
Abstract
Purpose
Hospital factors along with various patient and surgeon factors are considered to affect the prognosis of colorectal cancer. Hospital volume is well known, but little is known regarding other hospital factors.
Methods
We reviewed data on 853 patients with stage IV colorectal cancer who underwent elective palliative primary tumor resection between January 2006 and December 2007. To detect the hospital factors that could influence the prognosis of incurable colorectal cancer, the relationships between patient/hospital factors and overall survival were analyzed. Among hospital factors, hospital type (Group A: university hospital or cancer center; Group B: community hospital), hospital volume, and number of colorectal surgeons were examined.
Results
In univariate analysis, Group A hospitals showed significantly better prognosis than Group B hospitals (p = 0.034), while hospital volume and number of colorectal surgeons were not associated with overall survival. After adjustment for patient factors in multivariate analysis, hospital type was significantly associated with overall survival (hazard ratio: 1.31; 95 % confidence interval: 1.05–1.63; p = 0.016). However, there was no significant difference in short-term outcomes between hospital types.
Conclusions
Hospital type was identified as a hospital factor that possibly affects the prognosis of stage IV colorectal cancer patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Many reports have observed that hospital factors along with various patient and surgeon factors affect the short-term and long-term outcomes of patients undergoing surgery for colorectal cancer [1, 2]. Hospital volume is the best known example of a hospital factor [3, 4]. Patients with stage IV colorectal cancer need support from various medical professionals with diverse backgrounds and skills, including colorectal surgeons, medical oncologists, radiologists, and palliative care physicians. Accordingly, their prognosis is possibly influenced by many factors [5–8]. However, little is known regarding the hospital factors that may affect the prognosis of patients with incurable colorectal cancer. Therefore, in this study, we assessed certain hospital factors that potentially affected the prognosis of patients with stage IV colorectal cancer who underwent palliative primary tumor resection.
Materials and methods
Patients
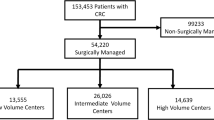
The Japan Society of Laparoscopic Colorectal Surgery (JSLCS) retrospectively collected data on 968 patients with stage IV colorectal cancer who underwent palliative tumor resection at 41 participating hospitals between January 2006 and December 2007. All surgeons were experienced in laparotomy, and most of them performed over 100 laparoscopic surgeries [9]. From the 968 patients, we excluded 37 patients who had active cancer in other organs, 5 patients with a performance status of 4, 51 patients who underwent emergency operation, and 23 patients who underwent insufficient lymph node dissection (D0 or D1). We included only patients undergoing D2 or D3 lymph node dissection. The scope of lymph node dissection was classified between D0 and D3 according to guidelines from the Japanese Society for Cancer of the Colon and Rectum [10]. D2 lymph node dissection indicates the removal of pericolic and intermediate lymph nodes, and D3 involves removal of pericolic, intermediate, and main lymph nodes around the root of the regional artery. Hepatic and peritoneum metastases were distinguished from distant metastasis according to Japanese classification [10]. Finally, 853 patients who underwent elective palliative tumor resection with sufficient scope of lymph node dissection were included in the analyses.
Hospital factors
This study included 41 hospitals that participated in the JSLCS study. We focused on three hospital factors, namely hospital type (university hospital, cancer center, or community hospital), hospital volume, and number of colorectal surgeons. In Japan, university hospitals and cancer centers play a leading role in cancer care, and we divided the hospitals into the following two groups according to the hospital type: (1) group A, which included university hospitals and cancer centers, and (2) group B, which included community hospitals. Hospital volume was defined as the average annual number of colorectal cancer patients who underwent surgery in each institution.
Statistical analysis
Continuous variables were compared by Student’s t test. Categorical valuables were compared by Fisher’s exact test. Survival analyses were performed with Kaplan-Meier estimates, and they were compared by the log-rank test. Multivariate analysis was performed using the Cox proportional hazards model. Overall survival (OS) was defined as the time between the date of primary tumor resection and the date of death. All p values were two-sided, and p values less than 0.05 were considered statistically significant. All statistical analyses were performed using JMP Statistical Software Version 11 (SAS-Institute Inc., Cary, NC).
