
Abstract
Background
Sleep-disordered breathing (SDB) represents a common and highly relevant co-morbidity in patients with atrial fibrillation (Afib). Obstructive sleep apnea (OSA) has been identified as an independent risk factor for developing Afib and for Afib recurrence after treatment, but the role of central sleep apnea (CSA) is less clear. This study investigated characteristics of SDB in Afib patients with preserved left ventricular ejection fraction (PEF).
Methods and results
Consecutive patients (07/2007 to 03/2016) with documented Afib at hospital admission and PEF undergoing 6-channel cardiorespiratory polygraphy (PG) screening were retrospectively analyzed. A total of 211 patients were included (146 men; age 68.7 ± 8.5 years). Only 6.6% of patients had no SDB (apnea-hypopnea index [AHI] < 5/h). When moderate-to-severe SDB (AHI ≥ 15/h) was classified based on the predominant type of apneas and hypopneas, OSA (≥ 80% obstructive events) was found in 15% of patients, CSA (≥ 80% central events) in 10%, and 36% had mixed sleep apnea. For patients with Cheyne–Stokes respiration (CSR; 34%), time spent in CSR increased significantly as total AHI increased (p < 0.001); total CSR duration was 20, 50, and 117 min, respectively, in patients with mild, moderate, and severe SDB.
Conclusions
SDB was highly prevalent in this cohort of patients with Afib and PEF. The proportion of patients with moderate-to-severe OSA, for whom treatment is recommended by current guidelines, was about 15%. With 36% of patients presenting with moderate-to-severe mixed sleep apnea and almost 10% of patients having CSA, treatment guidelines for these types of SDB in the setting of Afib are needed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Atrial fibrillation (Afib) is one of the most common cardiac arrhythmias, affecting approximately 1% of the general population and up to 10% of those aged 80 years and older. The aging population demographic means that the number of patients with Afib is estimated to increase 2.5-fold by 2050 [1], with an associated significant rise in costs to the healthcare system [2].
There are a number of recognized independent risk factors for development of Afib, including increasing age, arterial hypertension, heart failure, coronary disease, and obstructive sleep apnea (OSA) [3,4,5,6]. OSA is the most common type of sleep-disordered breathing (SDB) [7, 8] and is characterized by partial (hypopnea) or complete (apnea) collapse of the upper airways resulting in negative intrathoracic pressure swings, oxygen desaturation, and hypoxemia, as well as initial vagal stimulation followed by activation of the sympathetic nervous system [9].
OSA has both short- and long-term effects on Afib. Even short-term episodes of negative intrathoracic pressure can trigger Afib in animal models [10], probably mediated by sympathico-vagal-imbalance [11]. In an in vitro model, hypoxia increased atrial vulnerability to re-entrant arrhythmias via alteration of conduction properties [12]. The long-term effects of OSA include sympathetic activation, oxidative stress, and systemic inflammation, along with comorbidities resulting in structural and electrical remodeling of the atria, and the left atrium in particular. Thus, OSA might create an arrhythmogenic substrate and be a trigger for Afib onset at the same time [13, 14]. OSA has been shown to be an independent predictor of Afib development and of arrhythmia recurrence after antiarrhythmic treatment or intervention [15,16,17,18,19,20]. Therefore, recent European and US guidelines recommend screening for OSA and implementation of effective treatment in patients with Afib [21, 22].
Central sleep apnea (CSA), another form of SDB, is characterized by interruption or reduction of ventilatory effort combined with oxygen desaturation and is thought to promote Afib independently of congestive heart failure (CHF) [23]. There is a lack of data on pathogenetic mechanisms of CSA in Afib [24, 25], although CSA has been shown to be associated with incident Afib [26] and successful cardioversion of Afib can moderately decrease central SDB events and the corresponding apnea-hypopnea index (AHI) [27]. Cheyne–Stokes respiration (CSR) is a subtype of CSA and is characterized by a crescendo-decrescendo alteration of breathing amplitude. CSR has been established as an indicator of worse outcome in heart failure (HF) patients [28].
While continuous positive airway pressure (CPAP) is recommended for the first-line treatment of OSA and has been shown to reduce Afib recurrence after antiarrhythmic therapy [29,30,31], adaptive servo-ventilation (ASV) is a more appropriate treatment for patients with CSA and preserved left ventricular ejection fraction (PEF) [32]. However, just as more information is needed on the pathophysiological links between CSA and Afib, definitive therapeutic recommendations for the treatment of CSA/CSR in Afib cannot be made based on available data [21].
