
Abstract
Purpose
Psychometric evaluation with tools such as the faecal incontinence quality of life scale is an essential component of clinical assessment. Currently, there is no translated Traditional Chinese version of the scale. A validated translated version may help to improve the quality of healthcare received in countries with Chinese minorities (0.5, 1.2 and 4.0 % of the UK, USA and Australian population, respectively) as well as local population of Hong Kong. The purpose of this study is to validate the Traditional Chinese version of the faecal incontinence quality of life scale (FIQL).
Methods
The FIQL questionnaire was translated into Traditional Chinese Language followed by linguistic validation. It was then tested on 55 patients with faecal incontinence and 93 controls in the colorectal outpatients clinic. Faecal incontinence severity index was also used for the assessment of disease severity.
Results
Internal consistency was good/excellent for all scales (Cronbach’s alpha >0.70, between 0.71 and 0.93). The intra-class correlation indicated a high stability over time with coefficients ranging between 0.78 and 0.90. Test and retest of all four scales found no significant differences of mean scores between baseline and retest. The mean faecal incontinence quality of life scale scores of all four domains improved significantly after treatment of 10 patients whose faecal incontinence severity index scores decreased by 50 % of their pre-treatment scores, hence indicating good sensitivity.
Conclusions
This study demonstrates the linguistic and psychometric validity of the traditional Chinese version of the faecal incontinence quality of life scale.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Faecal incontinence (FI) is defined as an involuntary loss of anal sphincter control resulting in an uncontrolled release of gas, liquid or solid stool [1]. The estimated prevalence of FI in the community is believed to be increasing with age and the female sex more likely to be suffering from it [2]. Aetiology such as obstetric trauma, previous anal surgery, rectal prolapse and elderly age are known to be associated with FI. The incidence of FI is thought to be under-reported, as sufferers may not seek medical help due to the embarrassing nature and the social stigma surrounding the disease.
Patients who seek help are initially assessed in specialised colorectal clinic where a detailed history and examination are carried out. The impact of FI on an individual should not only be measured by its severity but also on the quality of life of the individual. In general, the current recognised measurements on FI severity (Wexner’s score [3], St. Mark’s Incontinence scoring system [4] and the faecal incontinent severity index (FISI) [5]) focus the frequency of the loss of gas, liquid or solid stool, along with the impact on life style and use of medication. The measurement of quality of life can either be used with a generic scale, such as the Short-Form 36 Health Survey (SF-36) or a disease-specific quality of life measurement. Rockwood et al. initially developed the faecal incontinence quality of life scale (FIQL) in 2000 [6]. The instrument comprises of four domains (lifestyle, coping/behaviour, depression/self-perception and embarrassment) with a total of 29 items. This validated instrument was originally written in English but later translated into different languages (e.g. French [7], Norwegian [8], Italian [9], Japanese [10], Turkish [11] and Spanish [12]), with minor changes made to suit cultural diversities.
Hong Kong has a population of 7.18 million (94 % Chinese) with the majority of the population uses Cantonese as their spoken language and traditional Chinese characters as their written language. Traditional Chinese is also commonly used in Taiwan and Macau. Moreover, the Chinese community represent 0.5, 1.2 and 4.0 % of the UK, USA and Australian population, respectively. Therefore, a validated translated version of the FIQL may help to improve the quality of healthcare provided for local populations and ethnic minorities in Western countries. Translated version of the SF-36 is currently in use in Hong Kong [13]. However, as it is a generic scale, a more disease-specific scale such as a translated version of the FIQL will undoubtedly benefit FI patients in Hong Kong.
The aim of this study is to produce a validated Traditional Chinese version of the FIQL.
Method
Patients and measurements
The sample population consists of 55 patients with faecal incontinence and 93 controls with other gastrointestinal symptoms. Subjects were over 18 years of age, recruited among patients referred to the colorectal clinic at the Prince of Wales Hospital between the periods of January 2011 and January 2012.
FI patients and controls were asked to complete the translated version of the FIQL, FISI and the Chinese version of the SF-36 [13].
