
Abstract
Purpose
Obesity is a global epidemic affecting around 10 % of 5- to 17-year olds. With the causes for obesity being multifactorial, a better understanding of the influencing factors is essential for effective treatment and prevention programs. The aim of this study was therefore to identify specific risk factors for overweight and obesity in children in Switzerland.
Methods
A nationally representative sample of children aged 6–12 years was recruited (n = 2724). Height and weight were measured to calculate BMI (kg/m2). In addition, a questionnaire was distributed to all children asking about their physical activity, media consumption, and dietary habits as well as some parental factors.
Results
The prevalence of overweight and obesity in boys was 11.8 and 7.5 %, respectively, and in girls, it was 11.9 and 5.7 %. In univariate analyses, a number of parental, dietary, and activity factors were shown to be associated with BMI category. Based on a multinomial logistic regression, parent nationality and media consumption were the most important factors predicting obesity in boys, while in girls it was parental education, nationality, and physical activity.
Conclusion
We have demonstrated that parental nationality and education play an important role in the development of childhood obesity, together with media consumption and physical activity. However, risk factors are also different according to child gender. Thus, an important target group for the treatment and prevention of childhood obesity in Switzerland are immigrant families, and the problem needs to be tackled differently in boys and girls as their risk factors are not the same.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity has long been considered a global epidemic. The World Health Organization (WHO) and World Obesity Clinical Care estimate that in 2008 more than 1.4 billion adults and in 2004 around 10 % of children aged 5–17 years were overweight globally [1, 2]. Despite observed trends for a stabilization of the prevalence of childhood obesity in several countries, it is unclear how the overall epidemic can be stopped [3]. From an international point of view, the rates of childhood overweight and obesity in Switzerland are low, with a total prevalence (overweight and obesity together) of 19 % [4] compared to 34 % in the USA, 59 % in Mexico, and 31 % in Spain [5]. Furthermore, we have recently demonstrated that the prevalence of childhood adiposity in Switzerland stabilized between 1999 and 2012 [4]. Nevertheless, as obesity during childhood is a risk factor not only for short-term health consequences [6] but also for obesity and its associated comorbidities in adulthood [7], the ultimate goal should be to reduce its prevalence even further.
Even though the direct reason for weight gain is generally a positive energy balance, the causes for obesity are multifactorial. Changes in food habits; an increasingly sedentary lifestyle; and genetic, social, and cultural factors have been named as important factors influencing the prevalence of obesity, and consequently, treatment possibilities are multiple. Lifestyle interventions comprised of several treatment aspects are generally recommended for the treatment of childhood obesity [8–10]. Although such approaches have been shown to be effective in randomized controlled trials, the amount of weight lost is limited, and many children are unsuccessful over the long term [8]. Alternative treatment options such as medication or bariatric surgery can be explored for severely obese children [9], but ideally, the prevention of the development of obesity should be emphasized.
Population-based prevention approaches which address obesity and specifically childhood obesity through multistrategic interventions have been suggested as the method of choice and have already been implemented in several settings [11, 12]. Even though a recent review by Wolfenden suggested a modest positive effect of such population-based programs, not all included studies reached the same conclusion [13]. A better understanding of the importance of different factors in the development of childhood obesity is required for the development of more targeted and therefore more successful strategies.
The aim of this study was therefore to identify specific risk factors for overweight and obesity in a representative national sample of Swiss primary school children aged 6–12 years, by testing factorial associations with weight status. Specifically, associations between diet, leisure time activity and socioeconomic components, and the risk of overweight and obesity were examined.
Methods
Subjects
A probability proportionate-to-size (PPS) cluster sampling was used to obtain a representative national sample of Swiss children aged 6–12 years. PPS cluster sampling is a widely used and recommended method for anthropometric school-based surveys. Based on current census data, the Swiss Federal Office of Statistics divided Switzerland into five geographic regions: west (French language), northwest (German language), northeast (German language), central east (German language), and south (Italian language). Each of these regions was divided into three strata by population size of the communities (i.e., small communities: <10,000 inhabitants; middle-sized communities: 10,000–100,000 inhabitants; and large communities >100,000 inhabitants). Then, a two-stage PPS random cluster sampling was used to obtain independent national samples of the population groups. One school in each of the 60 communities was identified by stratified random selection. Schools that declined participation were systematically replaced by another randomly selected school from the same strata (sampling stage 1). Per school, 3–4 classrooms were randomly selected, and all students from these classrooms were invited to participate (sampling stage 2).
