M, Manios Y, Gilbert CC, Ortega FB, Dallongeville J, Arcella D, Wärnberg J, Hallberg M, Fredriksson H, Maes L, Widhalm K, Kafatos AG, Marcos A, HELENA Study Group (2008) Assessing, understanding and modifying nutritional status, eating habits and physical activity in European adolescents: the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr 11(3):288–299
De Henauw S, Gottrand F et al (2007) Nutritional status and lifestyles of adolescents from a public health perspective. The HELENA project—Healthy Lifestyle in Europe by Nutrition in Adolescence. J Public Health 15(3):187–197
Moreno LA, De Henauw S, González-Gross M, Kersting M, Molnár D, Gottrand F, Barrios L, Sjöström M, Manios Y, Gilbert CC, Leclercq C, Widhalm K, Kafatos A, Marcos A, HELENA Study Group (2008) Design and implementation of the Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-sectional study. Int J Obes (Lond) 32:S4–S11
Rey-López JP, Vicente-Rodriguez G, Ortega FB, Ruiz JR, Martinez-Gómez D, De Henauw S, Manios Y, Molnar D, Polito A, Verloigne M, Castillo MJ, Sjöström M, De Bourdeaudhuij I, Moreno LA, HELENA Study Group (2010) Sedentary patterns and media availability in European adolescents: the HELENA study. Prev Med 51(1):50–55. doi:10.1016/j.ypmed.2010.03.013
Béghin L, Huybrechts I, Vicente-Rodríguez G, De Henauw S, Gottrand F, Gonzales-Gross M, Dallongeville J, Sjöström M, Leclercq C, Dietrich S, Castillo M, Plada M, Molnar D, Kersting M, Gilbert CC, Moreno LA (2012) Main characteristics and participation rate of European adolescents included in the HELENA study. Arch Public Health 70(1):14. doi:10.1186/0778-7367-70-14
Béghin L, Castera M, Manios Y, Gilbert CC, Kersting M, De Henauw S, Kafatos A, Gottrand F, Molnar D, Sjostrom M, Leclercq C, Widhalm K, Mesana MI, Moreno LA, Libersa C (2008) Quality assurance of ethical issues and regulatory aspects relating to good clinical practices in the HELENA Cross-sectional study. Int J Obes 32:S12–S18. doi:10.1038/ijo.2008.179
Vereecken CA, Covents M, Matthys C, Maes L (2005) Young adolescents’ nutrition assessment on computer (YANA-C). Eur J Clin Nutr 59:658–667
Vereecken CA, Covents M, Sichert-Hellert W, Alvira JMF, Le Donne C, De Henauw S, De Vriendt T, Phillipp MK, Beghin L, Manios Y, Hallstrom L, Poortvliet E, Matthys C, Plada M, Nagy E, Moreno LA (2008) Development and evaluation of a self-administered computerized 24-h dietary recall method for adolescents in Europe. Int J Obes 32:S26–S34
Brussaard JH, Lowik MRH, Steingrimsdottir L, Moller A, Kearney J, De Henauw S, Becker W (2002) A European food consumption survey method conclusions and recommendations. Eur J Clin Nutr 56:S89–S94
Santaliestra-Pasías AM, Mouratidou T, Verbestel V, Huybrechts I, Gottrand F, Le Donne C, Cuenca-García M, Díaz LE, Kafatos A, Manios Y, Molnar D, Sjöström M, Widhalm K, De Bourdeaudhuij I, Moreno LA, Healthy Lifestyle in Europe by Nutrition in Adolescence Cross-sectional Study Group (2012) Food consumption and screen-based sedentary behaviors in European adolescents: the HELENA study. Arch Pediatr Adolesc Med 166(11):1010–1020. doi:10.1001/archpediatrics.2012.646
Diethelm K, Huybrechts I, Moreno L, De Henauw S, Manios Y, Beghin L, González-Gross M, Le Donne C, Cuenca-García M, Castillo MJ, Widhalm K, Patterson E, Kersting M (2014) Nutrient intake of European adolescents: results of the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) study. Public Health Nutr 17(3):486–497. doi:10.1017/S1368980013000463
