
Abstract
Purpose
The association between antibiotics and colorectal cancer (CRC) risk has drawn increasing attention but remains controversial. This study was performed to clarify the association.
Methods
A systematic review and meta-analysis was performed on seven electronic databases. The pooled odds ratios (OR) with a 95% confidence interval (CI) were calculated to estimate the association using the fixed-effects model or the random-effects model.
Results
Ten studies that contained 4,853,289 participants were included in our study. We found that antibiotics use was associated with a higher risk of CRC (OR 1.09, 95%CI 1.02–1.17, I2 = 92.8%). More than 60 days of antibiotics use and 5 prescriptions of antibiotics were significantly associated with a higher risk of CRC. Sub-analysis on different types of antibiotics found that anti-anaerobic antibiotics, penicillins, and quinolones use led to increased risk of CRC (OR 1.22, 95% CI 1.04–1.44, I2 = 89.1%; OR 1.09, 95% CI 1.04–1.13, I2 = 69.2%; OR 1.15, 95% CI 1.03–1.35, I2 = 88.2%; respectively) and colon cancer (OR 1.28, 95% CI 1.04–1.58, I2 = 98.5%; OR 1.09, 95% CI 1.05–1.12, I2 = 0; OR 1.09, 95% CI 1.04–1.15, I2 = 0; respectively). However, antibiotics use was not significantly associated with rectal cancer (OR 1.03, 95% CI 0.92–1.16, I2 = 77.6%).
Conclusion
It needs attention that antibiotics use is associated with a higher risk of CRC, especially for colon cancer. Clinicians should be aware of the potential risk of CRC when prescribing anti-anaerobic antibiotics, penicillins, and quinolones in the future. Further studies are needed to assess any potential differences by tumor sites and class of antibiotics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cancer is a major public health problem that seriously affects people’s health and quality of life. Colorectal cancer (CRC) is one of the top five most commonly diagnosed cancer in both men and women [1], and is the fourth most deadly cancer worldwide after lung, liver and stomach cancers [2]. Studies showed that the incidence rate of CRC is higher in developed countries compared with developing countries [1, 2]. According to the Global Burden of Disease Study (GBD), 830,000 people died from CRC in 2016, and this number is expected to increase to 1,540,000 in 2040 [3]. This drastic increase is likely due to increase in many risk factors such as aging, smoking, low physical activity, and obesity [2, 4].
It is believed that CRC occurs due to synergy of multiple factors including genetic, environmental, and lifestyle risk factors. In recent years, with the advances in gut microbiota research, people now suspect there are connections between intestinal microorganisms and cancer [5, 6]. Previous studies confirmed that disruption of gut microbiota can lead to gastrointestinal diseases including CRC [7]. Antibiotics can destroy gut microbiota and damage the integrity of intestinal barrier [8, 9]. Furthermore, antibiotics use indirectly destroys the symbiosis that makes up the microbial community which may result in the colonization of invading bacteria and increased susceptibility to infections [10]. Therefore, antibiotics may allow colonization of carcinogenic bacteria, leading to local inflammation and tumor formation. A few epidemiological studies have already shown the positive relationship between CRC and antibiotics use, but the results vary widely. A nested case-control study in Asian population reported that anti-anaerobic antibiotics use was associated with a higher risk of colon cancer and rectal cancer, but it was not significant for the relationship between anti-aerobic agents and CRC [11]. However, another nested case-control study from the Netherlands found that both anti-anaerobic and anti-aerobic agents lead to increased risk of CRC [12]. Additionally, a study in the UK found that oral antibiotics use was associated with an increased risk of colon cancer but a reduced risk of rectal cancer [13]. Therefore, the link between antibiotics use and CRC risk remains controversial and needs further exploration.
Therefore, we performed a systematic review and meta-analysis to evaluate the relationship between antibiotics use and CRC risk. We also performed sub-analyses on the tumor location and class of antibiotics to explore whether these correlations were varied among different classes of antibiotics use or different types of cancer (colon and rectal cancer).
