
Abstract
Purpose
Muffins made with wheat flour are a popular snack consumed in western and emerging countries. This study aimed to examine the content of amylose, glycemic response (GR) and glycemic index (GI) of muffins baked with refined wheat and rice flours, as well as wholegrain corn, oat and barley flours.
Methods
This study adopted a randomized, controlled, crossover, non-blind design. Twelve healthy participants consumed wheat, rice, corn, oat and barley muffins once and the reference glucose solution three times in a random order on non-consecutive day. Capillary blood samples were taken every 15 min in the first 60 min and every 30 min for the remaining 60 min for blood glucose analysis. The Megazyme amylose/amylopectin assay procedure was employed to measure amylose content.
Results
The GR elicited from the consumption of wheat, rice and corn muffins was comparable between these samples but significantly greater when compared with oat and barley muffins. Consumption of wholegrain muffins, apart from corn muffin, blunted postprandial GR when compared with muffins baked with refined cereal flours. Muffins baked with wheat, rice, corn, oat and barley flours gave rise to GI values of 74, 79, 74, 53 and 55, respectively. The content of amylose was significantly higher in corn, oat and barley muffins than wheat and rice muffins.
Conclusions
The greater content of amylose and fibre may play a part in the reduced glycemic potency of oat and barley muffins. Wheat flour can be substituted with oat and barley flours for healthier muffins and other bakery products.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cereals form a cluster of food grains. Wheat, rice and corn remain the dominant cereals worldwide consumed as refined grains together with the minor oat, barley, rye, triticale, sorghum and millet. Cereal grains contain starch granules with different morphology and molecular structure, amylose and amylopectin ratio, nutrient compositions including dietary fibre, protein, lipid and phenolic [1]. These factors can greatly influence the digestibility of starch and thereby resulting in different glycemic index (GI) of cereals. GI is a system of classifying carbohydrate-containing foods according to the extent to which they raise blood glucose levels after ingestion. Cereal grains are commonly processed into a wide range of grain products such as bread, pastries, cookies, breakfast cereals, pasta and noodle. Both cereal grains and grain products are important sources of carbohydrates providing not merely energy but also an increased glycemic load (GL). GL is a concept mathematically derived by combining GI and the amount of carbohydrate intake intended to represent the overall glycemic effect of a diet [2].
Consumers are increasingly purchasing convenient baked goods owing to changing eating patterns. Muffins baked with wheat flour are a popular snack widely consumed in both western and emerging countries. A recent study by the authors revealed that in vitro starch digestibility of muffins baked with rice, wheat, corn, oat and barley flours differed considerably depending on the source of cereals [3]. Rapidly digested starch (RDS) was greatest in rice and wheat muffins, followed by oat, corn and barley. RDS is a reflection of the amount of readily digestible starch in food that is largely accountable for the short-term postprandial glycemic response (GR) seen in in vivo human studies [4]. The presence of lower RDS could make oat, corn and barley muffin an ideal snack for the consumer to modulate GR.
In Asia, the increasing prevalence of obesity could be attributed to the high consumption of starch-based foods high in GR rather than sugar alone [5]. Overconsumption of starchy foods high in glycemic potential will trigger a rapid and sharp increase in blood sugar in turn increases insulin secretion, which has implications in the aetiology of diabetes [6]. Epidemiologic studies have revealed the preventive role of consuming low GI foods against development of diabetes and obesity [2]. Evidence-based dietary guideline can therefore be the cornerstone for improving glycemic control as the prevalence of diabetes has reached pandemic level worldwide. The current study is the first to examine the GR and GI of muffins within a single design baked with a range of cereals notably refined wheat and rice flours, as well as wholegrain corn, oat and barley flours. The amylose content of cereal flours was also determined in order to gain insights into the impact of amylose:amylopectin ratio on GR.