An information letter describing the study and the examination process was sent to the school principal, teachers, parents, and children 2 weeks prior to the measurement day in order to give parents/children sufficient time to consider participation. Children were automatically enrolled in the study, but parents had the possibility to withdraw their child from the survey by letter (passive informed consent). Data were collected from February to June 2012, and ethical approval was obtained from the Ethical Commission of the ETH Zurich (Zurich, Switzerland) and the Cantonal Ethic Committee Vaud (Lausanne, Switzerland).
Anthropometric measurements
For the anthropometric measurements, which took place over the entire school day, children left the classroom in pairs, and measurements were taken in a separate room. Children removed their shoes, emptied their pockets, and wore light indoor clothing. All measurements were taken by two trained examiners (S.B.M. and S.S.). Height and weight were measured using standard anthropometric techniques [14]. Body weight was measured to the nearest 0.1 kg using a digital scale (PS22; Breuer, Ulm, Germany). Height was measured to the nearest 0.1 cm using a portable stadiometer (Seca 214; Seca Medizinische Waagen und Messsysteme, Hamburg, Germany).
Sex and date of birth were obtained from the school lists. In the case of missing data, they were established at the time of examination.
Questionnaire
After the anthropometric measurements, a questionnaire was distributed to all participating children to gather information about parental characteristics, in addition to the child’s physical activity behavior, media consumption, and dietary habits. The questions used were derived from a validated questionnaire used in the same age group by the Institute of Movement Sciences at ETH, Zurich, and from a collection of standard questions published by the Federal Institute of Public Health [15]. Children were advised to fill out the questionnaire at home with the assistance of a parent, and who filled in the answers was specified at the beginning of the questionnaire. Questionnaires completion was voluntary and anonymous. To provide anonymity, each child was assigned a subject identification number as part of the anthropometric examination, which was then used on the questionnaires and forms throughout the study. The questionnaires were collected by teachers and sent back to us by mail. Data entry was via a standardized procedure, undertaken by two trained persons (S.S. and J.Z.).
Parental characteristics
The questionnaire included an open question regarding the nationalities of both parents. For the analysis, the nationalities of the parents were combined and categorized into the following three groups: “Both Swiss,” “Swiss and non-Swiss,” and “Both non-Swiss.” Furthermore, the education level of both parents was surveyed, with the following possible responses “obligatory school time,” “apprenticeship without professional maturity,” “apprenticeship with professional maturity,” “university of applied sciences or technical university,” and “university.” The educational levels of the parents were combined and categorized into the following three groups: “low” (obligatory school time), “moderate” (apprenticeship with or without professional maturity), and “high” (university of applied sciences, technical university or university).
Physical activity
The children were asked for how many days in a typical week they were physically active for ≥60 min. Physical activity was defined as any body movement that leads to an increase in heart rate and respiration, and includes light sweating. Answers were categorized as follows: “≤1 day/week,” “2–3 days/week,” “4–5 days/week,” and “≥6 days/week.” The question specifically asked about physical activity outside school, so any physical activity classes during normal school hours were not included.
Media consumption
The children were asked how many hours and minutes in a typical day they watched television (including videos, DVD), played PlayStation or other video games, and used a computer (including surfing the Internet). The respective times for each activity were summed up to form the variable media consumption. Media consumption was categorized into “<1 h/day,” “≥1 and <2 h/day,” “≥2 and <3 h/day,” and “≥3 h/day.”
