
Abstract
Background
We compared serum levels of S100A12, a proinflammatory protein predominantly secreted by neutrophils, in children with newly diagnosed childhood-onset systemic lupus erythematosus (cSLE), systemic juvenile arthritis (sJIA), and systemic undefined recurrent fevers (SURFS) to examine its role as a diagnostic and discriminative marker of inflammation and to indirectly point out the importance of neutrophils and innate immunity in the pathogenesis of these diseases.
Materials and methods
In a cross-sectional study, the serum levels of S100A12 protein of 68 children (19 with cSLE, 18 with sJIA, 7 with SURFS, and 24 controls) were determined by enzyme-linked immunosorbent assay and compared between groups and with clinical and laboratory findings.
Results
The median serum S100A12 levels were 469 ng/mL in the cSLE group, 6103 ng/mL in the sJIA group, 480 ng/mL in the SURFS group, and 44 ng/mL in the control group. Children with cSLE, sJIA, and SURFS had significantly higher serum S100A12 levels compared to the control group (p < 0.0001). sJIA patients had the highest levels of S100A12 in comparison to other patients (p < 0.0001), while there was no significant difference between children with cSLE and SURFS.
Conclusion
Elevated serum SA100A12 levels in children with cSLE, sJIA, and SURFS may indicate intense neutrophil activation, which may play an important role in innate immunity in chronic inflammation in these diseases. Serum S100A12 levels could be used as a diagnostic marker of inflammation and be suitable for distinguishing sJIA and other disorders.
Zusammenfassung
Hintergrund
Die Serumspiegel von S100A12, einem hauptsächlich von Neutrophilen sezernierten proinflammatorischen Protein, bei Kindern mit neu diagnostiziertem systemischem Lupus erythematodes (cSLE), systemischer juveniler idiopathischer Arthritis (sJIA) und systemischen undefinierten wiederkehrenden Fieberschüben (SURFS) wurden verglichen. Das Ziel war, die Rolle von S100A12 als diagnostischem und diskriminierendem Entzündungsmarker zu untersuchen und indirekt sowohl auf die Bedeutung von Neutrophilen als auch der angeborenen Immunität bei der Pathogenese dieser Krankheiten hinzuweisen.
Material und Methoden
In einer Querschnittsstudie wurden die Serumspiegel des S100A12-Proteins von 68 Kindern (19 mit cSLE, 18 mit sJIA, 7 mit SURFS und 24 Kontrollen) durch den ELISA-Test („enzyme-linked immunosorbent assay“) bestimmt und zwischen den Gruppen sowie mit klinischen und Laborbefunden verglichen.
Ergebnisse
Die medianen Serumspiegel von S100A12 betrugen 469 ng/ml in der cSLE-Gruppe, 6103 ng/ml in der sJIA-Gruppe, 480 ng/ml in der SURFS-Gruppe und 44 ng/ml in der Kontrollgruppe. Kinder mit cSLE, sJIA und SURFS wiesen jeweils signifikant höhere S100A12-Serumspiegel als die Kontrollgruppe auf (p < 0,0001). sJIA-Patienten hatten die höchsten S100A12-Spiegel im Vergleich zu anderen Patienten (p < 0,0001), während es keinen signifikanten Unterschied zwischen Kindern mit cSLE und SURFS gab.