Subjects and methods
Raw materials
Whole grain barley flour (flour 128 g, carbohydrate 76.8 g, fibre 21.4 g, protein 12.8 g, fat 0 g), whole grain oat flour (flour 128 g, carbohydrate 70.4 g, fibre 12.8 g, protein 22.4 g, fat 9.6 g), whole grain yellow corn flour (flour 128 g, carbohydrates 79.5 g, fibre 17.7 g, protein 8.8 g, fat 4.5 g) and white rice flour (flour 128 g, carbohydrates 99.2 g, fibre 3.2 g, protein 6.4 g, fat 1.6 g) were purchased from Bob’s Red Mill (Milwaukie, USA). Refined wheat flour (flour 128 g, carbohydrates 91.0 g, fibre 3.7 g, protein 14.1 g, fat 1.5 g) was purchased from Prima Flour (Singapore). Compositional information was obtained from the suppliers. Baking powder (Bake King, Singapore), fine salt (Pagoda, Singapore), white sugar (SIS, Singapore), milk (Malaysia Dairy Industries, Singapore), sunflower oil (Sunbeam, Singapore) and egg (Seng Choon, Singapore) were obtained from local supermarkets. Pure glucose was purchased from Little Pharmaceutical Suppliers (Singapore).
Test meals
Muffins were prepared in the food preparation laboratory at Clinical Nutrition Research Centre (CNRC) (Singapore). Mixture of flour (128 g), baking powder (5 g), salt (2 g), sugar (50 g), milk (100 ml), sunflower oil (30 g) and one egg was blended at slow speed for 1 min 20 s using an electronic mixer (5KSM150, KichenAid Europa, Inc., Belgium). Muffin batter was then weighed into muffin cups and baked for 20 min at 180 °C in the baking oven (EOB 98000, Electrolux, Sweden). Muffins were served in portions containing 50 g of available carbohydrates, which amounted to 126.1, 119.4, 136.9, 146.8 and 139.7 g of wheat, rice, corn, oat and barley batters, respectively. Muffins were prepared in the evening prior to the test day and stored in air-tight container at 20–22 °C, in order to minimize retrogradation. A glass of water (150 mL) was served with muffins, which the participants had to consume in entirety. A time period of 12 min was allocated to complete the food consumption. As a reference, the glucose solution was prepared from pure glucose (50 g) and water (250 mL) prior to the analysis.
Subjects
The study recruited 12 healthy adults (eight female and four male) by means of advertisements, flyers and personal communication. After questions and concerns about the study protocol were addressed, participants gave their informed consent. This was followed by a health assessment, which included anthropometric measurements and a health questionnaire (giving details of food allergies/intolerances, metabolic diseases, special dietary needs and smoking habits). Those who fulfilled all the inclusion criteria (body mass index 18.0–24.9 kg/m2; blood pressure, between 110 and 120/75 and 85 mm Hg; age 21–50 years; fasting blood glucose 4–6 mmol/L; not on prescription medication; non-smoking; no genetic or metabolic diseases) were included in the study. Physical activity level was quantified using the questionnaire of Baecke et al. [7], and only those not partaking in competitive sports and endurance events were included. Prior to the test day, participants were asked to restrict their intake of alcohol and caffeine-containing drinks, as well as to restrict their participation in intense physical activity. The study was conducted according to the guidelines laid down in the Declaration of Helsinki and was initiated after the approval by the Domain Specific Review Board (DSRB) of National Healthcare Group.
Study protocol
This study adopted a randomized, controlled, crossover, non-blind design. The participants were served with glucose solution on three separate occasions and the test meals on five separate occasions, between 8:30 and 9:30 AM after a 12-h overnight fast. One of the five different test meals was randomly assigned to the participants. The test meals were consumed at a comfortable pace within 15 min. Blood samples were obtained 5 min apart (−5 and 0 min) in the fasting state and at 15, 30, 45, 60, 90 and 120 min subsequent to the start of the meal. The participants were encouraged to keep physical activity to a minimum in the morning before testing. During testing, they were discouraged from walking and were instructed to stay seated. Computers, work desks, reading area and a television were provided to the participants. Upon completion of the eight sessions, the participants were debriefed and compensated for their time and transportation cost.
