
Abstract
Purpose
The United States Preventive Services Task Force (USPSTF) newly drafted recommendations for colorectal cancer (CRC) screening age in average-risk individuals decreased to 45 years from 50 years. This study evaluates the change in the incidence of CRC, compares the demographic characteristics, characteristics of CRC, survival, and factors affecting the survival of younger (< 50 years) with the older (> 50 years) CRC-diagnosed population of Boston Medical Center (BMC). Also tailors the screening recommendations of CRC based on subpopulations.
Methods
A retrospective cohort study was conducted from 2004 to 2019 at BMC who underwent colonoscopy, to see newly diagnosed CRC. The analysis was done in R studio version 1.2.5033.
Results
The incidence rate of CRC is increasing in the younger population. The CRC in younger population was 350 and older was 2019. The most prevalent site among the younger population was rectum (33.33%), and most of the CRC were diagnosed at an advanced stage. Hispanics were less likely to be diagnosed with CRC in older age group (OR= 0.468, 95% CI 0.285, 0.796). Lower BMI was associated with a higher risk of mortality (p= 0.012). There was no difference in survival in younger and older populations.
Conclusions
CRC is increasing in the younger population, and Hispanics are diagnosed with CRC usually at a younger age. Early screening in young populations with average risk and even earlier screening in high-risk populations like Hispanics is warranted for timely recognition for prevention, early management, and reduction of mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, CRC is the third most common cancer and second most common cancer-causing death [1]. The lifetime risk of developing colorectal cancer according to the American Cancer Society is about 1 in 23 (4.4%) for men and 1 in 25 (4.1%) for women [2]. The incidence of CRC varies across and within countries [3]. In the USA, the incidence of CRC differs among states, resulting in the threefold higher incidence in Alaska compared to the Southwest. Many factors like access to screening and other daily lifestyle and behaviors might have contributed to these differences [4].
CRC has now been increasing in younger populations (age < 50 years) in the USA [5]. Many studies done globally have shown a similar trend [6]. Despite being one of the curable cancers, the mortality rate of CRC is increasing in this subgroup of the population [7]. Obesity, sedentary lifestyle, alcohol, smoking have been hypothesized to be the common modifiable risk factors for the development of colon cancer in these younger populations [8]. CRC usually begins with noncancerous proliferation of mucosal epithelial cells, grows as a polyp, and gradually becomes a cancerous growth [9]. Because of the lack of screening in these younger populations, it is difficult to diagnose CRC in its very early stage when a cure is possible. The American Cancer Society has decreased the recommended age of screening for CRC from 50 to 45 years, not just in African Americans and other high-risk people but to all individuals [10]. However, there was still a debate between different organizations including the United States Multi-Society Task Force (USPSTF) on Colorectal Cancer to keep the screening age at 50 years due to insufficient evidence. But USPSTF recently drafted a recommendation supporting the screening age for CRC at 45 for average-risk individuals [11]. The downside of moving the age of initiation to age 45 is decreased efficiency. Specifically, it increases the number of colonoscopies per year of life saved by about 10% (11.97 to 13.16) for colonoscopy-based screening [11] which is particularly concerning given the already strained system/resources. The performance of this strategy in a racially diverse safety net population has not been elucidated. BMC being the largest safety net population in New England does high number of colonoscopy per year (Appendix 1); serves the diverse patient population including low-income communities, elders, disability, immigrants; and also has referrals from mostly 14 different community health centers of Boston health. Since tailoring recommendations to these populations is critical, we wanted to examine the time trends of CRC incidence at BMC, the largest safety-net hospital in New England, which serves a diverse population. We wanted to focus on both the incidence of CRC, characteristics of CRC, and CRC-diagnosed patients and survival.
Methods
Study design
A retrospective cohort study was conducted in the patients with a diagnosis of Colorectal Cancer in the Clinical Data Warehouse of BMC from 2004 to 2019. We searched populations who underwent colonoscopy. If the same person had multiple colonoscopies in a year, colonoscopy at the time of diagnosis was taken. Data for BMI, smoking, race, age, sex, American Joint Committee on Cancer (AJCC) stage of cancer, and site of cancer were taken at the same time of the colonoscopy. Also, the number of colonoscopies each year was obtained (Appendix 1). The dataset was pseudonymized and cleaned. No one had missing age at the time of the colonoscopy during our initial search. Data were categorized into two groups: young (< 50 years) and older (≥ 50 years) (Fig. 1). Ethical approval was issued by the IRB of Boston University Medical Center, and the requirement for informed consent was waived.