Schlussfolgerung
Erhöhte S100A12-Serumspiegel bei Kindern mit cSLE, sJIA und SURFS können auf eine intensive Neutrophilenaktivierung hinweisen, die eine wichtige Rolle in der angeborenen Immunität bei chronischen Entzündungen im Rahmen dieser Krankheiten spielen könnte. Die S100A12-Serumspiegel könnten als diagnostischer Entzündungsmarker verwendet werden und zur Unterscheidung von sJIA und anderen Erkrankungen geeignet sein.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The S100 proteins are calcium-binding proinflammatory proteins with a wide spectrum of functions, including inflammation, cell proliferation, differentiation, migration, apoptosis, and metabolic functions [1]. The S100A12 protein, also known as calgranulin C, is a part of the S100 protein family predominantly secreted by neutrophil granulocytes and its extracellular secretion leads to activation of the inflammation cascade, cytokine production, and induction of oxidative stress. It has chemotactic activity and is linked with innate immunity [2, 3]. The S100A12 protein is significantly elevated in systemic juvenile arthritis (sJIA) compared to other autoinflammatory diseases [4]. Previous studies have suggested the use of S100A12 as a useful diagnostic tool in a number of inflammatory disorders [5,6,7,8].
Until recently, disorders of adaptive immunity were thought to play an exclusive and major role in the pathogenesis of childhood-onset systemic lupus erythematosus (SLE). However, novel research suggests that disorders of the immune system in this disease affect both innate and adaptive immunity [9]. Neutrophils are key cells of innate immunity and are involved in the pathogenesis of cSLE and sJIA, but in different ways [9]. Therefore, the two diseases, despite differences in clinical manifestations, share some common pathogenic features.
In this study we compared serum levels of S100A12 protein in children with newly diagnosed cSLE and sJIA, to examine the role of this molecule in innate immunity as a diagnostic and discriminative marker of inflammation and to indirectly point out the importance of neutrophils and innate immunity in the pathogenesis of these diseases. We also included a group of children with recurrent fevers in the absence of infection with high inflammatory markers (systemic undefined recurrent fevers [SURFS]). We chose these diseases for comparison because the inflammatory component is pronounced in all of them, at the beginning of each disease it is not easy to make a diagnosis, and there are recent studies that have described the important role of neutrophils [9], the main source of S100A12 [2], in these diseases.
Patients and methods
Patients
The study was designed as a cross-sectional study in which a total of 68 children were enrolled and divided into three groups: 19 children with newly diagnosed cSLE, 18 children with newly diagnosed sJIA, 7 children with SURFS, and the control group.
All cSLE patients included in this study fulfilled the American College of Rheumatology diagnostic criteria for SLE [10], while sJIA patients fulfilled the International League of Associations for Rheumatology (ILAR) diagnostic criteria [11]. Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) was used to assess disease activity in patients with cSLE [12].
For scoring disease activity in sJIA, we used the Systemic Juvenile Arthritis Disease Activity Score based on the count of any involved joint up to a maximum of ten joints, physician’s global assessment of disease activity, parent global assessment of wellbeing, the modified Systemic Manifestation Score, and erythrocyte sedimentation rate (sJADAS10) or C‑reactive protein (sJADAS10-CRP) [13]. Both sJADAS10 and sJADAS10-CRP scores range from 0 (no activity) to 50 (maximum activity).
Patients with three or more episodes of fever (body temperature ≥38 °C) more than 7 days apart in a period of at least 6 months in the absence of infection, accompanied by high inflammatory markers (either C‑reactive protein >50 mg/L, erythrocyte sedimentation rate >40 mm/h, leukocytes >20 × 109/L, or ferritin >500 μg/L) and without a defined diagnosis were included in the SURFS group. Patients with leukocytopenia were excluded.
The control group included 24 children admitted to hospital for reasons not related to autoimmunity, autoinflammation, or infectious diseases (e.g., tension or psychogenic headaches, functional abdominal pain). Children with leukocytopenia were excluded from the control group.
All the children were patients of the Division of Paediatric Immunology, Rheumatology and Allergology, University Hospital Centre Zagreb, University of Zagreb School of Medicine, Croatia. The study was approved by the Ethics Committee of the University of Zagreb School of Medicine. All procedures performed in the study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Procedures
For all patients, blood samples were collected at the time of diagnosis, prior to initiation of immunosuppressive treatment. All patients with SURFS had fever at the time of blood collection. The blood samples were taken between 9 and 10 am, and collected into vacutainer tubes with clot activator. The tubes were centrifuged at 3500 rpm for 5 min at room temperature and the collected serum was frozen at −80 °C until analysis.