Dietary intakes and dietary habits
The questionnaire gathered information on both dietary intakes and dietary habits with respect to mealtime behaviors. The children were asked how many times they consumed the following food items during the last 4 weeks: soft drinks, fruits, vegetables, and green salad. The possible responses were “never or rarely,” “1–3 times/month,” “once/week,” “2–4 times/week,” “5–6 times/week,” “once/day,” “twice/day,” “3 times/day,” and “4–5 times/day.” For soft drinks, the children were categorized into following consumer categories: “≤1 day/week,” “2–4 days/week,” “5–6 days/week,” and “daily.” The intakes of fruits, vegetables, and green salad were summed up to form the variable fruit and vegetable intake, which was categorized into “<once/day,” “1–2 times/day,” “3–4 times/day,” and “≥5 times/day.” Regarding dietary habits, the children were asked whether they eat breakfast. Subjects could choose between “yes,” “no,” and “sometimes.” For the multinomial logistic regression analysis, the groups “no” and “sometimes” were combined to obtain the following two groups: “no” (not eating breakfast regularly) and “yes” (eating breakfast regularly). Additionally, the children were asked how many times per week they eat a family supper or in front of the television/computer. The possible answers were “<once/week,” “1–2 times/week,” “3–4 times a week,” and “≥5 times/week.”
Data analysis
All data were thoroughly checked for data entry errors. The exact ages of the children were calculated from the date of birth and date of anthropometric measurement. Children <6.0 and ≥13.0 years were excluded from the data analysis.
BMI was calculated as weight (kg) divided by height squared (m2). Overweight (excluding obesity) and obesity were defined according to the age- and sex-specific 85th and 95th BMI percentiles, respectively, of the Centers for Disease Control and Prevention (CDC) [16]. As there is no national growth reference dataset for Swiss children, we previously validated the accuracy of the CDC criteria in classifying adiposity, estimated by measuring multiple skinfold thicknesses, in a national sample of Swiss children at this age [17]. In both sexes, the sensitivity and specificity of the CDC criteria in defining overweight and obesity was found to be high and superior to that of the International Obesity Task Force criteria [17]. BMI–standard deviation scores (BMI–SDS) were calculated using the software Epi Info version 3.5.3 (Centers for Disease Control and Prevention, Atlanta, GA, USA) to compare BMI values across different ages and by sex. A more detailed presentation of overweight and obesity prevalence of the study population as well as time trends in Switzerland using both CDC and International Obesity Task Force (IOTF) criteria for childhood obesity has been published elsewhere [4].
Statistical analysis was done using IBM SPSS Statistics version 20 (IBM Company, Armonk, NY, USA) and Excel (Microsoft Office 2010; Microsoft Corporation, Redmond, WA, USA). Continuous data were checked for normal distribution using a Kolmogorov–Smirnov test and graphically by evaluating histograms and Q–Q plots. Non-normally distributed data were log-transformed before data analysis and expressed as median (Min–Max) (i.e., BMI–SDS). No suitable transformation could be found for age, and therefore, nonparametric testing was applied for this variable. For the comparison of continuous data between sexes, independent t test for parametric and Mann–Whitney U test for nonparametric variables were used. One-way ANOVA followed by Bonferroni post hoc testing was performed to check for significant differences among the three age groups (6–8, 9–10, 11–12 years) for normally distributed continuous variables. Prevalence estimates of overweight and obesity between sexes and the three age groups were compared using the Chi-square test, followed by the z test to check for significant differences between the individual values (Bonferroni correction). Chi-square testing was further used to check for associations between BMI categories and socioeconomic, dietary or activity parameters. Multinomial logistic regressions were used to examine the associations between BMI category and risk factors (i.e., parental characteristics and child’s lifestyle habits). In a first step, each risk factor was tested individually (dependent variable: BMI category; factor: each of the risk factors). In a second step, all risk factors which showed an association in the univariate model were added into the multivariate model, controlling for age in addition (dependent variable: BMI category; factors: all risk factors; covariate: age). p values <0.05 were considered significant.