Blood glucose analysis
The protocol used to measure blood glucose response was adapted from the method described by Brouns et al. [8] and is in line with the procedures recommended by Food and Agricultural Organization/World Health Organization [9]. Blood was obtained by finger prick using the Unistick® 3 single-use lancing device (Owen Mumford, Woodstock, UK). Participants were encouraged to warm their hand to increase blood flow before a finger prick. To minimize plasma dilution, fingertips were not squeezed to extract blood but were instead gently massaged starting from the base of the hand moving towards the tips. The first two drops of expressed blood were discarded, and the third drop was used for testing. Blood glucose was measured using the calibrated HemoCue Glucose 201+ analysers (HemoCue® Ltd, Dronfield, UK). The HemoCue is a reliable method for blood glucose analysis [10]. GR data were converted to “the change in GR” values. The change in GR was calculated by computing the difference between the blood glucose concentration at a time point and mean baseline blood glucose concentration (based on two baseline values taken 5 min apart). Because it represented the relative increment in the GR at any time point compared with the baseline value, it was this change in GR that was used for all further analyses, including incremental area under the curve (IAUC) calculations, blood glucose response curve construction and statistics. The total blood glucose response was expressed as the IAUC ignoring the area beneath the baseline and was calculated geometrically using the trapezoidal rule [7, 11].
Amylose measurement method
The Megazyme amylose/amylopectin assay procedure, utilizing the commercial kit (Megazyme Ireland International, Ltd., Bray, Ireland), was followed according to the manufacturer’s recommendation.
Data processing and statistical analysis
Assessment of GR and GI in vivo was based on 10 subjects to take account of inter-individual variations [8, 9]. A sample size of 12 was therefore considered adequate for the current study. A statistical analysis was conducted using the statistical package for the social sciences (SPSS) version 16 (SPSS Inc, Chicago, Ill). Data and figures were processed in a Microsoft Excel spreadsheet (Microsoft Corporation, Redmond, WA, USA). The IAUC and GI values were subjected to repeated measures ANOVA, and after demonstrating significant heterogeneity, the least significant differences between individual means were obtained by pair-wise comparisons. The amylose content between the muffins was compared using one-way ANOVA performed with Tukey’s test. The criterion for significance was a two-tailed p < 0.05. Pearson’s correlation analysis was used to compare the association between amylose content and GR of muffins, as well as GR of muffins and the RDS.
Results
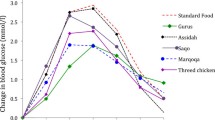
The baseline characteristics of subjects were age 26.2 ± 5.3 years, height 1.6 ± 0.1 m, weight 53.6 ± 7.7 kg, body mass index 20.2 ± 1.7 kg/m2, waist circumference 69.8 ± 7.2 cm and fasting blood glucose 4.6 ± 0.4 mmol/L. All anthropometric data were within the acceptable normal ranges. The mean IAUC elicited from consumption of wheat, rice and corn muffins was comparable but significantly greater when compared with oat and barley muffins (p < 0.05) (Table 1). For the 12 subjects, the coefficient of variation of IAUC elicited from each of the five muffins assayed was <25 %. The incremental blood glucose values during the 2 h after glucose and muffins consumption are shown in Fig. 1. Consumption of muffins baked with wheat, rice, corn, oat and barley flours resulted in distinct temporal GR patterns. The peak GR occurred at 30 min after consumption of wheat, corn and barley muffins as opposed to 45 min after consumption of rice and oat muffins. Wheat, rice and corn muffins demonstrated a greater peak GR compared with barley muffin. The greater initial GR produced by wheat, rice and corn muffins gave rise to higher GI values of 74, 79 and 74, respectively. Barley muffin produced a low and sustained GR during the entire 120-min period, resulting in a medium GI value of 55. A rapid decrease in GR of oat muffin was observed after 45 min, whereas wheat, rice, corn and barley muffins showed a gradual decrease in GR. The reduction in IAUC after 45 min resulted in a medium GI value of 53 for oat muffin. At 120 min, wheat, corn, oat and barley muffins elicited blood glucose concentrations above the baseline value, whereas the GR of rice muffin dipped below baseline. Corn, oat and barley muffins contained significantly higher amylose content than wheat and rice muffins (Fig. 2). An inverse relationship (r = −0.84) was observed between the amylose content and GR of muffins.