The FIQL comprises 29 items measuring four domains of health-related quality of life: lifestyle (10 items), coping/behaviour (9 items), depression/self-perception (7 items) and embarrassment (3 items). All items are rated on a scale from 1 to 4 points except two items in the depression/self-perception with ranges of 1 to 5 and 1 to 6 points. The score for each domain is the mean score of all the items within its domain.
The FISI is a 4-item scale to assess patient’s symptom severity by the frequency (2 or more times a day; once a day; 2 or more times a week; once a week; 1–3 times a month; never) to loss of gas, mucus, liquid or solid stool [5].
Several aspects of the translated questionnaire are tested. In order to avoid responder fatigue, some of the aspects are divided into subgroups for analysis.
This study was approved by the Local Survey and Behaviour Ethics Committee.
Linguistic validation of the translated FIQL
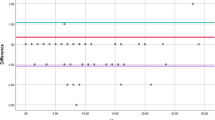
An independent translator translated the American version of the FIQL into a traditional Chinese version with Chinese as his mother tongue. The translated script was then inspected and confirmed by the authors (TWCM, WWL, DKYN). The questionnaire was then back-translated into American-English by a native independent translator with good command of the English language. The translated FIQL (Fig. 1) and FISI was then pilot tested on 10 patients (5 with FI and 5 controls) to verify that it is clear, understandable and acceptable (Fig. 2).

Traditional Chinese version of the faecal incontinence quality of life score

Linguistic validation of the translated FIQL
Psychometric properties
Reliability of the translated scale was established by measuring internal consistency and test-retest coefficients. The internal consistency of each domain was tested by means of Cronbach’s alpha coefficient. Scores were considered poor if <0.5, suspicious if between 0.5 and 0.69, acceptable if 0.7 and 0.8, good if 0.81 and 0.9 and excellent if >0.9 [14].
Test-retest aims to measure the temporal stability of the instrument. A subgroup of randomly selected FI patients was given the same questionnaire to complete at two time-points between 10 and 14 days without treatment. The second questionnaires were sent to the patients’ home with a stamped addressed envelope. This was examined by calculating the intra-class correlations (ICC) for each scale with the corresponding 95 % confidence interval. ICC > 0.8 was considered acceptable.
Validity of the questionnaire was assessed on its convergent and divergent validity. The convergent validity was analysed by evaluating the correlation between the four scales and the appropriate dimensions of the SF-36. Scores of 0 to 0.25 were deemed very poor, 0.26 to 0.49 were judged poor, 0.50 to 0.69 were judged average, 0.70 to 0.89 were deemed strong and 0.9 or higher were judged very strong. On analysing the divergent validity, four scales of the translated questionnaire were correlated to the FISI.
Statistical analysis
The analysis of the internal validity was performed by Cronbach’s alpha coefficients. The test-retest analysis was performed using the ICC. Analysis of validity of the translated FIQL with respect to the SF-36 and FISI was made using Pearson’s correlation coefficients. Statistical analysis was performed using SPSS version 20.0 (IBM SPSS statistics, Somers USA). A p value <0.05 was considered significant.
Results
Of the 148 patients, 55 patients were referred first time with symptoms of FI and 93 patients with other gastrointestinal symptoms without faecal incontinence as controls. The demographics of the patient population are listed in Table 1.
In this study, 84 % of the FI patients completed the questionnaire. Of the uncompleted questionnaires, those which were <80 % completed were discarded (2/150; 1.3 %). The remaining partially completed questionnaires (10/148, 6.8 %; 2/55, 3.6 % FI group and 8/93, other GI group) were completed using the mean score method for each corresponding domain. Frequently missing items were related to their sexual history (3 h; 33 % and 3 k; 28 %). There were no significant correlations among incomplete items.
There were also significant differences in FIQL scores of all domains between FI patients and controls, indicating that it is disease specific (Table 2).
Psychometric analysis
Reliability
The internal consistency of the translated FIQL in 79 patients evaluated using Cronbach’s alpha was found to range from acceptable to excellent in all four domains; 0.93 for lifestyle, 0.89 for coping/behaviour, 0.84 for depression/self-perception and 0.70 for embarrassment (Table 3).
A subgroup of 25 FI patients were randomly chosen for the test and retest study.