Results
Response rates
In total, 3239 children attending the consenting schools were invited to participate in the study. Of those, 177 children did not participate (77 children/parents declined participation, and 100 children were absent on the day of measurement due to illness or other reasons) resulting in a participation rate of 94.5 % (n = 3062) [4]. The return rate of the distributed questionnaires was 91.7 % (n = 2808), and only children who filled in the questionnaires were considered for the analysis in this publication. After discarding data from nine children due to missing age, 68 children as they were either <6.0 or ≥13.0 years of age, and 7 children because of non-identifiable questionnaires, a final sample size of 2724 children remained.
Study population characteristics
The final sample consisted of 1375 boys [median age (range) 9.83 (6.36–12.98) years] and 1349 girls [median age (range) 9.94 (6.25–12.99) years]. Median (range) BMI–SDS was 0.8 (−3.2 to 5.6) in boys and 0.6 (−2.7 to 4.6) in girls, and did not differ between sexes and age groups (p > 0.05). The prevalence estimates of overweight and obesity by sex and age groups are shown in Table 1. There was no sex difference in prevalence rates of overweight and obesity in all age groups (p > 0.05), although a clear trend toward higher obesity rates in boys was apparent with the exception of the 9- to 10-year olds. In addition, for both sexes, no age effect was observed for either overweight or obesity (p > 0.05).
Risk factors for overweight and obesity
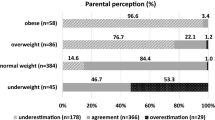
Prevalence estimates of overweight and obesity by nationality and education level of the parents are shown in Fig. 1. There was a significant association between parents’ nationality and BMI category, both in boys (χ 2(4) = 46.1, p < 0.001) and in girls (χ 2(4) = 32.4, p < 0.001). Furthermore, a significant relationship between parental education level and BMI category in boys (χ 2(4) = 13.9, p = 0.008) and girls (χ 2(4) = 25.9, p < 0.001) was found (Fig. 1).

Prevalence (±SE) of overweight (excluding obesity) and obesity in Swiss children aged 6–12 years in 2012 by nationality and education level of the parents, using the Centers for Disease Control and Prevention (CDC) Ref. [16]. a Prevalence was significantly different from “both Swiss” group, p < 0.05 (z test, Bonferroni correction); b prevalence was significantly different from “highly educated” group, p < 0.05 (z test, Bonferroni correction)
Several dietary parameters were investigated for their effect on BMI. Not eating breakfast was significantly associated with BMI category in both boys (χ 2(2) = 8.9, p = 0.012) and girls (χ 2(2) = 15.6, p < 0.001). Similarly, there was a significant association between the number of days that children consume lunch at school and BMI categories in both boys (χ 2(8) = 19.1, p = 0.014) and girls (χ 2(8) = 37.1, p < 0.001), while the effect of family supper seems to be less important in both groups [(χ 2(6) = 12.6, p = 0.050) for boys and (χ 2(6) = 9.6, p = 0.143) for girls]. Eating in front of the TV, on the other hand, was related to BMI categories in boys (χ 2(6) = 23.7, p = 0.001) but not in girls (χ 2(6) = 11.1, p = 0.086). The consumption of fruits and vegetables was associated with BMI categories in girls (χ 2(8) = 18.3, p = 0.019) but not in boys (χ 2(8) = 10.5, p = 0.232), while soft drink consumption was not found to be significantly associated in either boys (χ 2(6) = 2.7, p = 0.850) or girls (χ 2(6) = 7.6, p = 0.273).
In a last step, the impact of physical activity and inactivity was investigated. Media consumption was significantly associated with BMI categories in both boys (χ 2(6) = 46.9, p < 0.001) and girls (χ 2(6) = 33.3, p < 0.001), while physical activity (as frequency categories) was only significantly associated with BMI categories in girls (χ 2(6) = 21.0, p = 0.002) with a trend for boys (χ 2(6) = 11.9, p = 0.064).