Serum levels of S100A12 were determined with commercially available enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, USA) according to the manufacturer’s protocol. According to the literature, the normal range of S100A12 is 32–385 ng/mL [5].
The following routine laboratory tests were performed: C‑reactive protein, erythrocyte sedimentation rate, hemoglobin, leukocyte count, platelets, ferritin, and α2 globulin. For patients with cSLE, antinuclear antibodies (ANA; positive when ≥1:100 using HEp‑2 indirect immunofluorescence assay), anti-double stranded DNA antibodies (anti-dsDNA; positive when >120 IU/mL using multiplex, fluorescent bead-based immunoassay), and C3 (low when <0.9 g/L) and C4 (low when <0.1 g/L) complement components levels were also analyzed.
Statistical analysis
Numerical variables are descriptively presented with medians and interquartile ranges, while categorical data are presented as absolute and relative frequencies. Differences between the groups of patients and the control group were analyzed by Kruskal–Wallis test followed by a post-hoc test. A p-value <0.05 was considered as statistically significant. Correlations between variables were analyzed with the Spearman’s correlation test.
Results
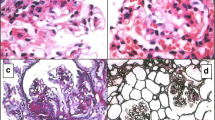
Median time from symptom onset to blood collection was 2 months (range 0–4 months). Baseline features of patients in the cohort are summarized in Table 1. Patients with cSLE were statistically significantly older than other patients and controls. They had lower leukocyte counts in comparison to the patients with sJIA and SURFS. Five cSLE patients presented with renal involvement: four had biopsy-proven lupus nephritis class IV according to the histological classification of the International Society of Nephrology/Renal Pathology Society and one had lupus nephritis class V. Fourteen cSLE patients had arthritis.
Patients with sJIA and SURFS had significantly higher C‑reactive protein levels in comparison to other patients and controls. When comparing inflammatory markers and generally used laboratory markers, including C‑reactive protein, erythrocyte sedimentation rate, hemoglobin, leukocyte count, platelets, ferritin, and α2 globulin, patients with sJIA and SURFS differed only in ferritin concentrations. Fourteen sJIA patients had arthritis at disease presentation, eleven had hepatomegaly, three splenomegaly, while no one had serositis.
The median (range) serum S100A12 levels were 469 (390–653) ng/mL in the cSLE group, 6103 (4087–7969) ng/mL in the sJIA group, 480 (453–763) ng/mL in the SURFS group, and 44 (40–72) ng/mL in the control group (Fig. 1). Serum S100A12 levels were significantly higher in patients with sJIA, cSLE, and SURFS compared to the control group (p < 0.0001). Patients with sJIA had significantly higher serum S100A12 levels compared to the patients with cSLE and SURFS (p < 0.0001). At the same time, there was no statistical difference in S100A12 serum levels between cSLE and SURFS patients (Table 2). S100A12 levels did not differ between patients with cSLE and nephritis and those without nephritis, nor between patients with cSLE and arthritis and those without arthritis. In patients with sJIA there was no difference in the level S100A12 regarding the presence of arthritis (at disease onset), hepatomegaly, or splenomegaly.