This explorative study investigated different phenotypes of SDB, and their prevalence and characteristics, in patients with Afib. The aim was to provide more detailed characterization of apneas and hypopneas in a large group of patients to offer qualified treatment decisions. To reduce bias, patients with impaired left ventricular ejection fraction (LVEF) and those who had undergone specific antiarrhythmic treatment were excluded.
Methods
Patients
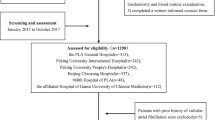
This study included all patients with documented Afib on admission (12-channel ECG on admission) and preserved left ventricular ejection fraction [PEF; ejection fraction ≥ 55% on standardized echocardiography (modified Simpson method)] who underwent routine 6-channel cardiorespiratory polygraphy (PG) screening for SDB between July 2007 to March 2016. Of 22,135 entries in our database 1,220 met these criteria. Exclusion criteria included hemodynamically relevant valvular diseases (> grade 2), valvular reconstruction or replacement surgery, any kind of implanted pacemaker or defibrillator apart from event recorders, previous cardiac surgery or interventional arrhythmic therapy, acute decompensation of heart failure, chronic obstructive pulmonary disease (GOLD > 2) or other structural lung diseases (oxygen saturation < 90% at rest), pregnancy, and age < 18 years. After analysis for exclusion criteria, 211 patients meeting all inclusion criteria and presenting none of the exclusion criteria were included.
All patients gave informed consent and the study was approved by the local institutional review board.
Cardiorespiratory polygraphy
SDB was evaluated using high-quality 6-channel PG as described previously [33]. A minimum of 240 min of artifact-free recording time was chosen based on guidelines from several European countries stating that a minimal length of 4 h is sufficient [34].
Respiratory events were classified by a single investigator using the American Academy of Sleep Medicine (AASM) 2012 criteria [35]. Events were classified as apnea if there was a drop in peak nasal airflow by ≥ 90% of pre-event baseline lasting for ≥ 10 s. Apnea was scored as obstructive if apnea criteria were met in association with continuation of, or increase in, inspiratory effort during the event. Central apnea was defined as apnea according to the above definition in the absence of associated inspiratory effort, and mixed apnea was characterized by absence of inspiratory effort during the first part of the event and recommencement in the later part of the event. Events were classified as hypopnea if there was a drop in peak nasal airflow by ≥ 30% of pre-event baseline lasting for ≥ 10 s in combination with an oxygen desaturation of ≥ 3% from pre-event baseline (ODI3%). Hypopneas were classified as obstructive if there was either snoring at the time of the event or an increase of inspiratory flattening of nasal airflow, or occurrence of associated thoracoabdominal paradox during, but not before, the event; central hypopnea was scored if none of the obstructive hypopnea criteria were met [35].
SDB was defined as an AHI of ≥ 5/h. SDB severity was classified as mild (AHI 5–14/h), moderate (AHI 15–29/h), or severe (AHI ≥ 30/h) [36]. Current guidelines recommend treatment when AHI is ≥ 15/h [30]. Therefore, patients with an AHI of < 15/h were classified as having none–mild SDB (nmSDB) for this analysis.
Cheyne–Stokes respiration (CSR) was defined as ≥ 3 successive episodes of central apneas and/or hypopneas connected by a crescendo–decrescendo variation in breathing amplitude with a cycle length (CL) of ≥ 40 s [35]. In addition, the breathing pattern had to occur in five central apneas and/or hypopneas per hour in 2 or more hours of recorded time. CSR CL was calculated as the period between commencement of a central hypopnea or apnea to termination of ventilation, and circulatory delay (CD) was assessed as the period between completion of central apnea or hypopnea to nadir of oxygen saturation [37].
Moderate-to-severe SDB (AHI ≥ 15/h) was classified according to the predominant type of apneas (> 80% central events as CSA; > 80% obstructive events as OSA) or as mixed sleep apnea (20–80% of events central or obstructive respectively). This definition was also used in a previous study [20], but it is more restrictive than some current guidelines referring to the association between OSA and Afib [20].
PG recordings were analyzed using RemLogic-E version 3.2. by Embla systems (Broomfield, CO, USA) or DOMINO version 2.6.0 by Somnomedics (Randersacker, Germany).