Julián-Almárcegui C, Bel-Serrat S, Kersting M, Vicente-Rodriguez G, Nicolas G, Vyncke K, Vereecken C, De Keyzer W, Beghin L, Sette S, Halström L, Grammatikaki E, Gonzalez-Gross M, Crispim S, Slimani N, Moreno L, De Henauw S, Huybrechts I (2015) Comparison of different approaches to calculate nutrient intakes based upon 24-h recall data derived from a multicenter study in European adolescents. Eur J Nutr 55(2):537–545. doi:10.1007/s00394-015-0870-9
Haubrock J, Harttig U, Souverein O, Boeing H (2010) An improved statistical tool for estimating usual intake distributions: the multiple source method (MSM). Arch Public Health 68:14–15
Ottevaere C, Huybrechts I, Béghin L, Cuenca-Garcia M, De Bourdeaudhuij I, Gottrand F, Hagströmer M, Kafatos A, Le Donne C, Moreno LA, Sjöström M, Widhalm K, De Henauw S, HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study Group (2011) Relationship between self-reported dietary intake and physical activity levels among adolescents: the HELENA study. Int J Behav Nutr Phys Act 6(8):8. doi:10.1186/1479-5868-8-8
Louie JCY, Moshtaghian H, Boylan S, Flood VM, Rangan AM, Barclay AW, Brand-Miller JC, Gill TP (2015) A systematic methodology to estimate added sugar content of foods. Eur J Clin Nutr 69(2):154–161. doi:10.1038/ejcn.2014.256
Rugg-Gunn A, Adamson AJ, Appleton DR, Butler TJ, Hackett AF (2007) Sugars consumption by 379 11–12-year-old English children in 1990 compared with results in 1980. J Hum Nutr Diet 20(3):171–183
Bel-Serrat S, Julián-Almárcegui C, González-Gross M, Mouratidou T, Börnhorst C, Grammatikaki E, Kersting M, Cuenca-García M, Gottrand F, Molnár D, Hallström L, Dallongeville J, Plada M, Roccaldo R, Widhalm K, Moreno LA, Manios Y, De Henauw S, Leclercq C, Vandevijvere S, Lioret S, Gutin B, Huybrechts I (2016) Correlates of dietary energy misreporting among European adolescents: the Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA) study. Br J Nutr 115(8):1439–1452. doi:10.1017/S0007114516000283
Schofield WN (1985) Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 39(Suppl. 1):5–41
Goldberg GR, Black AE, Jebb SA, Cole TJ, Murgatroyd PR, Coward WA, Prentice AM (1991) Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur J Clin Nutr 45:569–581
Pigeyre M, Bokor S, Romon M, Gottrand F, Gilbert CC, Valtueña J, Gómez-Martínez S, Moreno LA, Amouyel P, Dallongeville J, Meirhaeghe A, HELENA Study Group (2010) Influence of maternal educational level on the association between the rs3809508 neuromedin B gene polymorphism and the risk of obesity in the HELENA study. Int J Obes (Lond) 34(3):478–486. doi:10.1038/ijo.2009.260
Currie CE, Elton RA, Todd J, Platt S (1997) Indicators of socioeconomic status for adolescents: the WHO Health Behaviour in School-aged Children Survey. Health Educ Res 12(3):385–397
Jiménez Pavón D, Ortega FP, Ruiz JR, España Romero V, García Artero E, Moliner Urdiales D, Gómez Martínez S, Vicente Rodríguez G, Manios Y, Béghin L, Répasy J, Sjöstrom M, Moreno LA, González Gross M, Castillo MJ, HELENA Study Group (2010) Socioeconomic status influences physical fitness in European adolescents independently of body fat and physical activity: the HELENA study. Nutr Hosp 25(2):311–316
Béghin L, Dauchet L, De Vriendt T, Cuenca-García M, Manios Y, Toti E, Plada M, Widhalm K, Repasy J, Huybrechts I, Kersting M, Moreno LA, Dallongeville J, HELENA Study Group (2014) Influence of parental socio-economic status on diet quality of European adolescents: results from the HELENA study. Br J Nutr 111(7):1303–1312. doi:10.1017/S0007114513003796
Wittekind A, Walton J (2014) Worldwide trends in dietary sugars intake. Nutr Res Rev 27(2):330–345. doi:10.1017/S0954422414000237