Boxplot of serum levels of S100A12 protein in the groups with sJIA, cSLE, SURFS, and CTRL. Serum S100A12 levels are plotted on the ordinate using a logarithmic scale. sJIA systemic juvenile arthritis, cSLE childhood-onset systemic lupus erythematosus, SURFS systemic undefined recurrent fevers, CTRL control group
Among 19 patients with cSLE, 12 had a positive anti-dsDNA at the time of diagnosis. Patients who initially had negative anti-dsDNA during the follow-up period did not develop positive anti-dsDNA. The correlation between anti-dsDNA and S100A12 levels at the time of diagnosis was analyzed. We found a high positive correlation between serum S100A12 and anti-dsDNA levels in patients with cSLE (rs = 0.84, p = 0.002). S100A12 levels in serum furthermore strongly correlate with sJADAS10 (rs = 0.75, p = 0.003) and sJADAS10-CRP score (rs = 0.82, p = 0.0007) in sJIA patients. There was no correlation between S100A12 levels and ANA, C3 and C4 complement components, and SLEDAI-2K in patients with cSLE. Correlation was also absent between S100A12 and erythrocyte sedimentation rate, C‑reactive protein, hemoglobin, leukocyte count, platelets, ferritin, and α2 globulin in patients with cSLE, sJIA, and SURFS.
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the sensitivity and specificity for various cut-off serum S100A12 levels. The cut-off serum S100A12 levels >763 ng/mL distinguished sJIA patients from patients with cSLE and different fever syndromes in the absence of infection with sensitivity of 100% and specificity of 100%.
Discussion
Currently, 25 members of the S100 protein family are known [1]. The most studied members of the S100 protein family are S100A4, S100A8, S100A9, and S100A12, and, among them, S100A8, S100A9, and S100A12 play the main role as mediators of the inflammatory response. S100A4 differs from other members of the S100 family in that it is involved in the pathogenesis of fibrotic diseases [8]. S100A12, on the other hand, stands out for its effect on neutrophils [3]. Namely, it is constitutively expressed in neutrophils and its role in promotion of neutrophil infiltration is significant. This study aimed to compare the serum levels of S100A12 protein in children with cSLE, sJIA, and SURFS as well as their correlation with clinical and laboratory findings at the onset of each disease in order to explore S100A12 as a potential diagnostic marker of inflammation and indirect marker of the role of neutrophils and innate immunity in the pathogenesis of these diseases.
We hypothesized that serum S100A12 protein levels would be elevated in cSLE and sJIA based on previous research on the importance of neutrophils, which secrete it, in the pathogenesis of all three diseases [9]. In children with sJIA, at initial presentation of the illness, it cannot be distinguished from systemic infection or other systemic diseases and different autoinflammatory diseases because of the absence of arthritis [14, 15]. cSLE and sJIA often present with constitutional symptoms [15, 16]. In our cohort of patients, we have shown statistically significant differences in serum S100A12 protein levels between children with sJIA and children with cSLE and other fever syndromes, which may indicate that serum S100A12 could be a discriminatory marker for distinguishing between sJIA and these diseases.
Evidence for neutrophil activation in SLE is contradictory and their exact role in pathogenesis has not yet been elucidated [9]. On the one hand there are studies on decreased neutrophil activity and impaired adhesion and phagocytosis in SLE [17], and on the other, there are studies on increased activity, especially in the vessel wall [18]. In patients with cSLE, neutrophils release neutrophil extracellular traps (NETs) [19, 20]. NETs can stimulate plasmacytoid dendritic cells to produce type I interferon, can cause endothelial cell damage, and serve as an antigen reservoir [21].
Recent data demonstrate use of S100 proteins as potential biomarkers of SLE and lupus nephritis [6,7,8]. In this study we found a positive correlation of serum S100A12 and anti-dsDNA levels in patients with cSLE, but there was no correlation between disease activity (SLEDAI-2K) and serum S100A12 levels. Although increases in anti-dsDNA titers are associated with disease activity, this does not apply to all patients [22]. Since it is known that the increase in anti-dsDNA levels could precede relapse of the disease [23, 24], our finding of a strong association between S100A12 and anti-dsDNA may indicate the use of this S100 protein in predicting relapse in patients with cSLE. We did not observe a difference in serum S100A12 levels between cSLE patients with and without nephritis, which is consistent with other research [7]. Considering the association of serum S100A12 levels in SLE with disease activity, there are conflicting results in the literature. Some studies showed that elevated serum levels of S100A12 were associated with disease activity in SLE patients [6, 8]. Nonetheless, the results of other research similar to ours have not confirmed this association [7]. Instead, it was found that higher urine S100 levels are associated with increased nephritis activity in cSLE [7].