Methods
This study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [14] (supplementary material).
Search strategy
A comprehensive literature search was performed in PubMed, Web of Science, and ScienceDirect databases from database construction to November 2, 2019. The recently updated search was conducted in February 2020. We used the following search terms: “antibiotic,” “anti-bacterial agent,” “colorectal,” “colon,” “rectum,” “rectal,” “cancer,” “neoplasm,” “carcinoma,” and “adenoma”. Full search steps in each database were provided in the supplementary material. We did not limit the searches by languages or regions. We also reviewed the reference list of the included articles for additional studies.
Study selection
Two authors independently carried out the search and disagreements were solved by consensus. The abstract of the retrieved studies was reviewed initially and excluded if deemed irrelevant. The full text of the relevant studies was further reviewed for eligibility. If there were duplicate publications of the same study, the one with the most detailed information and complete data was included.
Studies included in this meta-analysis must meet all of the following criteria: (1) participants were adults without any prior history of cancer; (2) the study design was case-control or cohort; (3) exposure was any history of antibiotics use and the main outcome included CRC or colon cancer or rectal cancer; and (4) the effect size reflecting the association between CRC and antibiotic use was reported or the data that can be used to indirectly calculate the effect size was available. In addition, studies which had one of the following characteristics were excluded: (1) studies did not meet the inclusion criteria; (2) participants with known concomitant antibiotic use at the time when CRC was diagnosed or it was difficult to determine the sequence of antibiotic use and CRC diagnosis; (3) the study was a case report, animal experiment, or review; and (4) the criteria for CRC diagnosis were not clearly reported.
Data extraction
We extracted the following data from each eligible studies: first author’s name, year of publication, study region, number of participants in case and control groups, age of participants, main characteristics of participants, study design, comparison of antibiotic groups, cumulative time of antibiotics use, number of prescribed doses, antibiotics class, type of CRC evaluated, adjusted odds ratios (ORs) or relative risks (RRs) with most multiple factors adjusted, and covariates or confounders for effect size adjustment. For studies that did not report ORs or RRs, we extracted the number of antibiotics use/CRC in different groups to calculate crude effect sizes.
Quality assessment of included studies
Considering that the included studies were all observational studies (case-control and cohort), the Newcastle-Ottawa Scale (NOS) was adapted to assess the quality of evidence. NOS is an 8-item scale that evaluates the quality of the literature from three aspects (participant selection, comparability, and assessment of exposure or outcome) [15]. Each included study was characterized as being at low-, moderate-, or high-quality according to the scores assessed on NOS (0–3, 4–6, 7–9, respectively).
Statistical analysis
To comprehensively reveal the association between antibiotics use and CRC risk, meta-analyses were performed contained the following steps. First, the association between any antibiotics use and total CRC risk was clarified through pooling ORs extracted from included studies. Second, we grouped the antibiotics by class and further conducted meta-analysis to assess the relationship between different classes of antibiotics and CRC risk. Third, the ORs of the comparison of different duration of antibiotics exposure and number of prescriptions with no antibiotics use (if they were reported in included studies) were pooled. Fourth, subgroup analyses of the association between antibiotics use and total CRC risk were also conducted based on the characteristics of included studies (such as characteristics of participants, study design, and adjusted covariates/confounders) to explore the diversity of the association and also explore the source of heterogeneity. Finally, similar analysis strategies mentioned above were applied separately to colon and rectal cancers to explore if there was any difference in the association based on different tumor sites. The pooled effect sizes were displayed as ORs with corresponding 95% confidence intervals (CIs). Heterogeneity between studies was evaluated using the I-squared test and Cochrane Q test. Heterogeneity was defined as P value < 0.1 on the Q test. If heterogeneity is present, random-effects model (DerSimonian-Laird method) was used to create forest plots. If not present, the fixed-effects model was adopted (Mantel-Haenszel method) [16, 17]. Publication bias was assessed by funnel plots. Publication bias was defined as positive when the P value of the Begg’s and Egger’s test is less than 0.05 [17]. Sensitivity analysis was also conducted by omitting studies one by one to identify the stability of the results of meta-analysis. All statistical analyses were performed using the STATA 14.0 software.