Total number of colonoscopy and total CRC diagnosis
Statistical analysis
The trend of change of incidence rates of colorectal cancer was analyzed in the young age population and compared with the older age population. Mean ± SD for continuous variable and percentage for categorical variables were used to characterize the data. The categorical variables were analyzed with the chi-square test. Logistic regression was used to identify the independent variables associated with CRC in the age groups. Survival probability analysis was done by the Kaplan-Meier method. The impact of variables on survival was evaluated by multivariable-Cox proportional hazard. All statistical tests were two-sided and conducted using the R studio version 1.2.5033. p values less than 0.05 were considered to indicate statistical significance. Any point estimate was considered statistically significant when the 95% confidence interval did not include 1.
Results
Baseline characteristics
Table 1 represents the baseline characteristics of the population stratified by age groups, older age group, and younger age group. The total CRC was 2485 with the older population, 2104 (84.67% and younger population, 381 (15.33%).
Incidence rate
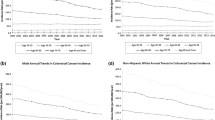
We calculated the incidence rate of each group, by CRC-diagnosed patients at BMC, of the group (younger or older), as the total number of the population of the same group who underwent colonoscopy each year per 100. The total number of the population, younger and older, who underwent colonoscopy were taken as denominators for each consecutive year. Our study revealed a higher incidence rate of CRC in the young population in the years 2010, 2012, 2013, and 2014 than the older group. And the incidence rate of CRC started to decline in 2015 and 2016 in younger groups. However, the incidence rate of CRC in the younger population started to rise again from 2017, 2018, to 2019, making a similar rate as in the older group in 2019 (Fig. 2).

Incidence rate over years comparing older and younger age groups. Here, incidence rate is calculated by number of diagnosed CRC at BMC in a year divided by number of people who undergoes colonoscopy in the same year per 100 people
Age
The overall mean age of CRC diagnosis was 63.21 years (Fig. 3). In the younger age group, the mean age of diagnosis of CRC was 41 years, and in the older age group, the mean age of diagnosis of CRC was 67 years. Among the participants who died, the mean age at the diagnosis of CRC was 68 years, and among the participants who did not die, the mean age of CRC diagnosis was 61 years (Fig. 4). In Kaplan-Meier Survival Probability, there was no significant difference between the survival probability among the younger and older age groups (Fig. 5). In the Cox proportional hazard model, holding BMI constant, older age increased the risk of death of CRC-diagnosed patients by 7% compared to a younger age. And adjusting for the BMI and stage of cancer (Stage 0 as reference), diagnosis of CRC at an older age increased the death by about 3% compared to the young age, although both of the values were not statistically significant (Table 3).

Bar diagram of age group at diagnosis of CRC in BMC population. Most of the CRC are diagnosed at 50–60 years of age

Boxplot showing death (events) in CRC-diagnosed patients. The mean age at diagnosis of CRC was higher (68 years) in the participants who died and relatively lower in the participants who did not die

Survival probability according to the age group; yellow younger, blue older. The horizontal axis (x-axis) represents time in days, and the vertical axis (y-axis) shows the probability of survival. The lines represent the survival curves of the two groups. A vertical drop in the curves indicates an event (death). At time zero, the survival probability is 1.0 (or 100% of the participants are alive). There was no significant difference between the survival probability among the younger and older age groups (p value = 0.6)
BMI
The mean BMI in the older age group was 29.3, and the younger age group was 28.8. BMI was categorized into a higher BMI group (≥ 25) and a lower BMI group (<25). Unadjusted logistic regression model revealed that for those with a higher BMI, the odds of a diagnosis of CRC increased by 19% compared to having a lower BMI at an older age group, but the value was not statistically significant (OR = 1.19, 0.816, 1.719) (Table 2). In Kaplan-Meier survival analysis, there was an actual difference in survival rates among the two BMI groups, with a CRC-diagnosed population with lower BMI having higher mortality with the p value of 0.012 (Fig. 6). In the Cox proportional hazard model adjusted for age, having a higher BMI reduced the death of the CRC-diagnosed population by 29% (Table 3), and by 41% holding age and stage of CRC constant, i.e., having lower BMI (< 25), increased the risk of death. However, our lower BMI group included the normal BMI (18.5–24.9) as well as underweight BMI, which might have skewed the result. Therefore, we did a post hoc analysis by re-stratifying BMI into true low BMI, underweight (<18.5), and normal to high BMI (≥ 18.5), to see the true effect of low BMI in mortality of CRC patients. Our analysis demonstrated being underweight (BMI ≤ 18.5) increased the risk of death in CRC-diagnosed patients by 2.34 times compared to normal to high BMI (≥18.5), irrespective of age at diagnosis and stage of cancer, and the p value was 0.014. (HR = 2.34, 95% CI 1.18, 4.63).