In sJIA, neutrophils are generally activated and neutrophilia can sometimes be so severe that a leukemoid reaction occurs [9]. Neutrophils may be primary effectors and their aberrant activation, including other phagocytes, results in secretion of proinflammatory cytokines and the proteins S100A8, S100A9, and S100A12 [25]. In patients with sJIA, multiple elevated S100A12 values have been reported [4]. We found strong correlation between serum S100A12 and both sJADAS10 and sJADAS10-CRP score in sJIA patients, confirming the utility of S10012 in monitoring disease course [5].
In general, the small number of patients in all groups is a limitation of this study.
Since we detected significantly elevated serum S100A12 levels in children with newly diagnosed sJIA, cSLE, and different fever syndromes, but not in the control group, this may point to intense neutrophil activation, which may play an important role in chronic inflammation in these diseases. Considering that neutrophils are key cells in innate immunity, this finding is an indirect indicator that innate immune disorders are involved in the pathogenesis not only of sJIA, but also of cSLE. Nevertheless, because neutrophils secrete cytokines that can activate the cells of the adaptive immune system, they also form an important link between innate and adaptive immunity. In this way, the paradigm of rheumatic diseases being divided into autoimmune and autoinflammatory changes, and these diseases should be viewed as part of a continuum of disorders of immune regulation, where one or the other pattern overlap to varying degrees. In other words, cSLE can be seen as a disorder of immune regulation in which the autoimmune component is predominantly present, as opposed to sJIA in which the autoinflammatory component is predominantly present.
In summary, this research demonstrated elevated serum levels of S100A12 protein in children with newly diagnosed sJIA, cSLE, and different fever syndromes in the absence of infection with high inflammatory markers, but not in controls. Therefore, this protein may be used as a marker of inflammation in these diseases as well as a discriminative marker and indirect indicator of neutrophil activation and the role of an innate immunity disorder in their pathogenesis.
The contribution of neutrophils to the pathogenesis of rheumatic diseases is still insufficiently understood, but it arouses growing interest and further research is needed to elucidate their involvement with the aim of better diagnosis and development of new therapeutic modalities.
References
Gonzalez LL, Garrie K, Turner MD (2020) Role of S100 proteins in health and disease. Biochim Biophys Acta Mol Cell Res 1867:118677
Pietzsch J, Hoppmann S (2009) Human S100A12: a novel key player in inflammation? J Amino Acids 36:381–389
Li SC, Tsai KW, Huang LH et al (2020) Serum proteins may facilitate the identification of Kawasaki disease and promote in vitro neutrophil infiltration. Sci Rep 10:15645
Foell D, Wittkowski H, Hammerschmidt I et al (2004) Monitoring neutrophil activation in juvenile rheumatoid arthritis by S100A12 serum concentrations. Arthritis Rheum 50:1286–1295
Aljaberi N, Tronconi E, Schulert G et al (2020) The use of S100 proteins testing in juvenile idiopathic arthritis and autoinflammatory diseases in a pediatric clinical setting: a retrospective analysis. Pediatr Rheumatol Online J 18:7
Tydén H, Lood C, Gullstrand B et al (2017) Pro-inflammatory S100 proteins are associated with glomerulonephritis and anti-dsDNA antibodies in systemic lupus erythematosus. Lupus 26:139–149
Turnier JL, Fall N, Thornton S et al (2017) Urine S100 proteins as potential biomarkers of lupus nephritis activity. Arthritis Res Ther 19:242
Šumová B, Cerezo LA, Szczuková L et al (2019) Circulating S100 proteins effectively discriminate SLE patients from healthy controls: a cross-sectional study. Rheumatol Int 39:469–478