The following risk factors showed significant associations with BMI categories in individual multinomial logistic regression and were thus used for the multivariate model: parents’ nationality, parental education, physical activity, media consumption, and breakfast consumption (data not shown). Results of the multivariate model are displayed in Table 2 for boys and in Table 3 for girls. The model shows the odds ratio (OR) for obesity to be significantly increased in boys if they have at least one non-Swiss parent and with increasing media consumption; similar results can be seen for overweight but to lower extent (Table 2). In girls, the OR for obesity was significantly increased only if they have two non-Swiss parents, and media consumption was also a less important predictor. On the other hand, the girls’ OR for obesity was significantly increased based on the parents’ education level, and there was a trend for reduced physical activity and skipping breakfast to be a contributing factor. The OR for overweight in girls, however, was strongly increased with increasing media consumption (Table 3).
Discussion
The etiology of obesity is multifactorial, and for successful prevention, a detailed understanding of the specific risk factors is essential. We have investigated dietary, leisure time activity, and socioeconomic factors for their role in childhood overweight and obesity in a representative sample of schoolchildren in Switzerland. In boys, the risk of obesity was clearly dependent on the parent’s nationality and increased with increasing media consumption. In girls, on the other hand, the associations were less pronounced; however, media consumption, parent’s nationality, parental education, and physical activity seemed to play a role in their risk of overweight and obesity.
Unhealthy dietary habits are often cited as a main cause for the obesity epidemic; however, exactly which foods may be responsible is still a matter of debate, and it seems increasingly obvious that changing individual aspects of the diet and/or lifestyle is unlikely to achieve any long-term improvements [10]. Nevertheless, high consumption of fruits and vegetables, for example, has been associated not only with reduced BMI [18], but also other positive effects such as protection against cancer [19] and cardiovascular disease [20]. Consequently, higher intakes of fruits and vegetables have been promoted worldwide using different campaigns, with ‘5 a day’ being probably the most widely used. Despite the popularity of such programs, a recent systematic review concluded that family-focused interventions to increase daily fruit and vegetable intake had a very limited success rate, and that holistic approaches were needed [10]. The Health Behaviour in School-Aged Children (HBSC) study has, besides other factors, assessed the consumption of fruits in 11-, 13-, and 15-year-old schoolchildren in 39 countries. In Switzerland, 50 % of 11-year-old, 43 % of 13-year-old, and 35 % of 15-year-old children reported eating fruits daily. Even though this was high compared to internationally, these results indicate that more than 50 % of the children in Switzerland do not follow recommendations [21]. Nevertheless, in our study, we have not found children with a low consumption of fruits and vegetable to be at an increased risk of obesity in the multinomial model, even though at least for girls the overweight and obese groups showed a reduced frequency of fruit and vegetable consumption. Due to their high sugar content, soft drinks are often linked to an increased risk of obesity, even though the actual effect of a reduction in their consumption on body weight is still debated [22–24]. In our study, soft drink consumption was not associated with the risk of obesity either in boys or in girls. Regarding fruit and vegetable intakes and the risk of obesity, our results are comparable to a previous study conducted in Canadian children; however, in this study, a significant effect of soft drink consumption was reported [25]. A study in Greek adolescents, on the other hand, found even less impact then we did: the frequency of fruit and vegetable intake or of the consumption of soft drinks did not differ between the normal weight and the overweight/obese group [26]. Furthermore, data from 34 countries participating in the HBSC 2001/2002 study indicate that the consumption of fruits, vegetables, and soft drink influenced the OR for obesity in only a few exceptional cases [27]. This lack of association in our study may, to a certain extent, be the result of the quantitative questions asked. By only asking about frequencies, it was not possible to assess the actual amounts consumed, and thus, it may not have been possible to pick up all associations. Particularly for soft drinks, quantities may vary considerably between children. Nevertheless, questions asked were similar to those in the HBSC survey that also did not assess actual amounts but only frequencies. Thus, the fact that we did not find associations between fruit and vegetable as well as soft drink consumption may also be due to differences in overall eating patterns between Switzerland and other countries. For example, the HBSC survey showed that daily consumption of soft drinks and also fruits in Switzerland did not differ between affluent and less affluent families, while there were important differences in a large number of other European countries [21].