Survival probability according to the BMI group (<25 and ≥25). At 3000 days, the probability of survival is approximately 0.62 (or 62%) for CRC patients having BMI <25kg/m2 and 0.70 (or 70%) for BMI ≥25 kg/m2. The approximate median survival for both sexes is more than 5000 days. But there is an actual difference in survival rates among the two BMI groups, with a CRC-diagnosed population with lower BMI having higher mortality. The p value was 0.012
Stage of cancer
The AJCC categorizes CRC from Stage 0 to Stage 4. In our study, a higher number of the younger population were diagnosed at a later stage (stage 3 and 4) of CRC compared to the older population. Similarly, a higher percentage of the older population was diagnosed at an earlier stage of CRC (stage 1 and 2) (Table 1). Adjusted multivariable Cox model showed that having stage 4 CRC increases the risk of death in CRC by 3.50 compared to stage 0, holding age at diagnosis, and BMI constant. However, in the lower stage like stage 1, the risk of having death reduces by 55% (Table 3).
Smoking
More of the younger population were active current smokers than the older population. Most of the ex-smokers were older. In the unadjusted logistic regression model, an ex-smoker compared to a current smoker had double the odds of diagnosing CRC at an older age (Table 2). A higher percentage of the younger population were non-smokers, and we did not have the smoking status of some of the population from both the groups (Table 1).
Primary site of CRC
The primary site of involvement of CRC was similar in older and younger age groups. However, the involvement of the rectum as a primary site was higher in the younger population than the older population (33.33% vs 25.93%). Also, CRC of the recto-sigmoid area and the splenic flexure was higher in the younger population than the older population, although the absolute numbers were very small (Table 1).
Race
In our dataset, Hispanics were treated as a separate race. There was almost double the percentage of young Hispanics than older ones. In the logistic regression model, the odds of a diagnosis of CRC at an older age group in Hispanics were about half that of the older age white population (OR= 0.468, 95% CI 0.285, 0.796) (Table 2). There was no effect of other races on the age of diagnosis of CRC. However, those who declined to reveal the race had decreased odds of CRC diagnosis at an older age group compared to white (Table 2).
Discussion
The study retrospectively examined the change in the incidence of CRC diagnosis over the past 15 years and found that the incidence rate of CRC has been increasing in the younger population, especially in the last few years. Also, rectal cancer as a primary site was increasing in the young population. Our study also revealed that people with a lower BMI had a higher risk of mortality among CRC-diagnosed patients, and Hispanics in the younger age group were more likely to be diagnosed with CRC than the older age group.