Results
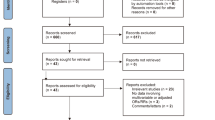
After initial literature search, we identified 10,426 records. After checking for duplicates, 8920 were left for title and abstract review. Eventually, 10 studies are included in the final meta-analysis [11,12,13, 18,19,20,21,22,23,24]. Detailed process of literature screening is shown in Fig. 1.

Flow diagram of study selection
Characteristics of included studies
Characteristics of the ten studies are summarized in Table 1. Overall, 4,853,289 participants were included and study sample sizes ranged from 4403 to 3,112,624 participants. All participants of included studies were adults. Six studies reported that participants with some diseases (i.e., inflammatory bowel disease or familial adenomatous polyposis) predispose to CRC were excluded [11,12,13, 18, 21, 23], but one study did not give detailed characteristics of the participants [24]. Of the 10 studies, eight were case-control studies [11,12,13, 18, 19,21, 23, 24] and two were cohort studies [20, 22]. Five studies were from Europe [12, 13, 18, 20, 21], four were from North America [19, 22,23,24], and one from Asia [11]. Six studies looked at different classes of antibiotics and CRC risk [11,12,13, 18, 19, 21]. Five of the studies reported the association between antibiotics use and different anatomical sites of CRC risk (colon cancer or rectal cancer) [11, 13, 20, 23, 24]. Seven studies were of moderate quality [11, 12, 18, 19, 21, 22, 24] and three were of high-quality based on NOS [13, 20, 23].
Antibiotic use and CRC risk
Our study showed that antibiotics use was significantly associated with higher risk of CRC (OR 1.09, 95% CI 1.02–1.17, P = 0.007, I2 = 92.8%) (Fig. 2). Furthermore, anti-anaerobic antibiotics were associated with increased risk (OR 1.22, 95% CI 1.04–1.44, P = 0.012, I2 = 89.1%), but not anti-aerobic antibiotics use (OR 1.03, 95% CI 0.98–1.08, P = 0.282, I2 = 60.2%). More than 60 days of antibiotics use and more than five numbers of prescription were both associated with increased CRC risk (OR 1.22, 95% CI 1.07–1.40, P = 0.003, I2 = 48.3% and OR 1.39, 95% CI 1.06–1.18, P = 0.019, I2 = 98.7%). For different classes of antibiotics, only penicillins (OR 1.09, 95% CI 1.04–1.13, P < 0.001, I2 = 69.2%) and quinolones (OR 1.15, 95% CI 1.03–1.35, P = 0.012, I2 = 88.2%) were associated with higher risk of CRC. No positive correlation was found for the other antibiotics (cephalosporins, macrolides, sulfonamides and trimethoprim, tetracyclines, and nitroimidazoles) (P for significance > 0.05). The positive association between any antibiotics use and CRC risk was also found in patients without inflammatory bowel disease, cohort or case-control studies, Europe patients, and studies which adjusted multiple confounders (Table 2).

Forest plot of the association between antibiotic use and the risk of colorectal cancer
Antibiotic use and colon cancer risk
Antibiotics use was not shown significant association with increased risk of colon cancer (OR 1.07, 95% CI 0.99–1.16, P = 0.07, I2 = 74.1%) (Fig. 3). However, the analyses stratified by antibiotics class did show an obvious association between anti-anaerobic use and colon cancer risk (OR 1.28, 95% CI 1.04–1.58, P = 0.020, I2 = 98.5%), but not for anti-aerobic antibiotic (OR 1.02, 95% CI 0.98–1.05, P = 0.353, I2 = 43.1% for anti-aerobic use). Additionally, we also found penicillins and quinolones use was associated with a higher risk of colon cancer (OR 1.09, 95% CI 1.06–1.13, P < 0.001, I2 = 0 for penicillins; OR 1.09, 95% CI 1.04–1.15, P = 0.001, I2 = 0 for quinolones), whereas cephalosporins use was not associated with an excess colon cancer risk (OR 1.71, 95% CI 0.69–4.23, P = 0.246, I2 = 99.3% ). In addition, subgroup analyses on studies with high-quality and studies contained patients from Europe identified the positive association between any antibiotics use and colon cancer risk (Table 2).