In an earlier Swiss study, children consuming breakfast frequently were shown to have a lower BMI compared to those skipping breakfast on a regular basis [28]. Similar findings were reported in other studies summarized by Rampersaud et al. [29]. In the present study, we found skipping breakfast to be more prevalent in overweight and obese children, but when controlling for other influencing factors in the multinomial model, only a trend remained for an increased risk of obesity in girls. Thus, even though skipping breakfast seems to be more frequent in overweight and obese children, other factors may be more important in determining the risk of overweight and obesity.
As weight gain is generally accepted to be the result of a positive energy balance, energy expenditure needs to be considered besides energy intake. In our study, we found increasing media consumption to be an important risk factor for obesity and to some extent also overweight, especially in boys, while in girls the associations were less clear. The amount of active physical activity, on the other hand, seemed to play only a limited role, at least when controlling for all other factors in the multinomial model. Contrary to this finding, the HBSC 2001/2002 data indicate a strong influence on obesity risk by physical activity level and TV viewing time, but not computer use [27]. Then again, Kosti et al. [26] showed that physical activity was reduced in overweight and obese Greek adolescents, while they reported no difference in the time watching TV or playing electronic games. Despite the existing discrepancies in these studies, which may to a certain extent be also the result of differences in the assessment methods, it becomes evident that physical activity and inactivity are important influencing factors when it comes to childhood overweight and obesity. One of the striking differences in our study compared to others is that media consumption seems to be one of the two main determining factors for obesity in boys, but was found to be much less important in girls. This may be explained to a large extent by the fact that the proportion of obese boys with media consumption >3 h/day is considerably higher than it is in girls (25.5 vs. 15.6 %).
Besides direct energy intake and energy expenditure, parental factors, including socioeconomic status as well as parental weight, have been discussed as important predictors of children’s weight status [30–32]. In our study, we have not been able to assess parental weight, but we did investigate the effect of parental education and migrant status on the child’s risk of overweight and obesity. We have found significantly higher frequencies of overweight and obesity in children from parents with lower education as well as non-Swiss nationality. Our data confirm findings of a previous study done in preschool children in Switzerland where parental education level and migration status were also found to be important predictors not only of child obesity but also of eating habits [33]. Similarly, Lasserre et al. [34] reported a strong influence of parental factors including weight, education, and migrant status in a regional sample of Swiss schoolchildren (Canton Vaud), but in this study dietary factors and physical activity were not considered. Migrant status and nationality were also determined as important contributing factors to childhood obesity in other countries including Germany [35] and the Netherlands [36], but most other surveys have focused more on socioeconomic status. The determination of socioeconomic status varies widely between studies. It can be based on living area, parent’s employment, or as in our study, education. Even though the prevalence of overweight and obesity was higher in children from parents with a lower education level in our study, parental education was not found to be a determinant for the risk of obesity in boys when controlling for other factors and the effect in girls was only limited. Similarly, the most recent Health Survey for England (HSE) showed a higher prevalence of overweight and obesity in children from families with lower household income [37]. Higher overweight and obesity prevalence in groups with lower socioeconomic status based on neighborhood was shown in a study in 10-year-old children in Stockholm County in Sweden, without investigating other influencing factors such as diet or physical activity [38]. Also in agreement with our findings, a French study that used composite index of socioeconomic status including household wealth, education level, and occupational status of the household head found the OR for children to be overweight and/or obese was significantly increased in the lowest group compared to the highest, but the analysis was only controlled for age and sex [39]. Thus, even though studies from other countries have found similarly increased prevalence for overweight and obesity in children from lower socioeconomic background as we did in our current report, generally they did not control for other potential influencing factors.
A limitation of the current study is certainly that we have not been able to assess socioeconomic status of the families in detail but have relied on migration status and education level of the parents. The fact that we have used self-reported data to assess the risk factors has to be considered as a further limitation, as it is very difficult to accurately assess dietary factors and to a certain extent also physical activity in this way. Nevertheless, the fact that we have been able to include a nationally representative sample of schoolchildren living in Switzerland and that we have assessed dietary factors, physical activity, and inactivity as well as parental factors certainly counterbalances the limitations and has allowed us to carry out a very broad analysis of risk factors for childhood overweight and obesity in Switzerland.