Our study showed an increase in the incidence of CRC in young populations in the years 2012–2014 and again in 2017 and beyond. This increase in the incidence of CRC was similar to other studies which showed an increase in the incidence rates of CRC in the adults aged 20–49 years in the USA, with the largest increase in age 40–49 years [12, 13]. So far, little is known about the cause of the increase in CRC in the younger population. Over the years, the increase of CRC in the younger population could be due to an increase in the risk factors which include sedentary life [14], poor diet with more red meat and less fiber-containing food, smoking, or alcohol consumptions [13]. Modern dietary regimens which include colorants and preservatives might have altered the microbiome in the colon or have acted as direct carcinogenesis on intestinal cells. A study with de novo introduction of Western-style high-fat, low-fiber diet initiates inflammation and proliferation in colonic mucosa within 2 weeks [15]. Likewise, the widespread use of antibiotics altering the microbiome of the gut or increased C-section delivery [16] in later generations might have altered the development of the immune system, leading to early CRC cases. However, we still cannot explain the decrease in CRC in the years 2015 and 2016 in our study of the younger population. One of the explanations could be that most of the participants who underwent screening in those years might have already removed the premalignant lesions and were only having a follow-up screening or were just more health concerned. However, our dataset did not have the cause for a colonoscopy at baseline. Large epidemiological and preclinical studies are warranted in the future to assess the clinical pathological and biological factors associated with the trend of CRC over the years in younger populations [13].
Unfortunately, young populations in our study were mostly diagnosed only at stage 3 and stage 4 of CRC which is consistent with the results from previous studies [17]. This highlights the real increase in the incidence in younger adults and is not merely attributable to the earlier detection of CRC. Despite the worrisome increase in the incidence of CRC shown by previous studies [18], no earlier preventative screening has been mandated yet, in the younger population. However, a new recommendation for screening for CRC has been drafted by USPSTF recently. Nonetheless, a significant number of the young population with CRC will still be missed as our study reveals the mean age of diagnosis of 41 in the young population. Colonoscopy is not done regularly at a young age (<50 years) unless participants in this age group have risk factors of developing colon cancers like ulcerative colitis, family history of colon cancer, history of radiation to treat other cancers, confirmed or suspected hereditary colorectal cancer syndromes (Familial Adenomatous Polyposis, Lynch Syndrome), or were symptomatic/bleeding. This makes the younger population in our study already a high risk to have CRC and might have affected the survival probability in younger adults. Our study shows no statistically significant difference in survival among the older and younger populations albeit the younger population was diagnosed at an advanced stage of CRC. However, the death rate was not attributable to CRC alone as the cause of death was not known. The older population might have had other comorbidities which led to the early death resulting in no difference in survival with the younger population. Also, our study did not include the immunohistochemistry and type of CRC. This could have limited our ability to detect the difference in survival.
Furthermore, the mean age at diagnosis of CRC was higher (68 years) in the participants who died and relatively lower in the participants who did not die (Fig. 4). This shift of mean age toward the older age is likely due to the unequal distribution of population in two groups as our study consisted of a younger population nearly one-fifth the size of the older population. However, one possible explanation for the higher mean age for diagnosis of CRC in the population who died could be the lack of regular screening and diagnosis only at later stages of CRC when the treatment is less effective. Nevertheless, different factors like the type of cancer and underlying comorbidities might affect mortality. We did not have enough data to assess the cause of mortality, and further study is needed in the future in CRC-diagnosed patients stratified by the age groups.
Our study demonstrated a higher percentage of involvement of the rectum as a primary site in the younger population (33.33% vs 25.93%). Rectal cancers are usually clinically more evident by overt blood mixed with the stool, pencil-stool reflecting constriction of the lumen, and pain while sitting. However, colon cancer presentations are usually vague like anemia, abdominal pain, diarrhea, and fatigue [19]. This might have prompted symptomatic young adults to undergo screening for CRC although our dataset does not include the cause for colonoscopy. Since rectal cancer metastasis is more localized below the peritoneal reflection, screening and diagnosis at an earlier stage will help to increase the survival of the younger population.
Obesity is an established risk factor for CRC. Our study showed only a small difference in BMI in two groups attributing marginally high mean BMI in the older age group. Participants with higher BMI (≥25) had higher odds (19%) of diagnosing CRC at an older age group, although this was not statistically significant. One of the interesting findings was that there was an actual difference in survival rates among the two BMI groups, with a CRC-diagnosed population with lower BMI having higher mortality. One possible explanation could be that later stages of CRC usually have lower BMI, leading to higher mortality and showing a paradoxical effect of BMI in survival [20]. However, we had the BMI at the time of diagnosis of CRC only, and we did not know the progression of the BMI before and after the diagnosis of the CRC. Moreover, our dataset was limited by the lower number of underweight population in each stage of CRC, and we were not able to analyze the BMI with the stage of cancer. Therefore, a future prospective study in a large cohort of patients is needed to see the progression of BMI in the young population along with the stage of cancer and its relationship with survival.