Cavadini C, Siega-Riz AM, Popkin BM (2000) US adolescent food intake trends from 1965 to 1996. Arch Dis Child 83:18–24
Duffey KJ, Huybrechts I, Mouratidou T, Libuda L, Kersting M, De Vriendt T, Gottrand F, Widhalm K, Dallongeville J, Hallström L, González-Gross M, De Henauw S, Moreno LA, Popkin BM, HELENA Study Group (2012) Beverage consumption among European adolescents in the HELENA study. Eur J Clin Nutr 66(2):244–252. doi:10.1038/ejcn.2011.166
Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M (2008) Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med 66(6):1429–1436. doi:10.1016/j.socscimed.2007.11.024
Inchley J, Todd J, Bryce C, Currie C (2001) Dietary trends among Scottish schoolchildren in the 1990s. J Nutr Diet 14(3):207–216
Mullan E, Currie C (2000) Socieconomic inequalities in adolescent health. In: Currie C, Hurrelmann K, Settertobulte W, Smith R, Todd J (eds) Health and health behaviour among young people. WHO policy series: health policy for children and adolescents issue 1, WHO regional office for Europe, Copenhagen, pp 65–72
Wijtzes AI, Jansen W, Jansen PW, Jaddoe VW, Hofman A, Raat H (2013) Maternal educational level and preschool children’s consumption of high-calorie snacks and sugar-containing beverages: mediation by the family food environment. Prev Med 57(5):607–612. doi:10.1016/j.ypmed.2013.08.014
Bjelland M, Lien N, Grydeland M, Bergh IH, Anderssen SA, Ommundsen Y et al (2011) Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (Health in Adolescents) study. Public Health Nutr 14:2156–2165. doi:10.1017/S1368980011000917
Bjelland M, Hausken SE, Bergh IH, Grydeland M, Klepp KI, Andersen LF, Totland TH, Lien N (2015) Changes in adolescents’ and parents’ intakes of sugar-sweetened beverages, fruit and vegetables after 20 months: results from the HEIA study a comprehensive, multicomponent school based randomized trial. Food Nutr Res 59:25932. doi:10.3402/fnr.v59.25932
Ahmadi N, Black JL, Velazquez CE, Chapman GE, Veenstra G (2015) Associations between socio-economic status and school-day dietary intake in a sample of grade 5–8 students in Vancouver, Canada. Public Health Nutr 18(5):764–773. doi:10.1017/S1368980014001499
Rahmati A, Tossell C, Shepard C, Kortum P, Zhong L (2012) Exploring iPhone usage: the influence of socioeconomic differences on smartphone adoption, usage and usability. In: MobileHCI’12, September 21–24, San Francisco, CA, USA
Thomas S, Heinrich S, Kühnlein A, Radon K (2010) The association between socioeconomic status and exposure to mobile telecommunication networks in children and adolescents. Bioelectromagnetics 31(1):20–27
Acknowledgements
Sources of support: HELENA study received funding from the European Community Sixth RTD Framework Programme (Contract FOODCT-2005-007034). Additional support from the Spanish Ministry of Education (AGL2007-29784-E/ALI), Axis-Shield Diagnostics Ltd (Oslo, Norway), Abbot Científica S.A. (Spain). This analysis was also supported by the Spanish Ministry of Science and Innovation (JCI-2010-07055) with the contribution of the European Regional Development Fund (FEDER). The study is supported by a grant from the Spanish Carlos III Health Institute: RD08/0072/0025 (Red SAMID: Maternal, Child Health and Development Research Network) and CIBEROBN. The content of this article reflects only the author’s views, and the European Community is not liable for any use that may be made of the information contained herein. Additional contributions: We thank all members of the study teams and especially the adolescents and their parents for their participation in the study.