Temporal blood glucose responses for glucose solution, wheat, rice, corn, oat and barley muffins. Data are expressed as mean ± SE of three measurements. Temporal blood glucose response curves for glucose square, wheat filled diamond, rice filled circle, corn filled triangle, oat filled square and barley cross muffins

Amylose content in wheat, rice, corn, oat and barley muffins containing 50 g of available carbohydrates. Data are expressed as mean ± SE of three measurements. Bars with different letters indicated significant difference in amylose content (p < 0.05)
Discussion
The mean IAUC elicited from consumption of wheat, rice and corn muffins were significantly greater than oat and barley muffins (p < 0.05). With the exception of corn muffin, whole grain oat and barley muffins blunted postprandial GR when compared with muffins baked with refined wheat and rice flours. The slower release of glucose from the wholegrain muffins could result in moderate change of blood glucose concentration thereby a better control in the kinetics of postprandial blood glucose. This could be substantiated by the lower content of RDS determined in wholegrain muffins than those baked with refined grain flours [3]. A moderate positive relationship (r = 0.60) was observed between GR of muffins and the RDS determined in the previous study. The in vitro method used provides quick and cost-effective indicative data that have been shown to accurately reflect the in vivo glycemic potential of carbohydrate foods [12].
The reduction of fibre content due to the removal of bran and germ from starchy endosperm during milling could have led to the greater glycemic potential of muffins baked with refined wheat and rice flours. Wholegrain corn (6.6 g fibre), oat (5.1 g fibre) and barley (8.1 g fibre) muffins, of which containing 50 g available carbohydrates, were calculated to contain at least five times more fibre than wheat (1.3 g fibre) and rice muffins (1 g fibre). Viscous dietary fibre can increase the viscosity of digesta in the gut thereby inhibiting the propulsive and mixing effects generated by peristalsis and limiting the interaction of the digesta with digestive enzymes [1]. β-glucan, the major component of oat and barley fibre, has been shown effective in reducing postprandial glucose and insulin responses [13]. It may restrict the starch gelatinization by limiting the availability of water for starch hydration [13, 14]. Gelatinization can disrupt the starch granules resulting in a greater susceptibility of starch to enzymatic degradation. The degree of starch gelatinization was reported positively related to GR [15]. In this study, the reduced GR of barley and oat muffins could therefore be attributed to the lower degree of starch gelatinization in the presence of high fibre content particularly β-glucan and their physiological effect in the gastrointestinal system, e.g. delaying the rate of absorption of glucose [16].
At the molecular level, the amount of amylose has been shown negatively correlated with the digestibility of starch [1, 17]. The linearity and hydroxyl groups cause the amylose to orient in parallel forming a more extensive network of hydrogen bonds, thereby limiting the starch gelatinization and accessible of starch to enzyme attack. Barley muffin was noted to contain the greatest amount of amylose, followed by oat and corn muffins, least in wheat and rice muffins (Fig. 2). The higher amount of amylose could therefore in part, explain the significant lower GR of oat and barley muffins than wheat and rice muffins (p < 0.05). After cooking and cooling, amylose in corn may retrograde to resistant starch type 3, which is indigestible starch.
Evident from the wide-ranging RDS content observed in muffins [3], the GR of muffins varied with the cereal flours used for baking. The variability was associated with not only total available carbohydrate but also morphological characteristics of starch granules. A negative relationship has been described between starch granule size and in vitro starch digestibility [18]. The surface of starch granule is also affected by enzyme action. Previous study has detected pinholes in the surface of corn starch, which could have facilitated the entry of the amylases for digestion [19]. These morphological characteristics could possibly explain the greater GR of whole grain corn muffins despite their high fibre and amylose content. In addition, the type of fibre is also of importance. The fibre in corn is mainly insoluble fibre and not soluble (viscous) fibre as in barley and oat.
Plant secondary metabolites may play a part in modulating the glycemic potential of carbohydrate-rich foods. In particular, phenolics are suggested to reduce starch digestibility by inhibiting digestive enzymes and interacting with starch [20]. Barley muffin has been previously reported to contain the greatest amount of phenolics, followed by corn, oat, wheat and rice muffin. The content of phenolics was observed to inversely relate to the RDS of muffins [3]. Thereby, the content of phenolics could be effective in diminishing the GR of barley and oat muffins.