Smoking is also a known risk factor for CRC. Our study revealed that ex-smokers compared to current smokers have twice the odds of diagnosing CRC at an older age (Table 2). Even controlling for BMI, ex-smoker had still a higher risk of diagnosing CRC at an older age. One of the possible explanations could be higher exposure of smoking in the older population with a change in exposure with the diagnosis of CRC [21]. However, we do not know the number of pack-years of smoking of the participants, and the exposure level of smoking before and after the diagnosis of CRC, limited by the retrospective nature of the data collection. Since most of the younger populations were non-smokers or current smokers, smoking might not have contributed to the increase in the incidence of CRC in the younger population despite nicotine being an established risk factor for CRC by different mechanisms including increasing cell proliferation [22] and migration [23].
Hispanics had a higher chance of being diagnosed with CRC at a younger age group by 53% (Table 2), which was similar to the findings from other studies [24]. However, irrespective of age, the incidence rate of CRC was rising in Hispanics compared to non-Hispanics white and AA [25]. One of the reasons could be the Hispanic diet in the US population, which includes a large proportion of red meat [26]. Shared risk factors like metabolic syndrome, with other gastrointestinal cancers (such as liver or gastric cancer), could also account for increasing CRC diagnosis in younger Hispanics [13]. Consideration of other possibilities like increase in HPV infection with integration into the colorectal tumor in the Hispanic population [27], significant health screening barriers due to lack of insurance, transportation, language, and culture [28] should be taken in future studies with the attention to the Hispanic population.
Our study has several limitations. The young age group population was already at higher risk of developing CRC as they had colonoscopy despite being below the screening age for colonoscopy. This might have led to the selection bias. However, we also do not know what proportion of the older population was diagnosed with CRC by screening alone and we do not know the indication of the colonoscopy irrespective of age group. Second, age, BMI, and smoking status were taken at the time of enrollment only. These factors can be changed throughout the follow-up years which might impact survival. Third, there were no data available on exercise, diet pattern, or aspirin intake which might impact the progression of CRC. We also did not have complete data on family history or alcohol consumption which affect the development of cancer. We were also unable to assess the immunohistochemistry of CRC, comorbidities due to incomplete data which might have affected the difference in survival of the CRC patients. Future studies are needed including all these missing covariates. Despite all these limitations of a retrospective study, our study had a large number of participants from 15 years. Also, Boston Medical Center (BMC) is a safety net hospital that provides service to a wide socioeconomic range of population, with diverse ethnicity similar to the population of the USA. We believe our study is generalizable to the population of the USA. This is the first study to tailor the screening recommendation for CRC for subpopulations after the new recommendation drafted by USPSTF.
Having the screening cut-off age of 50 years, younger populations are usually diagnosed at an advanced stage of CRC. Our study suggests advanced stages of CRC are also usually associated with low BMI, and our study shows low BMI has low survival. This supports the importance of timely evaluation of CRC. Only if such a population could be identified and screened in the earlier years or regular screening age decreased to younger years, perhaps early mortality from CRC could have been prevented. With the higher prevalence of rectal cancer in the younger population, particular attention should be given to an early detection strategy. A further prospective cohort study is needed including diet pattern, amount of exercise, the progression of BMI over the years, reasons for colonoscopy, aspirin or COX-2 inhibitor use, family history of CRC, history of ulcerative colitis, polyposis syndrome, and other comorbidities. CRC screening recommendations may vary in these populations. This will give us more clarity about the difference in the risk factors for the development of CRC in the younger and older population. Also, a prospective study focusing on only younger populations and Hispanics subpopulation should be done to identify the benefit of regular screening, at a minimum with non-invasive methods like guaiac-based fecal occult blood test (gFOBT) or fecal immunochemical test (FIT) starting at a younger age like 40–45. This will further support the updated recommendations for CRC screening at age 45 in average-risk individuals.