Members of the HELENA Study Group
Coordinator Luis A. Moreno; Core Group members Luis A. Moreno, Fréderic Gottrand, Stefaan De Henauw, Marcela González-Gross, and Chantal Gilbert; Steering Committee Anthony Kafatos (President), Luis A. Moreno, Christian Libersa, Stefaan De Henauw, Sara Castelló, Fréderic Gottrand, Mathilde Kersting, Michael Sjöstrom, Dénes Molnar, Marcela González-Gross, Jean Dallongeville, Chantal Gilbert, Gunnar Hall, Lea Maes, and Luca Scalfi; Project Manager Pilar Meléndez; Universidad de Zaragoza, Zaragoza, Spain Luis A. Moreno, Jesús Fleta, José A. Casajús, Gerardo Rodríguez, Concepción Tomás, María I. Mesana, Germán Vicente-Rodríguez, Adoración Villarroya, Carlos M. Gil, Ignacio Ara, Juan Revenga, Carmen Lachen, Juan M. Fernández Alvira, Gloria Bueno, Aurora Lázaro, Olga Bueno, Juan F. León, Jesús M. Garagorri, Manuel Bueno, Juan Pablo Rey López, Iris Iglesia, Paula Velasco, Silvia Bel, Luis A. Gracia Marco, and Theodora Mouratidou; Consejo Superior de Investigaciones Científicas, Madrid Ascensión Marcos, Julia Wärnberg, Esther Nova, Sonia Gómez, Ligia Esperanza Díaz, Javier Romeo, Ana Veses, Belén Zapatera, Tamara Pozo, and David Martínez; Université de Lille 2, Lille, France Laurent Beghin, Christian Libersa, Frédéric Gottrand, Catalina Iliescu, and Juliana Von Berlepsch; Research Institute of Child Nutrition Dortmund, Rheinische Friedrich-Wilhelms-Universität Bonn, Bonn, Germany Mathilde Kersting, Wolfgang Sichert-Hellert, and Ellen Koeppen; Pécsi Tudományegyetem, University of Pécs, Pécs, Hungary Dénes Molnar, Eva Erhardt, Katalin Csernus, Katalin Török, Szilvia Bokor, Angela Angster, Enikö Nagy, Orsolya Kovács, and Judit Répasi; University of Crete School of Medicine, Heraklion, Greece Anthony Kafatos, Caroline Codrington, María Plada, Angeliki Papadaki, Katerina Sarri, Anna Viskadourou, Christos Hatzis, Michael Kiriakakis, George Tsibinos, Constantine Vardavas, Manolis Sbokos, Eva Protoyeraki, and Maria Fasoulaki; Institut für Ernährungs und Lebensmittelwissenschaften–Ernährungphysiologie, Rheinische Friedrich-Wilhelms-Universität Bonn Peter Stehle, Klaus Pietrzik, Marcela González-Gross, Christina Breidenassel, Andre Spinneker, Jasmin Al-Tahan, Miriam Segoviano, Anke Berchtold, Christine Bierschbach, Erika Blatzheim, Adelheid Schuch, and Petra Pickert; University of Granada, Granada, Spain Manuel J. Castillo, Ángel Gutiérrez, Francisco B. Ortega, Jonatan R. Ruiz, Enrique G. Artero, Vanesa España, David Jiménez-Pavón, Palma Chillón, Cristóbal Sánchez-Muñoz, and Magdalena Cuenca-García; Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione, Roma, Italy Davide Arcella, Elena Azzini, Emma Barrison, Noemi Bevilacqua, Pasquale Buonocore, Giovina Catasta, Laura Censi, Donatella Ciarapica, Paola D’Acapito, Marika Ferrari, Myriam Galfo, Cinzia Le Donne, Catherine Leclercq, Giuseppe Maiani, Beatrice Mauro, Lorenza Mistura, Antonella Pasquali, Raffaela Piccinelli, Angela Polito, Raffaella Spada, Stefania Sette, and Maria Zaccaria; Department of Food Science, University