Intra-class correlation (ICC) for each scale was calculated which indicated high stability over time with coefficient; 0.94 for lifestyle, 0.95 for coping/behaviour, 0.88 for depression/self-perception and 0.78 for embarrassment (Table 3).
Convergent validity
The convergent validity of the questionnaire was analysed by evaluating the scales of the FIQL with the appropriate scales of the SF-36 (translated version). In total, 10 comparisons were examined and all were found to be statistically significant (Table 4). This confirms the validity of the translated questionnaire against the validated sensitivity of the SF-36.
To analyse the divergent validity, the scales of the FIQL were correlated with the FISI (translated version). Although all four domains were found to have negative correlations, only two of the four domains were found to be statistically significant (Table 5).
Responsiveness
The mean FIQL scores improved with statistical significance in all four domains after treatment of a pilot study carried out in our unit to investigate the efficacy of transcutaneous electric nerve stimulation on acupuncture points (Acu-Tens) on faecal incontinence where 8 out of 10 patients whose FISI scores decreased by 50 % from their pre-treatment scores, hence indicating good sensitivity (Table 6) [15].
Discussion
This present study demonstrates sufficient validity and reliability of the traditional Chinese version of the FIQL. Traditional Chinese characters are a written form of Chinese character set that does not contain the newly created characters, simplified Chinese characters, which were formed after 1946. Traditional Chinese characters are commonly in Taiwan, Hong Kong, Macau and many overseas Chinese ethnic communities in United Kingdom, Australia, USA and Canada. Hence, a validated translated traditional Chinese version of the FIQL may help to improve the quality of healthcare received in ethnic Chinese minorities in these countries.
The FIQL has been translated into many different languages for patient suffering from faecal incontinence in different countries. The size of the study population for revalidation in other studies varies from 50 patients (Portuguese version [16]), 76 patients (Norwegian version [8]) to 119 patients (Japanese version [17]). In this study, 55 patients with faecal incontinence were recruited which seemed to be sufficient for the study.
All of the patients were recruited from our outpatient colorectal clinics. Patients who agreed to participate completed their questionnaire in a quiet room with on-hand support if any questions arise. This method we believe allows a higher completion rate with a more accurate respond from the patient. However, for the reliability study, the retest questionnaires were sent to the patients’ address with a stamped address envelope. Although a 100 % return of these retest questionnaires were received, we were unable to know the time taken to complete the questionnaires and also to provide on-site assistance should queries arise.
We have found a significant proportion of unanswered questions related to sexual relations/behaviour, which were similar to the Norwegian study [8]. These questions are culturally sensitive and can be regarded as items that are ‘missing not at random’. Missing data are common in quality of life questionnaires. The personal mean score method to deal with missing data appears to be appropriate with insignificant bias [18].
Similar to the French [7], Norwegian [8] and Japanese [17] FIQL studies, the psychometric analysis of the FIQL indicated high internal consistency for three of the four scales with the lowest being the domain of embarrassment. Cronbach’s alpha has been known to be sensitive to the number of items, and this has been reflected in the value for the embarrassment domain, which has only three items. However, in this study, the Cronbach’s alpha value for embarrassment (0.70) still remains to be in the acceptable range.
The stability over time has shown to be good for this translated FIQL, with the intra-class correlations between 0.78 and 0.90 for all scales. The variability in results in other studies may be influenced by the time interval between the tests. Tsunoda et al. suggested that a shorter time interval may minimise the risk of changes in clinical status, which could therefore affect the quality of life score. We have chosen in this study for the time interval to be between 10 and 14 days without treatment, as used by Rockwood et al. in the original paper [6]. This time interval seemed to be a reasonable time frame as it has also been used in other studies [11, 12, 17].
In this study, we also correlated the FIQL with the FISI score. Negative correlations were found, indicating severity of the disease having a negative impact on the patient’s lifestyle, coping/behaviour, depression/self-perception and embarrassment. However, two of the four domains were not statistically significant, which may be due to type II error.
The correlations between the four scales of the traditional Chinese version and the scales of SF-36 were examined. We have selected 10 comparisons and found all of them to be statistically significant. This confirmation would allow this translated FIQL to be used in the assessment of outcomes in clinical trials.