Forest plot of the association between antibiotic use and the risk of colon cancer
Antibiotic use and rectal cancer risk
Contrary to colon cancer, antibiotics use was not significantly associated with increased risk of rectal cancer (OR 1.03, 95% CI 0.92–1.16, P = 0.577, I2 = 77.6%) (Fig. 4). Additionally, use of anti-anaerobic antibiotics, penicillins, or cephalosporins was not associated with increased rectal cancer risk, whereas anti-aerobic antibiotics use was associated with a lower risk of rectal cancer (OR 0.93, 95% CI 0.88–0.98, P = 0.012, I2 = 0), and a decreased rectal cancer risk was also found in quinolones (OR 0.92, 95% CI 0.86–0.99, P = 0.037, I2 = 39.6%). The results of subgroup analysis also indicated no significant association between antibiotic use and rectal cancer risk (Table 2).

Forest plot of the association between antibiotic use and the risk of rectal cancer
Publication bias and sensitivity analysis
No publication bias was present according to the Begg’s test (P = 0.531 for CRC, P = 0.142 for colon cancer, and P = 0.602 for rectal cancer) and Egger’s test (P = 0.446 for CRC, P = 0.124 for colon cancer, and P = 0.413 for rectal cancer). Also, sensitivity analysis by omitting studies one by one showed that no study had a significant impact on the pooled results of meta-analysis which meant that the pooled results of the meta-analysis were stable (supplementary material).
Discussion
Our meta-analysis, based on the pooled results of ten studies including 4,853,289 participants, showed that antibiotics use was associated with 9% increased risk in CRC. However, this association depends on the tumor location and the type of antibiotics. Specifically, there was no obvious association between antibiotics use and increased risk of rectal cancer, but some classes of antibiotics use were obviously associated with a higher risk of colon cancer. Furthermore, anti-anaerobic antibiotics use is associated with higher risk of CRC and colon cancer but not rectal cancer, whereas anti-aerobic antibiotics has no effect on the risk of colon cancer, and interestingly, leads to a lower risk of rectal cancer. However, considering the limited number of studies focus on the association between anti-anaerobic/aerobic antibiotics and colon and rectal cancer, this different association requires cautious interpretation, and more high-quality studies on this topic are urgently needed in the future. The primary finding of our study is consistent with a prior meta-analysis that showed antibiotics use leads to 8% increased risk of CRC [25], but inconsistent with other two meta-analyses that ever antibiotics use was not associated with CRC risk [26, 27]. Additionally, some results of separate analyses on antibiotics use and cancers at different sites of gastrointestinal tract are consistent with previous studies that antibiotics use was not associated with the risk of rectal cancer. Interestingly, different from previous meta-analyses, more information has been reported in our study that the link between different classes of antibiotics, and the risk of cancer has been further separately explored among different tumor location, and new findings are that use of anti-anaerobic antibiotics, penicillins, or quinolones was obviously associated higher risk of CRC and especially, colon cancer, which provides a cautionary message for clinicians that there are potential risks for patients’ health when prescribing these antibiotics in the future.
Although significant associations between antibiotics use and CRC and colon cancer risk had been revealed in the present study, the results of many analyses were shown with high heterogeneity. Owing to the small number of included studies, meta-regression was not appropriate for exploring the source of heterogeneity and subgroup analysis was therefore performed. The results of subgroup analyses suggested that participants with different characteristics, study design, study quality, and study region may be the causes of huge heterogeneity. In addition, most all results of subgroup analyses were consistent with the main analyses. This may indicate that the existence of high heterogeneity does not affect the validity of the final conclusion. However, it needs attention that our study is not able to determine the causal relationship between antibiotics use and CRC because that all included studies were observational design (most were case-control), and the CRC is expected to take 8–10 years to develop [11], but the follow-up period for the antibiotics exposure of most included studies was less than 8 years. In addition, as discussed in the previous studies, no duration-response relationship was found for the cumulative measures of antibiotics exposure, and a higher risk was found in short duration of antibiotic use compared with long duration of antibiotic use [11, 13]. Therefore, all these implied that antibiotics use may be a promotion rather than an etiology for CRC. Whether there is a causal relationship between antibiotics use and CRC should be further explored and confirmed by prospective study with a longer follow-up period.