In conclusion, the data from our survey indicate that, looking at individual parameters, several dietary, activity, and parental factors seem to be related to the prevalence of childhood overweight and obesity in our representative sample of schoolchildren living in Switzerland. When combining all potential influencing factors in one model, overweight and obesity were associated with parental nationality and media consumption in boys, while in girls parental education and physical activity played a predominant role. Therefore, our results indicate that an important target group for treatment and prevention of childhood obesity in Switzerland are immigrant families, but also that the problem needs to be tackled differently in boys and girls as their risk factors are not the same.
References
World Obesity (2014) Childhood obesity. (cited 2014 22.12.2014). http://www.worldobesity.org/aboutobesity/child-obesity/
WHO (2014) Obesity and overweight: fact sheet no 311. (cited 2014 29.07.2014). http://www.who.int/mediacentre/factsheets/fs311/en/
Olds T et al (2011) Evidence that the prevalence of childhood overweight is plateauing: data from nine countries. Int J Pediatr Obes 6(5–6):342–360. doi:10.3109/17477166.2011.605895
Murer SB et al (2013) Pediatric adiposity stabilized in Switzerland between 1999 and 2012. Eur J Nutr. doi:10.1007/s00394-013-0590-y
World Obesity (2014) (cited 2014 29.07.2014). http://www.worldobesity.org/aboutobesity/world-map-obesity/?map=children
Lobstein T et al (2004) Obesity in children and young people: a crisis in public health. Obes Rev 5(Suppl 1):4–104. doi:10.1111/j.1467-789X.2004.00133.x
Singh AS et al (2008) Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev 9(5):474–488. doi:10.1111/j.1467-789X.2008.00475.x
Reinehr T (2013) Lifestyle intervention in childhood obesity: changes and challenges. Nat Rev Endocrinol 9(10):607–614. doi:10.1038/nrendo.2013.149
Kirschenbaum DS, Gierut KJ (2013) Five recent expert recommendations on the treatment of childhood and adolescent obesity: toward an emerging consensus: a stepped care approach. Child Obes 9(5):376. doi:10.1089/chi.2013.0058
Bourke M, Whittaker PJ, Verma A (2014) Are dietary interventions effective at increasing fruit and vegetable consumption among overweight children? A systematic review. J Epidemiol Community Health 68(5):485–490
WHO (2009) WHO forum and technical meeting on population-based prevention strategies for childhood obesity. In Report of the WHO forum and technical meeting. World Health Organization, Geneva
WHO (2012) Population-based approaches to childhood obesity prevention. WHO, Geneva
Wolfenden L et al (2014) A systematic review and meta-analysis of whole of community interventions to prevent excessive population weight gain. Prev Med 62:193–200. doi:10.1016/j.ypmed.2014.01.031
World Health Organization (1995) Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser 854:1–452
Stamm H, Wiegand D, Lamprecht M (2011) Sammlung von Standardfragen für Datenerhebung in der Bereichen Ernährung und Bewegung. Federal Office of Public Health, Zurich
Ogden CL et al (2002) Centers for disease control and prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109(1):45–60
Zimmermann MB et al (2004) Detection of overweight and obesity in a national sample of 6-12-y-old Swiss children: accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and the International Obesity Task Force. Am J Clin Nutr 79(5):838–843
te Velde SJ, Twisk JWR, Brug J (2007) Tracking of fruit and vegetable consumption from adolescence into adulthood and its longitudinal association with overweight. Br J Nutr 98(2):431–438. doi:10.1017/S0007114507721451
Maynard M et al (2003) Fruit, vegetables, and antioxidants in childhood and risk of adult cancer: the Boyd Orr cohort. J Epidemiol Community Health 57(3):218–225. doi:10.1136/jech.57.3.218
Dauchet L et al (2006) Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr 136(10):2588–2593
WHO (2012) Social determinants of health and well-being among young people: health behaviour in school-aged children (HBSC) study 2009/2010. World Health Organization, Copenhagen