In conclusion, this traditional Chinese version of the FIQL presents sufficient psychometric properties to be used in clinical and research settings for patients with faecal incontinence.
References
Barker A, Hurley J (2014) Novel treatment options for fecal incontinence. Clin in Colon Rectal Surg 27:116–20
Erekson EA, Ciarleglio MM, Hanissian PD et al (2014) Functional disability among older women with fecal incontinence. Am J of Obs and Gynae 327:e1–7, March
Jorge JM, Wexner SD (1993) Etiology and management of fecal incontinence. Dis Colon Rectum 36:77–97
Vaizey CJ, Carapeti E, Cahill JA, Kamm MA (1993) Prospective comparison of faecal incontinence grading systems. Gut 44:77–80
Rockwood TH, Church JM, Fleshman JW et al (1999) Patient and surgeon ranking of the severity of symptoms associated with fecal incontinence: the fecal incontinence severity index. Dis Colon Rectum 42:1525–32
Rockwood TH, Church JM, Fleshman JW et al (2000) Fecal Incontinence Quality of Life Scale: quality of life instrument for patients with fecal incontinence. Dis Colon Rectum 43:9–16
Rullier E, Zerbib F, Marrel A et al (2004) Validation of the French version of the Fecal Incontinence Quality-of-Life (FIQL) scale. Gastroenterol Clin Biol 28:562–8
Dehli T, Martinussen M, Mevik K et al (2011) Translation and validation of the Norwegian version of the fecal incontinence quality-of-life scale. Scand j surg : SJS : official organ for the Finnish Surgical Society and the Scandinavian Surgical Society 100:190–5
Altomare DF, Rinaldi M, Giardiello GG et al (2005) Italian translation and prospective validation of fecal incontinence quality of life (FIQL) index. Chir Ital 57:153–8
Ogata H, Mimura T, Hanazaki K (2012) Validation study of the Japanese version of the Faecal Incontinence Quality of Life Scale. Colorectal dis : the official journal of the Association of Coloproctology of Great Britain and Ireland 14:194–9
Dedeli O, Fadiloglu C, Bor S (2009) Validity and reliability of a Turkish version of the Fecal Incontinence Quality of Life Scale. J wound, ostomy, continence nurs : official publication of The Wound, Ostomy and Continence Nurses Society / WOCN 36:532–8
Minguez M, Garrigues V, Soria MJ et al (2006) Adaptation to Spanish language and validation of the fecal incontinence quality of life scale. Dis Colon Rectum 49:490–9
Lam CL, Tse EY, Gandek B, Fong DY (2005) The SF-36 summary scales were valid, reliable, and equivalent in a Chinese population. J Clin Epidemiol 58:815–22
Cronbach LJ (1951) Coefficient alpha and the internal structure of tests. Psychometrika 16:297–334
Mak TWC, Ngo DKY, Leung WW et al (2014) A pilot study to investigate the efficacy of transcutaneous electric nerve stimulation on acupoints (Acu-TENS) for the treatment of faecal incontinence. Colorectal dis : the official journal of the Association of Coloproctology of Great Britain and Ireland 16:204–8
Yusuf SA, Jorge JM, Habr-Gama A et al (2004) Evaluation of quality of life in anal incontinence: validation of the questionnaire FIQL (Fecal Incontinence Quality of Life). Arq Gastroenterol 41:202–8
Tsunoda A, Yamada K, Kano N, Takano M (2013) Translation and validation of the Japanese version of the fecal incontinence quality of life scale. Surg Today 43:1103–8
Peyre H, Leplege A, Coste J (2011) Missing data methods for dealing with missing items in quality of life questionnaires. A comparison by simulation of personal mean score, full information maximum likelihood, multiple imputation, and hot deck techniques applied to the SF-36 in the French 2003 decennial health survey. Qual life res : an international journal of quality of life aspects of treatment, care and rehabilitation 20:287–300
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Mak, T.W.C., Leung, W.W., Ngo, D.K.Y. et al. Translation and validation of the traditional Chinese version of the faecal incontinence quality of life scale. Int J Colorectal Dis 31, 445–450 (2016). https://doi.org/10.1007/s00384-015-2462-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-015-2462-9