The relationship between antibiotics use and risk of CRC is possibly related to disruption of gut microbiota as previously discussed in other studies. Antibiotics use destroys the normal gut microbiota and disrupts the protection against the colonization and growth of pathogenic bacteria. Antibiotics also affects the production of bacteriocin which results in systemic inflammation and growth of latent cancer cells [10, 28, 29]. Additionally, the gut microbiota is also part of our innate immune system and assists our immune system to recognize, and attack opportunistic infections have a powerful role in shaping the immune system of the host body, one of which is to enable the immune system to recognize and attack opportunistic bacteria thereby preventing bacterial invasion and infection [29, 30]. However, this layer of protection is affected by antibiotics use [31].
Our study also demonstrated that the association between antibiotics and CRC is dependent on the type of antibiotics. This is possibly due to differences in the enrichment areas of putative carcinogenic bacteria and normal microorganisms in the gut and the varied anti-bacterial effects of different antibiotics [13]. Our study showed that anti-anaerobic antibiotics lead to an increased risk of CRC. This is because the gut microbiota is predominately composed of anaerobes; therefore, anti-anaerobic antibiotics will have a bigger effect on the bacterial composition in the gut, leading to mucosal immune or inflammatory deregulation [32, 33]. Our study also showed that penicillins are associated with CRC and colon cancer risk but not rectal cancer risk. This is possibly because penicillins affect parts of the gut differently. Zhang and his colleagues demonstrated that penicillins only led to increased risk of cancer in proximal colon [13]. One explanation is that the commonly used penicillins are anti-anaerobes, and proximal colon is the site of first exposure. Afterwards, the drug may undergo modification or degradation in distal colon and rectum, diminishing its anti-anaerobic effects distally [13, 18]. Additionally, our study showed that quinolones are associated with slightly higher CRC and colon cancer risk, and a lower rectal cancer risk. It is unclear the exact mechanism for now. Currently, there’s not enough studies available to fully explain this difference. However, we do know that quinolones can lead to turbulence of gut microbiota and lead to infection by harmful bacteria [34, 35]. One possible explanation is that the distribution of both pathogenic and physiological bacteria is location dependent [13]. For example, Fusobacterium nucleatum, an important bacterium associated with CRC, descends in a gradient fashion from cecum to rectum, with the highest concentration in proximal colon cancer [36]. Another explanation is that quinolones have anti-cancer effects; they have cytotoxic activity against cancer cells and are type II topoisomerase and tubulin polymerization inhibitors [37, 38]. Furthermore, ciprofloxacin, a commonly used fluoroquinolone, has been proved to induce apoptosis and inhibit the proliferation of human colorectal carcinoma cells [39]. Vosaroxin, a 4-quinolone derivative, induces DNA damage by intercalating DNA and inhibiting topoisomerase II that leads to cancer cell apoptosis, and it is currently in phase III clinical trials for the treatment of acute myelogenous leukemia [40,41,42]. However, this may not fully explain why quinolones are associated with a higher risk of CRC and colon cancers but not rectal cancers. Our study showed that cephalosporins had no significant association with colon cancer, rectum cancer, and overall colorectal cancer, nor did sulfonamides and trimethoprim, tetracycline, and nitroimidazoles; this is contrary to previously published results [25]. This discrepancy is likely because the previous study did neither breakdown CRC by tumor site nor breakdown antibiotics by class. More prospective studies with larger sample sizes are needed to confirm our findings in the future.