Statistical analysis
Patient demographic and clinical characteristics and sleep parameters were described by apnea type and severity (four groups) using mean and standard deviation values or frequencies and proportions. Hypotheses of no difference between the four groups for continuous variables were tested using ANOVA and pairwise tests were performed using t tests. Discrete variables were analyzed using a z test. Linear regression and Spearman Rank Order correlation were performed for comparison of time spent in Cheyne–Stokes Respiration (tCSR) and the AHI.
Adjusted comparisons of AHI (also dichotomized as < 15 vs ≥ 15/h), time spent with oxygen saturation (SpO2) below 90% (T < 90%), oxygen desaturation index (ODI3%), and obstructive AHI (oAHI) based on the type of Afib were performed using a linear regression model or logistic regression model; comparisons were adjusted for age, sex, body mass index, left atrial diameter (LAD) and history of arterial hypertension (aHTN).
All statistical analyses were explorative and there was no correction for multiple testing. Testing was performed using Stata 14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP) and SigmaPlot 12.0 by Systat Software Inc.
Results
After elimination of duplicate entries, PG recordings with < 6 channels, and insufficient recording time, a total of 211 patients previously untreated for SDB met all the inclusion criteria, and none of the exclusion criteria, and were included in this analysis.
The majority presented with persistent Afib. Demographic and clinical data at baseline for the total study population and by type of SDB are shown in Table 1.
None-to-mild SDB (nmSDB; AHI < 15/h) was documented in 85 patients (40.3%), 31 patients (14.7%) had predominant OSA, 20 (9.5%) had predominant CSA, and 75 (35.5%) had mixed sleep apnea (SA). CSR was documented in 71 patients (33.6%), 5 of whom had predominant OSA, 18 had predominant CSA, 44 had mixed SA, and 4 had nmSDB (Fig. 1).

Proportion of atrial fibrillation patients with different types of sleep-disordered breathing. nmSDB, none–mild sleep disordered breathing with apnea–hypopnea index < 15/h; CSA central sleep apnea, CSR Cheyne–Stokes respiration, MSA mixed sleep apnea, OSA obstructive sleep apnea
Patients with moderate-to-severe central, obstructive, or mixed SA had a significantly higher body mass index than patients in the nmSDB group. Compared to Afib patients without SDB, those with mixed SA were more likely to be male, and those with CSA were more likely to be male and were younger. Other baseline demographics and clinical characteristics were similar between patient groups.
Overall, nearly 60% of the total AHI was made up of hypopneas. Detailed baseline respiratory parameters for the total study population and by type of SDB are presented in Table 2. As expected, SDB metrics indicated greater SDB severity in patients with moderate-to-severe SDB compared with none or mild SDB. Also consistent with the definition of patient groups, patients with predominant OSA or mixed SA had significantly lower minimum oxygen saturation than other patient groups, and those with predominant OSA had more obstructive apneas and hypopneas compared with the predominant CSA and mixed SA groups. Patients with mixed SA spent significantly more time in CSR than those with OSA. The central apnea index (cAI) was higher in the CSA vs OSA and mixed SA groups, and patients with predominant CSA spent more time in CSR than other patient groups. In addition, CSA patients tended to spend more time with oxygen saturation at < 90% (T90) and had longer CSR CL and CD. For all patients with CSR, time spent in CSR increased significantly as the AHI increased (ρ < 0.01) (Fig. 2).

Relationship between the apnea–hypopnea index (AHI) and time spent in Cheyne–Stokes respiration (CSR) in patients with moderate–severe sleep-disordered breathing
The SDB phenotype tended to vary by the type of Afib (Fig. 3). Patients with paroxysmal Afib seemed to be more likely to have nmSDB, whereas the rate of nmSDB appeared to be lower in those with long-persistent-to-permanent Afib and these patients apparently had the highest rates of moderate-to-severe SDB and CSR. There were no significant differences between patients with different types of Afib with respect to AHI, ODI3%, T90, and CSR metrics (Table 3). The results of an explorative multivariate analysis adjusting for potential confounding factors including age, sex, history of hypertension, and BMI were similar, although no statistically significant associations were found.