In conclusion, CRC is increasing in the younger population with a higher prevalence of rectum as a primary site. With the higher diagnosis of CRC in young Hispanic, early screening is warranted in such a high-risk population for early recognition for prevention, early management, and reduction of mortality. It is encouraging to see the new recommendations drafted for CRC screening from 45 years for average-risk individuals. However, screening, at minimum non-invasive screening, should be done in the young Hispanic population even from an earlier age like 40 years.
References
Keum N, Giovannucci E (2019) Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 16(12):713–732
Colorectal Cancer Guideline | How often to have screening tests. [cited 2020 Nov 23]. Available from: https://www.cancer.org/cancer/colon-rectal-cancer/detection-diagnosis-staging/acs-recommendations.html
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 68(6):394–424
SEER Incidence Database - SEER Data & Software. SEER. [cited 2020 Nov 23]. Available from: https://seer.cancer.gov/data/index.html
Siegel RL, Fedewa SA, Anderson WF, Miller KD, Ma J, Rosenberg PS et al (2017) Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst. 109(8)
Araghi M, Soerjomataram I, Bardot A, Ferlay J, Cabasag CJ, Morrison DS, de P, Tervonen H, Walsh PM, Bucher O, Engholm G, Jackson C, McClure C, Woods RR, Saint-Jacques N, Morgan E, Ransom D, Thursfield V, Møller B, Leonfellner S, Guren MG, Bray F, Arnold M (2019) Changes in colorectal cancer incidence in seven high-income countries: a population-based study. Lancet Gastroenterol Hepatol. 4(7):511–518
Siegel RL, Miller KD, Jemal A (2017) Colorectal cancer mortality rates in adults aged 20 to 54 years in the United States, 1970-2014. JAMA 318(6):572–574
Wu S, Zhu W, Thompson P, Hannun YA. Evaluating intrinsic and non-intrinsic cancer risk factors. Nature Communications. 2018 [cited 2020 Nov 23];9(1):3490. Available from: https://www.nature.com/articles/s41467-018-05467-z
Stryker SJ, Wolff BG, Culp CE, Libbe SD, Ilstrup DM, MacCarty RL (1987) Natural history of untreated colonic polyps. Gastroenterology. 93(5):1009–1013
Wolf AMD, Fontham ETH, Church TR, Flowers CR, Guerra CE, LaMonte SJ, Etzioni R, McKenna M, Oeffinger KC, Shih YT, Walter LC, Andrews KS, Brawley OW, Brooks D, Fedewa SA, Manassaram-Baptiste D, Siegel RL, Wender RC, Smith RA (2018) Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 68(4):250–281
Draft Recommendation: Colorectal Cancer: Screening | United States Preventive Services Taskforce. [cited 2020 Nov 27]. Available from: https://uspreventiveservicestaskforce.org/uspstf/draft-recommendation/colorectal-cancer-screening3
SEER*Stat Databases: November 2015 Submission. SEER. [cited 2020 Dec 1]. Available from: https://seer.cancer.gov/data-software/documentation/seerstat/nov2015/index.html
Stoffel EM, Murphy CC (2020) Epidemiology and mechanisms of the increasing incidence of colon and rectal cancers in young adults. Gastroenterology. 158(2):341–353
Clark B, Sugiyama T. Prevalence, trends, and correlates of sedentary behavior. In: Kanosue K, Oshima S, Cao Z-B, Oka K, editors. Physical Activity, Exercise, Sedentary Behavior and Health. Tokyo: Springer Japan; 2015 [cited 2020 Dec 1]. p. 79–90. Available from: https://doi.org/10.1007/978-4-431-55333-5_8
O’Keefe SJD, Li JV, Lahti L, Ou J, Carbonero F, Mohammed K, Posma JM, Kinross J, Wahl E, Ruder E, Vipperla K, Naidoo V, Mtshali L, Tims S, Puylaert PGB, DeLany J, Krasinskas A, Benefiel AC, Kaseb HO, Newton K, Nicholson JK, de Vos WM, Gaskins HR, Zoetendal EG (2015) Fat, fibre and cancer risk in African Americans and rural Africans. Nat Commun. 6:6342
Dominguez-Bello MG, Costello EK, Contreras M, Magris M, Hidalgo G, Fierer N, et al. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc Natl Acad Sci USA. 2010 Jun 29;107(26):11971. Available from: http://www.pnas.org/content/107/26/11971.abstract