Ebbeling CB (2014) Sugar-sweetened beverages and body weight. Curr Opin Lipidol 25(1):1–7. doi:10.1097/Mol.0000000000000035
Hu FB (2013) Resolved: there is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes Rev 14(8):606–619. doi:10.1111/Obr.12040
Kaiser KA et al (2013) Will reducing sugar-sweetened beverage consumption reduce obesity? Evidence supporting conjecture is strong, but evidence when testing effect is weak. Obes Rev 14(8):620–633. doi:10.1111/Obr.12048
Janssen I et al (2004) Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. J Adolesc Health 35(5):360–367. doi:10.1016/j.jadohealth.2003.11.095
Kosti RI et al (2007) Dietary habits, physical activity and prevalence of overweight/obesity among adolescents in Greece: the Vyronas study. Med Sci Monit 13(10):Cr437–Cr444
Janssen I et al (2005) Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes Rev 6(2):123–132. doi:10.1111/j.1467-789X.2005.00176.x
Baldinger N et al (2012) Swiss children consuming breakfast regularly have better motor functional skills and are less overweight than breakfast skippers. J Am Coll Nutr 31(2):87–93
Rampersaud GC et al (2005) Review: breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J Am Diet Assoc 105(5):743–760. doi:10.1016/j.jada.2005.02.007
Whitaker KL et al (2010) Comparing maternal and paternal intergenerational transmission of obesity risk in a large population-based sample. Am J Clin Nutr 91(6):1560–1567. doi:10.3945/ajcn.2009.28838
Knai C et al (2012) Socioeconomic patterning of childhood overweight status in Europe. Int J Environ Res Public Health 9(4):1472–1489. doi:10.3390/ijerph9041472
Keane E et al (2012) Measured parental weight status and familial socio-economic status correlates with childhood overweight and obesity at age 9. Plos One 7(8):e43503. doi:10.1371/journal.pone.0043503
Ebenegger V et al (2011) Independent contribution of parental migrant status and educational level to adiposity and eating habits in preschool children. Eur J Clin Nutr 65(2):210–218. doi:10.1038/ejcn.2010.248
Lasserre AM et al (2007) Overweight in Swiss children and associations with children’s and parents’ characteristics. Obesity 15(12):2912–2919. doi:10.1038/Oby.2007.347
Will B, Zeeb H, Baune BT (2005) Overweight and obesity at school entry among migrant and German children: a cross-sectional study. BMC Public Health 5:45. doi:10.1186/1471-2458-5-45
de Wilde JA et al (2009) Trends in overweight and obesity prevalence in Dutch, Turkish, Moroccan and Surinamese South Asian children in the Netherlands. Arch Dis Child 94(10):795–800. doi:10.1136/adc.2009.163709
HSCIC (2013) Children’s BMI, overweight and obesity, in Health Survey for England: 2012. H.a.S.C.I. Centre, Editor. Health and Social Care Information Centre: Leeds
Sundblom E et al (2008) Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int J Obes 32(10):1525–1530. doi:10.1038/Ijo.2008.104
Lioret S et al (2009) Trends in child overweight rates and energy intake in France from 1999 to 2007: relationships with socioeconomic status. Obesity 17(5):1092–1100. doi:10.1038/Oby.2008.619
Acknowledgments
We would like to thank the principals of all participating schools as well as all teachers and children for their cooperation. Furthermore, we thank Regula Schüpbach, Jasmin Tajeri Foman, and Sara Stinca for their assistance in the study. Financial support for the study was provided by the Swiss Federal Office of Public Health (Bern, Switzerland). The authors’ responsibilities were as follows: SBM and IHA designed research; SBM, SS, and JZ conducted research; SBM and IHA analyzed data; SBM and IHA wrote the paper; SBM and IHA had primary responsibility for final content. All authors have read and approved the final manuscript.
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Murer, S.B., Saarsalu, S., Zimmermann, J. et al. Risk factors for overweight and obesity in Swiss primary school children: results from a representative national survey. Eur J Nutr 55, 621–629 (2016). https://doi.org/10.1007/s00394-015-0882-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-015-0882-5