Results
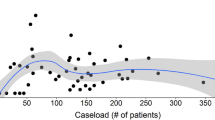
The clinicopathological characteristics of the 853 patients are shown in Table 1, and the characteristics of the 41 participating hospitals are described in Table 2. Groups A and B comprised 28 and 13 institutions, respectively, and the numbers of patients treated in each hospital group were 626 and 227, respectively. Hospital volume was classified into two categories of ≥200 and <200 operations/year, with 10 institutions (350 patients) and 31 institutions (503 patients) classified into the respective categories. The number of colorectal surgeons in each institute was divided into two categories of ≥5 and <5, with 20 institutions (396 patients) and 21 institutions (457 patients) classified into the respective categories.
Among patient factors, age, tumor depth, regional lymph node metastasis, hepatic metastasis, peritoneal metastasis, distant metastasis, tumor location, surgical approach, scope of lymph node dissection, preoperative intestinal stenosis, carcinoembryonic antigen (CEA), carbohydrate 19–9 (CA19-9), American Society of Anesthesiologists - Physical Status (ASA-PS) score, and postoperative chemotherapy were significantly associated with OS (Table 3). Among hospital factors, only hospital type was significantly associated with OS, and OS was significantly higher in the group A hospitals than in the group B hospitals (median survival time: 772 vs. 616 days, p = 0.034) (Fig. 1). The other hospital factors—hospital volume and number of colorectal surgeons—were not associated with OS (Table 4). In multivariate analysis, hospital type remained significantly associated with OS even after adjusting for patient factors (Table 5).

Overall survival of patients stratified by hospital type
Short-term outcomes after primary tumor resection were compared between the group A and B hospitals; these results are shown in Table 6. There were no significant differences between the two groups in terms of resumption of oral intake, length of postoperative hospital stay, conversion from laparoscopic to open surgery, intraoperative complications, or postoperative complications (National Cancer Institute Common Terminology Criteria for Adverse Events v3.0 ≥ grade 2).
Discussion
Outcomes of patients with colorectal cancer are believed to be influenced by hospital factors as well as tumor, patient, and surgeon factors [1, 2]. Many reports have described an effect of hospital volume on both short-term and long-term outcomes in patients with colorectal cancer [3, 4]. Recently, hospital type has been focused on as an influential factor in various disease groups, such as pediatric disease, urologic cancer, breast cancer, and hepatocellular carcinoma [11–14]. With respect to colorectal cancer, Elferink et al. [15] reported that different hospital types showed significant differences in treatment and long-term outcomes. The treatment of incurable stage IV colorectal cancer shows greater diversity than that of other, curable stages because these patients are treated with multimodality therapy, including medical oncology, radiology, and symptomatic palliative care [6]. Therefore, the survival of patients with stage IV colorectal cancer is expected to be highly influenced by hospital factors. However, little is known regarding the impact of hospital type on the prognosis of patients with stage IV colorectal cancer. In this study, we examined several hospital-related factors, and only hospital type was significantly associated with prognosis, while hospital volume and number of colorectal surgeons were not.
Regarding the reason for better OS in the group A hospitals than in the group B hospitals, we consider that the main difference is the number and variety of cancer specialists apart from surgeons. In Japan, university hospitals and cancer centers (group A hospitals) have many specialists from various fields who are actively involved in cancer care, as compared with community hospitals (group B), which have fewer cancer specialists. Specialized cancer care has been reported to improve outcomes in various cancers, including colorectal cancer, breast cancer, and ovarian cancer [16]. In particular, systemic chemotherapy has been reported to improve survival in patients with incurable colorectal cancer [17, 18], but there are considerable variations in the administration of chemotherapy across hospitals [19]. Japan has faced a chronic shortage of medical oncologists, similar to many other countries [20, 21]. In the present study period (2006–2007), more intensive and toxic chemotherapy, such as FOLFOX and FOLFORI, were introduced into clinical practice in Japan, leading to a greater need for medical oncologists specialized in colorectal cancer chemotherapy. In this study, postoperative chemotherapy significantly improved OS (p < 0.001), but there was no significant difference between group A and B hospitals in the proportion of patients who received postoperative chemotherapy (84.0 vs. 80.6 %, p = 0.174). Therefore, the management of chemotherapy by the oncologists might affect patients’ prognosis. An inhomogeneous distribution of such specialists across hospitals might contribute to the prognostic differences between group A and B hospitals.
Supportive care is also an essential factor in cancer care. Such care is reported to improve the patients’ condition and can help in continuing cancer therapy [7, 8]. Although it is difficult to assess the quality of supportive care, it has been reported that there might be large disparities between hospitals [22]. Higher quality supportive care in group A hospitals might improve the postoperative prognosis of patients with stage IV colorectal cancer who undergo palliative primary tumor resection.