Type of sleep-disordered breathing (SDB) in patients with different types of atrial fibrillation
Discussion
The results of this explorative study provide new information about the prevalence and characteristics of SDB in patients with Afib. In addition to identifying a high prevalence of moderate-to-severe SDB (60%), we showed that mixed SA was the most common manifestation of SDB in Afib followed by OSA, while CSA was less common. We also found that hypopneas accounted for the majority of respiratory events, and that time spent in CSR increased in parallel with both increasing SDB severity and persistence of Afib.
A previous study in patients with Afib and PEF documented moderate-to-severe CSA and OSA using PG in 49.4% of patients (half each with OSA and CSA) [38]. This study only used apneas, not hypopneas, to differentiate between central and obstructive events, whereas we also looked at hypopneas. In addition, the previous study defined predominant OSA and CSA as > 50% obstructive and central events, respectively, rather than the more strict ≥ 80% definition used in our study. These factors could explain the higher CSA rate compared with the current study. However, our overall prevalence of moderate-to-severe SDB was higher (approximately 60 vs 50%), which may be due to the higher BMI and more advanced age of our cohort. In another study of Afib patients, most of whom had HF with PEF, 50% of patients had an AHI of ≥ 15/h and predominant CSA (≥ 50% central events central or CSR pattern with AHI ≥ 5/h) was seen in 15% [39]. However, the ability to directly compare these results to our study is limited because of the use of different SDB classification criteria and also because oxygen desaturation was defined as > 4% (compared with > 3% as recommended by the current guidelines [35] and done in our study). Reported prevalence rates for OSA in Afib have varied between studies, from 32% (OSA defined as apnea index [AI] ≥ 5/h plus AHI ≥ 15/h) [40] to 80% (OSA defined as AHI ≥ 10/h) [7]. Again, the differences between studies are most likely explained by the different OSA definitions used and differences in patient characteristics between studied populations (e.g., age and BMI).
We found a tendency towards higher proportions of SDB as the duration of Afib increased (approximately 50 vs 60 vs 70% in paroxysmal vs persistent vs long persistent to permanent Afib, respectively). This is consistent with reports showing that SDB is an independent predictor of Afib occurrence [41]. Nocturnal hypoxemia, a consequence of SDB, has been shown to be a risk factor for developing Afib and appears to be one factor responsible for cardiac structural remodeling [11]. The hypoxemic burden (T90) was increased in all patients with SDB in our study. This parameter appears to be a robust and objective predictor of overall mortality in HF with reduced ejection fraction (HF-REF) [42], and this may also be the case in patients with HF-PEF. On average, in our study, patients with SDB spent nearly an hour with oxygen saturation at < 90%, regardless of the type of SDB, suggesting that treatment to reduce hypoxemia would be beneficial across all SDB phenotypes.
Although less marked than the relationship between increasing SDB and persistence of AF, we also showed that the proportion of CSR tended to increase with increasing AF persistence. This is consistent with data showing that both CSA and CSR are associated with a higher incidence of Afib [43]. Conversely, Afib itself has been reported to be a risk factor for CSA/CSR incidence in HF-REF patients [44]. If this also applies in patients with PEF, it will be interesting to further assess the cause-and-effect relationship between increased time in CSR and the duration of Afib. In our study, patients with CSA and CSR showed more severe SDB (higher proportion of CSR, longer time in CSR, and longer CL and CD). CSR has been identified as a predictor of mortality in CHF patients [45] and CSR severity appears to correlate with cardiac impairment [33]. In patients with HF-REF, the phenotype and morphology of CSR is reasonably well understood, and both CL and CD have been established as indicators of cardiac function [37]. To our knowledge, no such research has been conducted in patients with Afib and PEF. Our data on CL and CD in patients with CSR are consistent with those of Wedewardt and colleagues (mean CL 54.7 vs 49.1 s, mean CD 33.4 vs 29.0 s). The slight variations might be a result of the higher number of patients in our study (n = 72 vs 21). We found that patients with long-persistent-to-permanent Afib tended to have the longest CL; therefore, it might be worth investigating whether CL correlates with duration of arrhythmias, as well as with cardiac function, in a larger patient group.