Huttenlocher A, Smith JA (2015) Neutrophils in pediatric autoimmune disease. Curr Opin Rheumatol 27:500–504
Hochberg MC (1997) Updating the American college of rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40:1725
Petty RE, Southwood TR, Manners P et al (2004) International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol 31:390–392
Gladman DD, Ibañez D, Urowitz MB (2002) Systemic lupus erythematosus disease activity index 2000. J Rheumatol 29:288–291
Tibaldi J, Pistorio A, Aldera E et al (2020) Development and initial validation of a composite disease activity score for systemic juvenile idiopathic arthritis. Rheumatology (Oxford) 59:3505–3514
Bobek D, Grcevic D, Kovacic N et al (2014) The presence of high mobility group box‑1 and soluble receptor for advanced glycation end-products in juvenile idiopathic arthritis and juvenile systemic lupus erythematosus. Pediatr Rheumatol Online J 12:50
Prakken B, Albani S, Martini A (2011) Juvenile idiopathic arthritis. Lancet 377:2138–2149
Lukic A, Lukic IK, Malcic I et al (2013) Childhood-onset systemic lupus erythematosus in Croatia: demographic, clinical and laboratory features, and factors influencing time to diagnosis. Clin Exp Rheumatol 31:803–812
Fagerholm SC, MacPherson M, James MJ et al (2013) The CD11β integrin (ITGAM) and systemic lupus erythematosus. Lupus 22:657–663
Villanueva E, Yalavarthi S, Berthier CC et al (2011) Netting neutrophils induce endothelial damage, infiltrate tissues, and expose immunostimulatory molecules in systemic lupus erythematosus. J Immunol 187:538–552
Midgley A, Beresford MW (2011) Cellular localization of nuclear antigen during neutrophil apoptosis: mechanism for autoantigen exposure? Lupus 20:641–646
Whittall-García LP, Torres-Ruiz J, Zentella-Dehesa A et al (2019) Neutrophil extracellular traps are a source of extracellular HMGB1 in lupus nephritis: associations with clinical and histopathological features. Lupus 28:1549–1557
Knight JS, Kaplan MJ (2012) Lupus neutrophils: ‘NET’ gain in understanding lupus pathogenesis. Curr Opin Rheumatol 24:441–450
Narayanan K, Marwaha V, Shanmuganandan K et al (2010) Correlation between systemic lupus erythematosus disease activity index, C3, C4 and anti-dsDNA antibodies. Med J Armed Forces India 66:102–107
ter Borg EJ, Horst G, Hummel EJ et al (1990) Measurement of increases in anti-double-stranded DNA antibody levels as a predictor of disease exacerbation in systemic lupus erythematosus. A long-term, prospective study. Arthritis Rheum 33:634–643
Linnik MD, Hu JZ, Heilbrunn KR et al (2005) Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum 52:1129–1137
Lin YT, Wang CT, Gershwin ME et al (2011) The pathogenesis of oligoarticular/polyarticular vs systemic juvenile idiopathic arthritis. Autoimmun Rev 10:482–489
Funding
No specific grant from any public or commercial agency was received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
D. Bobek, M. Sestan, L. Mijacika, N. Kovacic, I.K. Lukic, D. Grcevic, and M. Jelusic declare that they have no competing interests.
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee (Ethics Committee of the University of Zagreb School of Medicine, Zagreb, Croatia) and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Redaktion
Ulf Müller-Ladner, Bad Nauheim
Uwe Lange, Bad Nauheim

Scan QR code & read article online
Rights and permissions
About this article

Cite this article
Bobek, D., Sestan, M., Mijacika, L. et al. Serum S100A12 levels in children with childhood-onset systemic lupus erythematosus, systemic juvenile arthritis, and systemic undefined recurrent fevers. Z Rheumatol 82 (Suppl 1), 74–79 (2023). https://doi.org/10.1007/s00393-021-01142-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00393-021-01142-9