The carbohydrate sources have a crucial effect on the glycemic potency of muffins. The greater content of fibre, amylose and phenolics may play a part in the reduced glycemic potency of oat and barley muffins. Wheat flour, commonly used for muffin baking, can therefore be substituted with oat and barley flours for healthier muffins. Manipulation of food microstructure, food compositions and food ingredients interaction through food processing technology could be the cornerstone to modulate the glycemic potential of starchy foods.
References
Singh J, Dartois A, Kaur L (2010) Starch digestibility in food matrix: a review. Trends Food Sci Tech 21:168–180
Salmerón J, Manson JE, Stampfer MJ, Colditz GA, Wing AL, Willett WC (1997) Dietary fiber, glycemic load, and risk of non-insulin-dependent diabetes mellitus in women. JAMA 277:472–477
Soong YY, Tan SP, Leong LP, Henry JK (2014) Total antioxidant capacity and starch digestibility of muffins baked with rice, wheat, oat, corn and barley flour. Food Chem 164:462–469
Englyst KN, Englyst HN, Hudson GJ, Cole TJ, Cummings JH (1999) Rapidly available glucose in foods: an in vitro measurement that reflects the glycemic response. Am J Clin Nutr 69:448–454
Henry CJ, Ranawana V (2012) Sugar: a problem of developed countries. Nature 482:471
Ludwig DS (2002) The glycemic index: physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA 287:2414–2423
Baecke JA, Burema J, Frijters JE (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36:936–942
Brouns F, Bjorck I, Frayn KN, Gibbs AL, Lang V, Slama G et al (2005) Glycaemic index methodology. Nutr Res Rev 18:145–171
FAO WHO (1998) Carbohydrates in human nutrition—report of a joint FAO/WHO expert consultation. Food and Agriculture Organisation, Rome
Stork AD, Kemperman H, Erkelens DW, Veneman TF (2005) Comparison of the accuracy of the HemoCue glucose analyzer with the yellow springs instrument glucose oxidase analyzer, particularly in hypoglycemia. Eur J Endocrinol 153:275–281
Wolever TMS (2006) The glycaemic index: a physiological classification of dietary carbohydrate. CABI, Oxfordshire
Monro JA, Mishra S, Venn B (2010) Baselines representing blood glucose clearance improve in vitro prediction of the glycemic impact of customarily consumed food quantities. Br J Nutr 103:295–305
Regand A, Chowdhury Z, Tosh SM, Wolever T, Wood P (2011) The molecular weight, solubility and viscosity of oat beta-glucan affect human glycemic response by modifying starch digestibility. Food Chem 129:297–304
Banchathanaki R, Suphantharika M (2009) Effect of different β-glucans on the gelatinisation and retrogradation of rice starch. Food Chem 114:5–14
Parada J, Aguilera JM (2009) In vitro digestibility and glycemic response of potato starch is related to granule size and degree of gelatinization. J Food Sci 74:E34–E38
Viebke C, Al-Assaf S, Phillips GO (2014) Food hydrocolloids and health claims. Bioact Carbohydr Diet Fibre 4:101–114
Chung SY, Lee SW, Rhee C (2011) Effects of various Maillard reaction products on in vitro starch hydrolysis and blood glucose responses in mice. Starch-Stärke 63:443–449
Langworthy CF, Deuel HJ (1922) Digestibility of raw rice, arrowroot, canna, cassava, taro, tree-fern, and potato starches. J Biol Chem 52:251–261
van de Velde F, van Riel J, Tromp RH (2002) Visualisation of starch granule morphologies using confocal scanning laser microscopy (CSLM). J Sci Food Agric 82:1528–1536
Hargrove JL, Greenspan P, Hartle DK, Dowd C (2011) Inhibition of aromatase and α-amylase by flavonoids and proanthocyanidins from Sorghum bicolor bran extracts. J Med Food 14:799–807
Acknowledgments
Funding for the study was provided by the Singapore Institute for Clinical Sciences, A*Star.
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Soong, Y.Y., Quek, R.Y.C. & Henry, C.J. Glycemic potency of muffins made with wheat, rice, corn, oat and barley flours: a comparative study between in vivo and in vitro. Eur J Nutr 54, 1281–1285 (2015). https://doi.org/10.1007/s00394-014-0806-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-014-0806-9