As described above, OSA and CSA have different pathophysiological mechanisms and etiology. In addition, definitions of OSA vary widely between the previous studies and guidelines. The majority of studies did not differentiate between OSA and CSA [5, 15,16,17, 40, 44, 46,47,48,49,50,51,52,53] or just used questionnaires for the diagnosis of SDB [18, 54,55,56]. Only two studies took hypopnea type into account; these defined OSA as > 5 obstructive hypopneas and apneas per hour [4] or when > 80% of apneas were obstructive [20]. In contrast, our study used recommended methods [35, 57] to clearly differentiate between obstructive and central respiratory events, including hypopneas. We chose to classify patients as having predominant OSA or CSA when > 80% of hypopneas and apneas were obstructive or central, respectively, to provide clear discrimination between the two forms of SDB. We also noted a high proportion of patients with mixed SA, who had both obstructive and central events.
Even though we used a strict classification for OSA and CSA, the prevalence of these conditions in Afib patients was quite high, suggesting an indication for therapy. Afib guidelines recommend CPAP treatment for patients with OSA. For CSA, AASM guidelines favor therapy with ASV in patients with PEF [32], because this provides more effective suppression of CSA and improves sleep quality to a greater extent than first-line therapy with CPAP [58]. The results of the Cardiovascular Outcomes With Minute Ventilation-Targeted Adaptive Servo-Ventilation Therapy in Heart Failure (CAT-HF) study recently indicated that treatment of SDB in post-acute HF-PEF patients might be associated with improved outcome [59]. Moreover, the CAT-HF arrhythmia substudy showed a 16% reduction in Afib burden in ASV-treated patients compared with a 24% increase in the control group who did not receive SDB-specific intervention [60].
While correct differentiation between OSA and CSA is important to identify the most appropriate primary treatment strategy to optimize therapy for every patient, there was a high prevalence of mixed SA in our study and there are currently no clear recommendations on therapy for these patients. In our sample, Afib patients with mixed SA had a high proportion of periodic breathing meeting CSR criteria, which is usually categorized as CSA, meaning that ASV might be the most appropriate treatment option.
Limitations
A larger patient population, the inclusion of hypopneas in SDB classification, and the use of strict criteria to define predominant OSA and CSA are all strengths of our study. However, there are also a number of limitations that need to be taken into account. The analysis was conducted retrospectively and exploratively using data from a tertiary center, and therefore, the patient population included might not be representative of those found in primary centers. Although use of PG is routine clinical practice for patients with heart diseases in our clinic, it is possible that some Afib patients did not undergo SDB screening. Finally, nocturnal respiratory parameters may have been underestimated by the use of PG, because calculations are based on total recording time rather than total sleep time (which is usually less than recording time).
Conclusions
Our analysis showed that SDB was highly prevalent in patients with Afib and PEF. Even using the most restrictive definitions for predominant OSA and CSA, a significant number of patients had SDB requiring treatment. Taken together, our findings contribute to better understanding of SDB in Afib and could help guide appropriate treatment strategies for different types of SDB and patient phenotypes.
References
Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE (2001) Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and risk factors in atrial fibrillation (ATRIA) study. JAMA 285:2370–2375
Reinhold T, Lindig C, Willich SN, Bruggenjurgen B (2011) The costs of atrial fibrillation in patients with cardiovascular comorbidities—a longitudinal analysis of German health insurance data. Europace 13:1275–1280
Benjamin EJ, Levy D, Vaziri SM, D’Agostino RB, Belanger AJ, Wolf PA (1994) Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study JAMA 271:840–844