To our knowledge, this study is a first meta-analysis to comprehensively analyze the association between different classes of antibiotics use and risk of colon cancer, rectal cancer, and overall CRC. Advantages of our study include a large sample size of over 4.8 million participants, making our results more reliable than previous studies. We also analyzed the association based on tumor site and class of antibiotics. Additionally, we used adjusted OR values to minimize confounders. One of the limitations of our study is the limited information reported in the included studies. It is known that the duration and cumulative dosage of antibiotics use are also important variables for the risk of cancer; but this information reported was not exactly the same or not reported in some studies. Therefore, we could only compare the CRC risk of a certain duration interval of antibiotic use or a certain interval of number of antibiotics prescriptions versus non-use. However, due to lack of enough data from original studies, it cannot be well-elaborated that whether different duration or cumulative dosage of antibiotics use is associated with the risk of colon cancer and whether the cancer risk increases linearly with the duration of use and cumulative dosage of antibiotics. Another limitation is that some studies only adjusted one or two covariates for the risk estimation, and some important factors associated with cancer risk such as diet, family history of CRC, and physical activity were not reported or well-adjusted in all studies, which may cause a certain bias for the pooled results of our study. This suggests that future research should adjust for as many confounders as possible, especially those known, in order to gain a more authentic understanding of the relationship between antibiotics use and cancer risk. Finally, there was significant heterogeneity among pooled meta-analysis, and the sources of some heterogeneity can be explained by the quality of included studies and study region; therefore, further studies with high-quality are needed to confirm our findings.
Conclusion
In conclusion, this meta-analysis demonstrated that antibiotics use is associated with increased CRC risk, but this association is depended on tumor site and types of antibiotics. Antibiotics use may be associated with a higher risk of colon cancer but not significant for rectal cancer. Anti-anaerobic antibiotics, penicillins, and quinolones are more likely to lead to CRC and colon cancer. Clinicians should be aware of this potential risk on CRC, especially for colon cancer when prescribing anti-anaerobic antibiotics, penicillins, and quinolones in the future.
Authorship and contributions
Guangbo Qu and Chenyu Sun contributed to study design and developed the research protocol; Guangbo Qu and Liqin Shu conducted study search and selection; Chenyu Sun extracted data; Guangbo Qu performed statistical analyses and drafted the manuscript; Monica Sharma, John Patrick Uy, Evelyn J. Song, Chandur Bhan, and Liqin Shu viewed and revised the manuscript. The final version of the manuscript approved by all authors.
References
World Health Organization (WHO) (2015) Cancer.
Brody H (2015) Colorectal cancer. Nature 521:S1
Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, Pletcher MA, Smith AE, Tang K, Yuan CW, Brown JC, Friedman J, He J, Heuton KR, Holmberg M, Patel DJ, Reidy P, Carter A, Cercy K, Chapin A, Douwes-Schultz D, Frank T, Goettsch F, Liu PY, Nandakumar V, Reitsma MB, Reuter V, Sadat N, Sorensen RJD, Srinivasan V, Updike RL, York H, Lopez AD, Lozano R, Lim SS, Mokdad AH, Vollset SE, Murray CJL (2018) Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 392:2052–2090
Kuipers EJ, Grady WM, Lieberman D, Seufferlein T, Sung JJ, Boelens PG, van de Velde CJH, Watanabe T (2015) Colorectal cancer. Nat Rev Dis Primers 1:15065
Yu LX, Schwabe RF (2017) The gut microbiome and liver cancer: mechanisms and clinical translation. Nat Rev Gastroenterol Hepatol 14:527–539
Lucas C, Barnich N, Nguyen HTT (2017) Microbiota, inflammation and colorectal cancer. Int J Mol Sci 18:E1310
Gao R, Gao Z, Huang L, Qin H (2017) Gut microbiota and colorectal cancer. Eur J Clin Microbiol Infect Dis 36:757–769
Gibson MK, Crofts TS, Dantas G (2015) Antibiotics and the developing infant gut microbiota and resistome. Curr Opin Microbiol 27:51–56
Ianiro G, Tilg H, Gasbarrini A (2016) Antibiotics as deep modulators of gut microbiota: between good and evil. Gut 65:1906–1915
Pamer EG (2016) Resurrecting the intestinal microbiota to combat antibiotic-resistant pathogens. Science 352:535–538
Wang JL, Chang CH, Lin JW, Wu LC, Chuang LM, Lai MS (2014) Infection, antibiotic therapy and risk of colorectal cancer: a nationwide nested case-control study in patients with Type 2 diabetes mellitus. Int J Cancer 135:956–967
Dik VK, van Oijen MG, Smeets HM, Siersema PD (2016) Frequent use of antibiotics is associated with colorectal cancer risk: results of a nested case-control study. Dig Dis Sci 61:255–264
Zhang J, Haines C, Watson AJM, Hart AR, Platt MJ, Pardoll DM, Cosgrove SE, Gebo KA, Sears CL (2019) Oral antibiotic use and risk of colorectal cancer in the United Kingdom, 1989-2012: a matched case-control study. Gut 68:1971–1978
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1
Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al (2017) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed May 17, 2017).