You YN. Young-onset colorectal cancer: is it time to pay attention? Arch Intern Med [Internet]. 2012 Feb 13 [cited 2020 Nov 23];172(3):287. Available from: http://archinte.jamanetwork.com/article.aspx?doi=10.1001/archinternmed.2011.602
Meester RGS, Mannalithara A, Lansdorp-Vogelaar I, Ladabaum U. Trends in incidence and stage at diagnosis of colorectal cancer in adults aged 40 through 49 years, 1975-2015. JAMA. 2019 May 21 [cited 2020 Nov 23];321(19):1933. Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2019.3076
Paschke S, Jafarov S, Staib L, Kreuser E-D, Maulbecker-Armstrong C, Roitman M, et al. Are colon and rectal cancer two different tumor entities? A proposal to abandon the term colorectal cancer. Int J Mol Sci. 2018 Aug 30 [cited 2020 Nov 23];19(9). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6165083/
Ch K, R N, J M, Cm P, E W, Ml K, et al. Analysis of body mass index and mortality in patients with colorectal cancer using causal diagrams. JAMA Oncol. 2016 Sep 1 [cited 2020 Nov 23];2(9):1137–45. Available from: https://europepmc.org/article/pmc/pmc5016213
Siegel RL, Jemal A, Ward EM (2009) Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev. 18(6):1695–1698
Nicotine stimulates proliferation and inhibits apoptosis in colon cancer cell lines through activation of survival pathways. - Abstract - Europe PMC. [cited 2020 Nov 23]. Available from: https://europepmc.org/article/med/22520577
Wei P-L, Kuo L-J, Huang M-T, Ting W-C, Ho Y-S, Wang W, An J, Chang YJ (2011) Nicotine enhances colon cancer cell migration by induction of fibronectin. Ann Surg Oncol. 18(6):1782–1790
Wang DY, Thrift AP, Zarrin-Khameh N, Wichmann A, Armstrong GN, Thompson PA, et al. Rising incidence of colorectal cancer among young Hispanics in Texas. J Clin Gastroenterol. 2017 Jan [cited 2020 Nov 23];51(1):34–42. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5157697/
Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer health disparities in racial/ethnic minorities in the United States. British Journal of Cancer. 2020 Sep 9 [cited 2020 Dec 1];1–18. Available from: https://www.nature.com/articles/s41416-020-01038-6
Daniel CR, Cross AJ, Koebnick C, Sinha R (2011) Trends in meat consumption in the USA. Public Health Nutr. 14(4):575–583
Bernabe-Dones RD, Gonzalez-Pons M, Villar-Prados A, Lacourt-Ventura M, Rodríguez-Arroyo H, Fonseca-Williams S, et al. High prevalence of human papillomavirus in colorectal cancer in Hispanics: a case-control study. Gastroenterology Research and Practice. 2016 [cited 2020 Nov 23];2016:7896716. Available from: https://jhu.pure.elsevier.com/en/publications/high-prevalence-of-human-papillomavirus-in-colorectal-cancer-in-h-3
Fernández ME, Savas LS, Carmack CC, Chan W, Lairson DR, Byrd TL, Wilson KM, Arvey SR, Krasny S, Vernon SW (2015) A randomized controlled trial of two interventions to increase colorectal cancer screening among Hispanics on the Texas-Mexico border. Cancer Causes Control. 26(1):1–10
Acknowledgements
We thank Dr Janice Weinberg and Stacey Hess Pino for their useful suggestions and comments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr Hemant Kumar Roy received grant from National Cancer Institute 1R33CA225323-01.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 70 kb)
Rights and permissions
About this article

Cite this article
Pandey, S., Fish, S.S. & Roy, H.K. Increasing colorectal cancer in the young population and tailoring of the colorectal cancer screening recommendations in subpopulation: a retrospective single-center study. Int J Colorectal Dis 36, 1515–1524 (2021). https://doi.org/10.1007/s00384-021-03934-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-021-03934-6