On the other hand, we did not observe any differences between the hospital types in short-term outcomes, including postoperative complication rates and length of hospital stay, which are well-known indicators of the quality of curative colorectal surgery. A possible explanation for this finding is that our study only included hospitals with experienced specialists in colorectal surgery, and so the quality of surgery did not differ by hospital type. Further, in the management of patients with incurable colorectal cancer, the impact of the primary cancer surgery on patient survival might be relatively small compared with the impact of multimodality treatment [23, 24].
This study has some limitations, including its retrospective nature and a possible selection bias, although we made adjustments to minimize the effects of both surgeon factors and patient diversity. Therefore, it may be difficult to generalize our findings. Another limitation is that we lacked information on the patients’ comorbidities and details of postoperative therapies. These factors might influence patient outcomes, but we made best effort to minimize the effect of disease other than colorectal cancer by excluding the patients with insufficient lymph node dissection, which was often performed in patients with severe comorbidities. Despite these limitations, we believe that the results of this study help in resolving medical inequality across hospitals.
In conclusion, hospital type was identified as a significant prognostic factor for OS in patients with stage IV colorectal cancer undergoing palliative primary tumor resection.
References
Gort M, Otter R, Plukker JT, Broekhuis M, Klazinga NS (2010) Actionable indicators for short and long term outcomes in rectal cancer. Eur J Cancer 46:1808–1814
Zheng Z, Hanna N, Onukwugha E, Bikov KA, Mullins CD (2014) Hospital center effect for laparoscopic colectomy among elderly stage I-III colon cancer patients. Ann Surg 259:924–929
Wibe A, Eriksen MT, Syse A, Tretli S, Myrvold HE, Soreide O (2005) Effect of hospital caseload on long-term outcome after standardization of rectal cancer surgery at a national level. Br J Surg 92:217–224
Salz T, Sandler RS (2008) The effect of hospital and surgeon volume on outcomes for rectal cancer surgery. Clin Gastroenterol Hepatol 6:1185–1193
Mathis KL, Nelson H, Pemberton JH, Haddock MG, Gunderson LL (2008) Unresectable colorectal cancer can be cured with multimodality therapy. Ann Surg 248:592–598
Ronnekleiv-Kelly SM, Kennedy GD (2011) Management of stage IV rectal cancer: palliative options. World J Gastroenterol 17:835–847
Andersen C, Rorth M, Ejlertsen B, Stage M, Moller T, Midtgaard J et al (2013) The effects of a six-week supervised multimodal exercise intervention during chemotherapy on cancer-related fatigue. Eur J Oncol Nurs 17:331–339
Cheville AL, Kollasch J, Vandenberg J, Shen T, Grothey A, Gamble G et al (2013) A home-based exercise program to improve function, fatigue, and sleep quality in patients with Stage IV lung and colorectal cancer: a randomized controlled trial. J Pain Symptom Manag 45:811–821
Hida K, Hasegawa S, Kinjo Y, Yoshimura K, Inomata M, Ito M et al (2012) Open versus laparoscopic resection of primary tumor for incurable stage IV colorectal cancer: a large multicenter consecutive patients cohort study. Ann Surg 255:929–934
Watanabe T, Itabashi M, Shimada Y, Tanaka S, Ito Y, Ajioka Y et al (2012) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int J Clin Oncol 17:1–29
Jan S, Slap G, Smith-Whitley K, Dai D, Keren R, Rubin DM (2013) Association of hospital and provider types on sickle cell disease outcomes. Pediatrics 132:854–861
Gort M, Broekhuis M, Otter R, Klazinga NS (2007) Improvement of best practice in early breast cancer: actionable surgeon and hospital factors. Breast Cancer Res Treat 102:219–226
van der Geest LG, van Meer S, Schrier JG, Ijzermans JN, Klumpen HJ, van Erpecum KJ, et al. (2015) Survival in relation to hospital type after resection or sorafenib treatment for hepatocellular carcinoma in The Netherlands. Clin Res Hepatol Gastroenterol [Epub ahead of print]