of Napoli Federico II, Naples, Italy Luca Scalfi, Paola Vitaglione, and Concetta Montagnese; Ghent University, Ghent, Belgium Ilse De Bourdeaudhuij, Stefaan De Henauw, Tineke De Vriendt, Lea Maes, Christophe Matthys, Carine Vereecken, Mieke de Maeyer, Charlene Ottevaere, and Inge Huybrechts. Medical University of Vienna, Vienna, Austria Kurt Widhalm, Katharina Phillipp, Sabine Dietrich, Birgit Kubelka, and Marion Boriss-Riedl; Harokopio University, Athens, Greece Yannis Manios, Eva Grammatikaki, Zoi Bouloubasi, Tina Louisa Cook, Sofia Eleutheriou, Orsalia Consta, George Moschonis, Ioanna Katsaroli, George Kraniou, Stalo Papoutsou, Despoina Keke, Ioanna Petraki, Elena Bellou, Sofia Tanagra, Kostalenia Kallianoti, Dionysia Argyropoulou, Katerina Kondaki, Stamatoula Tsikrika, and Christos Karaiskos; Institut Pasteur de Lille, Lille Jean Dallongeville and Aline Meirhaeghe; Karolinska Institutet, Huddinge, Sweden Michael Sjöstrom, Jonatan R. Ruiz, Francisco B. Ortega, María Hagströmer, Anita Hurtig Wennlöf, Lena Hallström, Emma Patterson, Lydia Kwak, Julia Wärnberg, and Nico Rizzo; Asociación de Investigación de la Industria Agroalimentaria, Paterna, Spain Jackie Sánchez-Molero, Sara Castelló, Elena Picó, Maite Navarro, Blanca Viadel, José Enrique Carreres, Gema Merino, Rosa Sanjuán, María Lorente, and María José Sánchez; Campden BRI, Chipping Campden, Gloucestershire, United Kingdom Chantal Gilbert, Sarah Thomas, Elaine Allchurch, and Peter Burgess; SIK Institutet foer Livsmedel och Bioteknik, Gothenburg, Sweden Gunnar Hall, Annika Astrom, Anna Sverkén, and Agneta Broberg; Meurice Research and Development asbl, Brussels, Belgium Annick Masson, Claire Lehoux, Pascal Brabant, Philippe Pate, and Laurence Fontaine; Campden and Chorleywood Food Development Institute, Budapest, Hungary Andras Sebok, Tunde Kuti, and Adrienn Hegyi; Productos Aditivos SA, Barcelona, Spain Cristina Maldonado and Ana Llorente; Cárnicas Serrano SL, Paterna, Spain Emilio García; Cederroth International AB, Sverige, Sweden Holger von Fircks, Marianne Lilja Hallberg, and Maria Messerer; Lantmännen Food R&D, Malmö, Sweden Mats Larsson, Helena Fredriksson, Viola Adamsson, and Ingmar Börjesson; European Food Information Council, Brussels Laura Fernández, Laura Smillie, and Josephine Wills; Universidad Politécnica de Madrid, Madrid Marcela González-Gross, Jara Valtueña, David Jiménez-Pavón, Ulrike Albers, Raquel Pedrero, Agustín Meléndez, Pedro J. Benito, Juan José Gómez Lorente, David Cañada, Alejandro Urzanqui, Rosa María Torres, and Paloma Navarro.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
All studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed consent prior to their inclusion in the study.
Rights and permissions
About this article

Cite this article
Mesana, M.I., Hilbig, A., Androutsos, O. et al. Dietary sources of sugars in adolescents’ diet: the HELENA study. Eur J Nutr 57, 629–641 (2018). https://doi.org/10.1007/s00394-016-1349-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-016-1349-z