Gami AS, Hodge DO, Herges RM, Olson EJ, Nykodym J, Kara T, Somers VK (2007) Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol 49:565–571
Leung RS, Huber MA, Rogge T, Maimon N, Chiu KL, Bradley TD (2005) Association between atrial fibrillation and central sleep apnea. Sleep 28:1543–1546
Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, O’Connor GT, Boland LL, Schwartz JE, Samet JM (2001) Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med 163:19–25
Braga B, Poyares D, Cintra F, Guilleminault C, Cirenza C, Horbach S, Macedo D, Silva R, Tufik S, De Paola AA (2009) Sleep-disordered breathing and chronic atrial fibrillation. Sleep Med 10:212–216
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S (1993) The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 328:1230–1235
Somers VK, Dyken ME, Clary MP, Abboud FM (1995) Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest 96:1897–1904
Linz D, Hohl M, Ukena C, Mahfoud F, Wirth K, Neuberger HR, Bohm M (2015) Obstructive respiratory events and premature atrial contractions after cardioversion. Eur Respir J 45:1332–1340
Linz D, Schotten U, Neuberger HR, Bohm M, Wirth K (2011) Negative tracheal pressure during obstructive respiratory events promotes atrial fibrillation by vagal activation. Heart Rhythm 8:1436–1443
Lammers WJ, Kirchhof C, Bonke FI, Allessie MA (1992) Vulnerability of rabbit atrium to reentry by hypoxia. Role of inhomogeneity in conduction and wavelength. Am J Physiol 262:H47-55
Linz D, Linz B, Hohl M, Bohm M (2016) Atrial arrhythmogenesis in obstructive sleep apnea: Therapeutic implications. Sleep Med Rev 26:87–94
Linz D, Denner A, Illing S, Hohl M, Ukena C, Mahfoud F, Ewen S, Reil JC, Wirth K, Bohm M (2016) Impact of obstructive and central apneas on ventricular repolarisation: lessons learned from studies in man and pigs. Clin Res Cardiol 105:639–647
Bitter T, Nolker G, Vogt J, Prinz C, Horstkotte D, Oldenburg O (2012) Predictors of recurrence in patients undergoing cryoballoon ablation for treatment of atrial fibrillation: the independent role of sleep-disordered breathing. J Cardiovasc Electrophysiol 23:18–25
Jongnarangsin K, Chugh A, Good E, Mukerji S, Dey S, Crawford T, Sarrazin JF, Kuhne M, Chalfoun N, Wells D, Boonyapisit W, Pelosi F Jr, Bogun F, Morady F, Oral H (2008) Body mass index, obstructive sleep apnea, and outcomes of catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 19:668–672
Kanagala R, Murali NS, Friedman PA, Ammash NM, Gersh BJ, Ballman KV, Shamsuzzaman AS, Somers VK (2003) Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 107:2589–2594
Matiello M, Nadal M, Tamborero D, Berruezo A, Montserrat J, Embid C, Rios J, Villacastin J, Brugada J, Mont L (2010) Low efficacy of atrial fibrillation ablation in severe obstructive sleep apnoea patients. Europace 12:1084–1089
Naruse Y, Tada H, Satoh M, Yanagihara M, Tsuneoka H, Hirata Y, Ito Y, Kuroki K, Machino T, Yamasaki H, Igarashi M, Sekiguchi Y, Sato A, Aonuma K (2013) Concomitant obstructive sleep apnea increases the recurrence of atrial fibrillation following radiofrequency catheter ablation of atrial fibrillation: clinical impact of continuous positive airway pressure therapy. Heart Rhythm 10:331–337
Patel D, Mohanty P, Di Biase L, Shaheen M, Lewis WR, Quan K, Cummings JE, Wang P, Al-Ahmad A, Venkatraman P, Nashawati E, Lakkireddy D, Schweikert R, Horton R, Sanchez J, Gallinghouse J, Hao S, Beheiry S, Cardinal DS, Zagrodzky J, Canby R, Bailey S, Burkhardt JD, Natale A (2010) Safety and efficacy of pulmonary vein antral isolation in patients with obstructive sleep apnea: the impact of continuous positive airway pressure. Circ Arrhythm Electrophysiol 3:445–451
Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K (2016) 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 37:2893–2962
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ Jr, Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D, Heart Rhythm Society Task Force on C, Surgical Ablation of Atrial F (2012) 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm 9:632–696 e621
Levy P, Pepin JL, Arnaud C, Tamisier R, Borel JC, Dematteis M, Godin-Ribuot D, Ribuot C (2008) Intermittent hypoxia and sleep-disordered breathing: current concepts and perspectives. Eur Respir J 32:1082–1095