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Boursi B, Haynes K, Mamtani R, Yang YX (2015) Impact of antibiotic exposure on the risk of colorectal cancer. Pharmacoepidemiol Drug Saf 24:534–542
Didham RC, Reith DM, McConnell DW, Harrison KS (2005) Antibiotic exposure and breast cancer in New Zealand. Breast Cancer Res Treat 92:163–167
Kilkkinen A, Rissanen H, Klaukka T, Pukkala E, Heliövaara M, Huovinen P, Männistö S, Aromaa A, Knekt P (2008) Antibiotic use predicts an increased risk of cancer. Int J Cancer 123:2152–2155
Armstrong D, Dregan A, Ashworth M, White P, McGee C, de Lusignan S (2020) The association between colorectal cancer and prior antibiotic prescriptions: case control study. Br J Cancer 122:912–917. https://doi.org/10.1038/s41416-019-0701-5
Falagas ME, Walker AM, Jick H, Ruthazer R, Griffith J, Snydman DR (1998) Late incidence of cancer after metronidazole use: a matched metronidazole user/nonuser study. Clin Infect Dis 26:384–388
Friedman GD, Coates AO, Potter JD, Slattery ML (1998) Drugs and colon cancer. Pharmacoepidemiol Drug Saf 7:99–106
Friedman GD, Jiang SF, Udaltsova N, Quesenberry CP Jr, Chan J, Habel LA (2009) Epidemiologic evaluation of pharmaceuticals with limited evidence of carcinogenicity. Int J Cancer 125:2173–2178
Petrelli F, Ghidini M, Ghidini A, Perego G, Cabiddu M, Khakoo S et al (2019) Use of antibiotics and risk of cancer: a systematic review and meta-analysis of observational studies. Cancers (Basel) 11:E1174
Wan QY, Zhao R, Wang Y, Wu Y, Wu XT (2020) Antibiotic use and risk of colorectal cancer: a meta-analysis of 412 450 participants. Gut 2020. [Epub ahead of print]:gutjnl-2020-320826. https://doi.org/10.1136/gutjnl-2020-320826
Sanyaolu LN, Oakley NJ, Nurmatov U, Dolwani S, Ahmed H (2019) Antibiotic exposure and the risk of colorectal adenoma and carcinoma: a systematic review and meta-analysis of observational studies. Colorectal Dis 2019. https://doi.org/10.1111/codi.14921
Khosravi A, Mazmanian SK (2013) Disruption of the gut microbiome as a risk factor for microbial infections. Curr Opin Microbiol 16:221–227
Gopalakrishnan V, Helmink BA, Spencer CN, Reuben A, Wargo JA (2018) The influence of the gut microbiome on cancer, immunity, and cancer immunotherapy. Cancer Cell 33:570–580
Honda K, Littman DR (2016) The microbiota in adaptive immune homeostasis and disease. Nature 535:75–84
Yang JH, Bhargava P, McCloskey D, Mao N, Palsson BO, Collins JJ (2017) Antibiotic-induced changes to the host metabolic environment inhibit drug efficacy and alter immune function. Cell Host Microbe 22:757–765
Sommer F, Bäckhed F (2013) The gut microbiota--masters of host development and physiology. Nat Rev Microbiol 11:227–238
Langdon A, Crook N, Dantas G (2016) The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med 8:39
Saxton K, Baines SD, Freeman J, O’Connor R, Wilcox MH (2009) Effects of exposure of Clostridium difficile PCR ribotypes 027 and 001 to fluoroquinolones in a human gut model. Antimicrob Agents Chemother 53:412–420