Hicks CW, Wick EC, Canner JK, Black JH 3rd, Arhuidese I, Qazi U et al (2015) Hospital-level factors associated with mortality after endovascular and open abdominal aortic aneurysm repair. JAMA Surg 150:632–636
Elferink MA, Wouters MW, Krijnen P, Lemmens VE, Jansen-Landheer ML, van de Velde CJ et al (2010) Disparities in quality of care for colon cancer between hospitals in the Netherlands. Eur J Surg Oncol 36:S64–S73
Selby P, Gillis C, Haward R (1996) Benefits from specialised cancer care. Lancet 348:313–318
Costi R, Di Mauro D, Giordano P, Leonardi F, Veronesi L, Sarli L et al (2010) Impact of palliative chemotherapy and surgery on management of stage IV incurable colorectal cancer. Ann Surg Oncol 17:432–440
Platell C, Ng S, O’Bichere A, Tebbutt N (2011) Changing management and survival in patients with stage IV colorectal cancer. Dis Colon Rectum 54:214–219
McLeod A (1999) Variation in the provision of chemotherapy for colorectal cancer. J Epidemiol Community Health 53:775–781
Nakano T (2004) Status of Japanese radiation oncology. Radiat Med 22:17–19
de Azambuja E, Ameye L, Paesmans M, Zielinski CC, Piccart-Gebhart M, Preusser M (2014) The landscape of medical oncology in Europe by 2020. Ann Oncol 25:525–528
van Ryn M, Phelan SM, Arora NK, Haggstrom DA, Jackson GL, Zafar SY et al (2014) Patient-reported quality of supportive care among patients with colorectal cancer in the Veterans Affairs Health Care System. J Clin Oncol 32:809–815
Hu CY, Bailey CE, You YN, Skibber JM, Rodriguez-Bigas MA, Feig BW et al (2015) Time trend analysis of primary tumor resection for stage IV colorectal cancer: less surgery, improved survival. JAMA Surg 150:245–251
Stillwell AP, Buettner PG, Ho YH (2010) Meta-analysis of survival of patients with stage IV colorectal cancer managed with surgical resection versus chemotherapy alone. World J Surg 34:797–807
Acknowledgments
The authors completed this study in collaboration with the following in data collection: Seiichiro Yamamoto (National Cancer Center Hospital), Hiroya Kuroyanagi (Cancer Institute ARIAKE Hospital), Atsushi Ikeda (Kitasato University), Koki Otsuka (Iwate Medical University), Shungo Endo (Showa University Northern Yokohama Hospital), Masaaki Ito (National Cancer Hospital East), Michitoshi Goto (Juntendo University), Shuji Saito (Shizuoka Cancer Center), Akiyoshi Kanazawa (Osaka Red Cross Hospital), Tadashi Suda (St. Marianna University), Hisanaga Horie (Jichi Medical University), Yousuke Kinjo (Kyoto University), Yoshiro Kubo (Shikoku Cancer Center), Koichi Hanai (Fujita Health University), Hiroyuki Bando (Ishikawa Prefectural Central Hospital), Yosuke Fukunaga (Bell-land General Hospital), Yasuhiro Munakata (Nagano Municipal Hospital), Toshimasa Yatsuoka (Saitama Cancer Center), Takashi Yamaguchi (Kyoto Medical Center), Hirotoshi Hasegawa (Keio University), Hitoshi Idani and Kanyu Nakano (Fukuyama Municipal Hospital), Shoichi Fujii (Yokohama City University), Ichiro Takemasa (Osaka University), Toshiaki Watanabe (Teikyo University), Yoshihisa Saida (Toho University Ohashi Medical Center), Tomohisa Furuhata (Sapporo Medical University), Kunihiko Nagakari (Juntendo University Urayasu Hospital), Ichio Suzuka (Kagawa Prefectural Central Hospital), Shigeki Yamaguchi (Saitama Medical University), Yoshiaki Kuriu (Kyoto Prefectural University), Kohei Murata (Suita Municipal Hospital), Kiyoshi Maeda (Osaka City University), Takeshi Ueki (Kyusyu University), Masafumi Inomata (Oita University), Hiroshi Hirukawa (Tachikawa General Hospital), Takao Ichihara (Nishinomiya Municipal Central Hospital), Kazuya Okamoto (Fujinomiya City General Hospital), Takao Hinoi (Hiroshima University), and Katsuichi Matsuo (Fukuoka University).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights and informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Hoshino, N., Hasegawa, S., Hida, K. et al. Influence of hospital type on survival in stage IV colorectal cancer. Int J Colorectal Dis 31, 1443–1449 (2016). https://doi.org/10.1007/s00384-016-2611-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-016-2611-9