Lavergne F, Morin L, Armitstead J, Benjafield A, Richards G, Woehrle H (2015) Atrial fibrillation and sleep-disordered breathing. J Thorac Dis 7:E575-584
Linz D, Woehrle H, Bitter T, Fox H, Cowie MR, Bohm M, Oldenburg O (2015) The importance of sleep-disordered breathing in cardiovascular disease. Clin Res Cardiol 104:705–718
Tung P, Levitzky YS, Wang R, Weng J, Quan SF, Gottlieb DJ, Rueschman M, Punjabi NM, Mehra R, Bertisch S, Benjamin EJ, Redline S (2017) Obstructive and central sleep apnea and the risk of incident atrial fibrillation in a community cohort of men and women. J Am Heart Assoc 6
Fox H, Bitter T, Horstkotte D, Oldenburg O (2016) Cardioversion of atrial fibrillation or atrial flutter into sinus rhythm reduces nocturnal central respiratory events and unmasks obstructive sleep apnoea. Clin Res Cardiol 105:451–459
Lanfranchi PA, Braghiroli A, Bosimini E, Mazzuero G, Colombo R, Donner CF, Giannuzzi P (1999) Prognostic value of nocturnal Cheyne–Stokes respiration in chronic heart failure. Circulation 99:1435–1440
Fein AS, Shvilkin A, Shah D, Haffajee CI, Das S, Kumar K, Kramer DB, Zimetbaum PJ, Buxton AE, Josephson ME, Anter E (2013) Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol 62:300–305
Epstein LJ, Kristo D, Strollo PJ Jr, Friedman N, Malhotra A, Patil SP, Ramar K, Rogers R, Schwab RJ, Weaver EM, Weinstein MD (2009) Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 5:263–276
Oldenburg O, Arzt M, Bitter T, Bonnemeier H, Edelmann F, Fietze I, Podszus T, Schafer T, Schobel C, Skobel E, Skowasch D, Penzel T, Nienaber C (2015) Positionspapier “Schlafmedizin in der Kardiologie”. Der Kardiologe 9:140–158
Aurora RN, Bista SR, Casey KR, Chowdhuri S, Kristo DA, Mallea JM, Ramar K, Rowley JA, Zak RS, Heald JL (2016) Updated adaptive servo-ventilation recommendations for the 2012 AASM Guideline: the treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses. J Clin Sleep Med 12:757–761
Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Topfer V (2007) Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 9:251–257
Arnardottir ES, Verbraecken J, Goncalves M, Gjerstad MD, Grote L, Puertas FJ, Mihaicuta S, McNicholas WT, Parrino L, The National Representatives as Study C (2016) Variability in recording and scoring of respiratory events during sleep in Europe: a need for uniform standards. J Sleep Res 25:144–157
Berry RB, Budhiraja R, Gottlieb DJ, Gozal D, Iber C, Kapur VK, Marcus CL, Mehra R, Parthasarathy S, Quan SF, Redline S, Strohl KP, Davidson Ward SL, Tangredi MM (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 8:597–619
Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. (1999). Sleep 22:667–689
Wedewardt J, Bitter T, Prinz C, Faber L, Horstkotte D, Oldenburg O (2010) Cheyne–Stokes respiration in heart failure: cycle length is dependent on left ventricular ejection fraction. Sleep Med 11:137–142
Bitter T, Langer C, Vogt J, Lange M, Horstkotte D, Oldenburg O (2009) Sleep-disordered breathing in patients with atrial fibrillation and normal systolic left ventricular function. Dtsch Arztebl Int 106:164–170
Albuquerque FN, Calvin AD, Sert Kuniyoshi FH, Konecny T, Lopez-Jimenez F, Pressman GS, Kara T, Friedman P, Ammash N, Somers VK, Caples SM (2012) Sleep-disordered breathing and excessive daytime sleepiness in patients with atrial fibrillation. Chest 141:967–973
Porthan KM, Melin JH, Kupila JT, Venho KK, Partinen MM (2004) Prevalence of sleep apnea syndrome in lone atrial fibrillation: a case-control study. Chest 125:879–885
Chao TF, Liu CJ, Chen SJ, Wang KL, Lin YJ, Chang SL, Lo LW, Hu YF, Tuan TC, Chen TJ, Chiou CW, Chen SA (2014) Incidence and risk of atrial fibrillation in sleep-disordered breathing without coexistent systemic disease. Circ J 78:2182–2187
Oldenburg O, Wellmann B, Buchholz A, Bitter T, Fox H, Thiem U, Horstkotte D, Wegscheider K (2016) Nocturnal hypoxaemia is associated with increased mortality in stable heart failure patients. Eur Heart J 37:1695–1703
May AM, Blackwell T, Stone PH, Stone KL, Cawthon PM, Sauer WH, Varosy PD, Redline S, Mehra R (2016) Central sleep-disordered breathing predicts incident atrial fibrillation in older men. Am J Respir Crit Care Med 193:783–791
Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD (1999) Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med 160:1101–1106
Javaheri S, Shukla R, Zeigler H, Wexler L (2007) Central sleep apnea, right ventricular dysfunction, and low diastolic blood pressure are predictors of mortality in systolic heart failure. J Am Coll Cardiol 49:2028–2034
Digby GC, Baranchuk A (2012) Sleep apnea and atrial fibrillation; 2012 update. Curr Cardiol Rev 8:265–272
Flemons WW, Remmers JE, Gillis AM (1993) Sleep apnea and cardiac arrhythmias. Is there a relationship? Am Rev Respir Dis 148:618–621
Guilleminault C, Connolly SJ, Winkle RA (1983) Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome. Am J Cardiol 52:490–494
Hoffstein V, Mateika S (1994) Cardiac arrhythmias, snoring, and sleep apnea. Chest 106:466–471
Mehra R, Benjamin EJ, Shahar E, Gottlieb DJ, Nawabit R, Kirchner HL, Sahadevan J, Redline S, Sleep Heart Health S (2006) Association of nocturnal arrhythmias with sleep-disordered breathing: the sleep heart health study. Am J Respir Crit Care Med 173:910–916
Mooe T, Gullsby S, Rabben T, Eriksson P (1996) Sleep-disordered breathing: a novel predictor of atrial fibrillation after coronary artery bypass surgery. Coron Artery Dis 7:475–478
Tanigawa T, Yamagishi K, Sakurai S, Muraki I, Noda H, Shimamoto T, Iso H (2006) Arterial oxygen desaturation during sleep and atrial fibrillation. Heart 92:1854–1855
Vizzardi E, Sciatti E, Bonadei I, D’Aloia A, Curnis A, Metra M (2014) Obstructive sleep apnoea-hypopnoea and arrhythmias: new updates. J Cardiovasc Med (Hagerstown)
Chilukuri K, Dalal D, Marine JE, Scherr D, Henrikson CA, Cheng A, Nazarian S, Spragg D, Berger R, Calkins H (2009) Predictive value of obstructive sleep apnoea assessed by the Berlin Questionnaire for outcomes after the catheter ablation of atrial fibrillation. Europace 11:896–901
Gami AS, Pressman G, Caples SM, Kanagala R, Gard JJ, Davison DE, Malouf JF, Ammash NM, Friedman PA, Somers VK (2004) Association of atrial fibrillation and obstructive sleep apnea. Circulation 110:364–367
Chilukuri K, Dalal D, Gadrey S, Marine JE, Macpherson E, Henrikson CA, Cheng A, Nazarian S, Sinha S, Spragg D, Berger R, Calkins H (2010) A prospective study evaluating the role of obesity and obstructive sleep apnea for outcomes after catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 21:521–525
Randerath WJ, Hein H, Arzt M, Galetke W, Nilius G, Penzel T, Rasche K, Ruhle KH, Mayer G (2014) Consensus paper on the diagnosis and treatment of sleep disordered breathing. Pneumologie 68:106–123
Teschler H, Dohring J, Wang YM, Berthon-Jones M (2001) Adaptive pressure support servo-ventilation: a novel treatment for Cheyne–Stokes respiration in heart failure. Am J Respir Crit Care Med 164:614–619
O’Connor CM, Whellan DJ, Fiuzat M, Punjabi NM, Tasissa G, Anstrom KJ, Benjafield AV, Woehrle H, Blase AB, Lindenfeld J, Oldenburg O (2017) Cardiovascular outcomes with minute ventilation-targeted adaptive servo-ventilation therapy in heart failure: the CAT-HF trial. J Am Coll Cardiol 69:1577–1587
Piccini JP et al (2016) Adaptive servo-ventlation reduces atrial fibrillation burden in patients with heart failure and sleep apnea: results from the CAT-HF arrhythmia substudy. Late-Breaking Clinical Trial Update. Presented at: Heart Failure Society of America Scientific Assembly; Sept. 17–20, 2016; Orlando, FL, USA
Acknowledgements
English language editing assistance was provided by Nicola Ryan, an independent medical writer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Olaf Oldenburg received honoraria for lectures and travel grants from ResMed, Somnomedics, Novartis, Boehringer Ingelheim, and Bayer. The other authors have no conflicts of interest to declare.
Rights and permissions
About this article

Cite this article
Strotmann, J., Fox, H., Bitter, T. et al. Characteristics of sleep-disordered breathing in patients with atrial fibrillation and preserved left ventricular ejection fraction. Clin Res Cardiol 107, 120–129 (2018). https://doi.org/10.1007/s00392-017-1163-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-017-1163-5