Knecht H, Neulinger SC, Heinsen FA, Knecht C, Schilhabel A, Schmitz RA, Zimmermann A, dos Santos VM, Ferrer M, Rosenstiel PC, Schreiber S, Friedrichs AK, Ott SJ (2014) Effects of β-lactam antibiotics and fluoroquinolones on human gut microbiota in relation to Clostridium difficile associated diarrhea. PLoS One 9:e89417
Mima K, Cao Y, Chan AT, Qian ZR, Nowak JA, Masugi Y, Shi Y, Song M, da Silva A, Gu M, Li W, Hamada T, Kosumi K, Hanyuda A, Liu L, Kostic AD, Giannakis M, Bullman S, Brennan CA, Milner DA, Baba H, Garraway LA, Meyerhardt JA, Garrett WS, Huttenhower C, Meyerson M, Giovannucci EL, Fuchs CS, Nishihara R, Ogino S (2016) Fusobacterium nucleatum in Colorectal carcinoma tissue according to tumor location. Clin Transl Gastroenterol 7:e200
Batalha PN, Vieira de Souza MC, Peña-Cabrera E, Cruz DC, da Costa Santos Boechat F (2016) Quinolones in the search for new anticancer agents. Curr Pharm Des 22:6009–6020
Gao F, Zhang X, Wang T, Xiao J (2019) Quinolone hybrids and their anti-cancer activities: An overview. Eur J Med Chem 165:59–79
Herold C, Ocker M, Ganslmayer M, Gerauer H, Hahn EG, Schuppan D (2002) Ciprofloxacin induces apoptosis and inhibits proliferation of human colorectal carcinoma cells. Br J Cancer 86:443–448
Liu F, Knight T, Su Y, Edwards H, Wang G, Wang Y, Taub JW, Lin H, Sun L, Ge Y (2019) Venetoclax Synergistically enhances the anti-leukemic activity of vosaroxin against acute myeloid leukemia cells ex vivo. Target Oncol 14:351–364
Ravandi F, Ritchie EK, Sayar H, Lancet JE, Craig MD, Vey N, Strickland SA, Schiller GJ, Jabbour E, Pigneux A, Horst HA, Récher C, Klimek VM, Cortes JE, Carella AM, Egyed M, Krug U, Fox JA, Craig AR, Ward R, Smith JA, Acton G, Kantarjian HM, Stuart RK (2018) Phase 3 results for vosaroxin/cytarabine in the subset of patients ≥60 years old with refractory/early relapsed acute myeloid leukemia. Haematologica 103:e514–e518
Jamieson GC, Fox JA, Poi M, Strickland SA (2016) Molecular and pharmacologic properties of the anticancer quinolone derivative vosaroxin: a new therapeutic agent for acute myeloid leukemia. Drugs 76:1245–1255
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they no conflict of interest.
Ethical approval
This systematic review and meta-analysis used previously published data and did not use any unpublished data. Therefore, ethical approval for analysis was not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOC 224 kb)
Rights and permissions
About this article

Cite this article
Qu, G., Sun, C., Sharma, M. et al. Is antibiotics use really associated with increased risk of colorectal cancer? An updated systematic review and meta-analysis of observational studies. Int J Colorectal Dis 35, 1397–1412 (2020). https://doi.org/10.1007/s00384-020-03658-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-020-03658-z