
Abstract
Purpose
Historically, gastroschisis was considered a death sentence in Mozambique. The purpose of this study was to evaluate the current state of gastroschisis management and outcomes in our facility and to identify potential areas of improvement in neonatal and surgical care.
Methods
A retrospective study was performed of all gastroschisis patients admitted to Hospital Central Maputo located in Maputo City/ Mozambique from 2019 to 2020. Demographic, perinatal, operative, and mortality data were obtained from neonatal and surgical logbooks. Descriptive analysis was performed.
Results
A total of 62 gastroschisis patients were admitted to the Hospital Central Maputo. No patients had a prenatal diagnosis. Many of the infants were born preterm (48%), and 68% had low birth weight. Only 15 (24%) patients underwent operative intervention (73% primary fascial closure and 27% sutured silo). There were only three survivors (5%) all of whom underwent primary closure. However, the overall survival rate for patients undergoing an attempt at surgical closure was 20%.
Conclusion
While the mortality rate remains high for gastroschisis patients in Mozambique, there have been a few survivors when surgery is performed. Improvements in neonatal care are needed. Given the high mortality rates and limited resources, we plan to focus our surgical efforts on bedside closure techniques.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Gastroschisis has been described as a bellwether for evaluating neonatal capacity [1]. Mortality rates for gastroschisis range from < 5% to > 95% depending on local resources and expertise [2, 3]. The high levels of mortality from gastroschisis in low- and middle- income countries (LMIC) have been attributed to sepsis and prematurity [4, 5].
Until recently, gastroschisis was considered a death sentence for newborns in Mozambique. Starting in 2019, we initiated strategies to improve perinatal care and attempt abdominal wall closure with the goal of achieving patient survival. The purpose of this study was to evaluate the current state of gastroschisis management and outcomes in our facility and to identify potential areas of improvement in neonatal and surgical care.
Methods
Study design and setting
A retrospective study for the period of January 1st, 2019, to 31st December 2020 was performed in the neonatal unit of Hospital Central Maputo (HCM).
This unit until January 2021 was the only neonatal unit for all country of about 30 million people. Hospital Central Maputo is the largest and referral hospital in Mozambique, takes care of population from all country principally from Maputo city and the provinces of Gaza, Inhambane, and Maputo. This hospital has 1512 beds, approximately and covers a population of 3,089,773 inhabitants.
The study was approved by the Institutional Review Board of the Faculty of Medicine at Hospital Central Maputo CIBS FM & HCM/ P078-2021).
Study population
All cases of gastroschisis who were admitted and registered at neonatal unit logbook of HCM during 2019 to 2021 were included in the study. The excluded cases were those gastroschisis patients who died outside hospital before admission or other abdominal malformations that are not gastroschisis or gastroschisis cases who survive and were readmitted with other complications or disease.
Data collection and data analysis
A qualitative assessment of the HCM neonatal unit and emergency operating room facilities was performed by evaluating the physical campus and the patient management protocols.
An estimate was made for the number of gastroschisis patients that would be expected during the time period based on total population, birth rate, and rate of gastroschisis birth defect.
Patient data were obtained from a secure spreadsheet containing all registered neonatal admissions as well as a logbook of emergency operative cases. Demographic and perinatal data were collected including location/province of birth, mode of delivery, gestational age, birthweight, comorbidities, type of surgical intervention (if performed), and outcome. Location of birth was classified into one of five categories: Hospital Central Maputo, other hospital in Maputo city, other hospital outside Maputo city, delivery outside of a hospital, and unspecified. Mode of delivery was categorized as vaginal or Cesarean section. Gestational age was categorized as preterm (< 37 weeks estimated gestational age) or term (> 37 weeks). Birthweight was categorized as low birth weight if less than 2500 g and normal birth weight if more than 2500 g.
All gastroschisis cases were managed in the neonatal unit of Hospital Central Maputo, and all surgical procedures were performed by pediatric surgeons from this hospital. All surgical operative reports were reviewed, and surgery management variables collected were age of the baby during the intervention (< 24 h, 24 to 48 h, or > 48 h) and type of intervention (primary closure or sutured silo). The outcome (survival or death) and others associated causes that contributed to death were also identified. Descriptive analysis was performed.
Results
The Hospital Central de Maputo neonatal unit
Hospital Central de Maputo was the only neonatal unit for the entire country until 2021, that performed surgery for gastroschisis. The neonatal unit has capacity for 78 patients and is staffed by 4 neonatologists (only 1 with specialized training in neonatal intensive care), 1 pediatrician, and 3 general doctors. The neonatal unit volume is approximately 2900 admissions per year. The unit is usually full, and it is common for 2 to 3 children to share an incubator. The unit also lacks essential equipment, consumables, and specific medications for neonatology (e.g., ventilator, parenteral nutrition, silo, machine to deliver gas anesthetics). It does not have a neonatal intensive care unit (NICU) or operating room facilities.
All newborn patients requiring surgery are transferred to a separate building for emergency operations. The emergency operating rooms are utilized by all surgical providers, and wait times are commonly greater than 12 to 24 h. Transport is usually performed by an attendant outdoors without an incubator or ambulance. In addition, there are no safeguards like warming blankets to prevent hypothermia.
Estimate of gastroschisis births
The estimated rate of gastroschisis births based on a Mozambique population of 30.8 million [6], birth rate of 37/1000 [6] and gastroschisis rate (1/3000 births)[6] is 345 per year. For the period 2019 to 2020, we would estimate 690 gastroschisis births in Mozambique.
Demographics of infants with gastroschisis (Table 1)
A total of 62 gastroschisis cases presented to the Maputo Central Hospital neonatal unit over the 2-year study period January 1, 2019 to December 31, 2020. Most infants were transferred in from outside facilities (82%). No patients had a prenatal diagnosis of gastroschisis. Vaginal delivery was performed for most patients (n = 49, 79%). Many of the infants were born preterm (n = 30, 48%) and 68% had low birth weight (See Table 1).
Surgical treatment (Table 2)
Of the 62 infants with gastroschisis, only 15 (24%) underwent surgery. However, the percentage of patients undergoing surgery went down from 9 in 2019 to 6 in 2020. Primary closure was utilized in 11 of the 15 patients who underwent surgery (73%). A sutured silo (using material from a sterile urine bag) was utilized to provide temporary closure in four patients (27%) whose viscera-abdominal disproportion prohibited primary closure.
Outcomes
Overall, 59 (95%) of gastroschisis cases died (Table 3). Of the 59 deaths, the most common attributed cause of death was sepsis (64%) followed by prematurity (17%). Other causes of death included small for gestational age, multiple malformations, and respiratory distress syndrome.
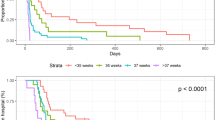
The mortality rate for the 15 patients who underwent an operation was 80% (Table 4). The majority of patients (83%) died within 1 week of the operation. Death was attributed to sepsis (82%) and prematurity (17%). All patients who underwent temporary closure with sutured silo failed to survive to final abdominal closure. Of the 11 patients who successfully underwent abdominal wall closure, the presumed cause of death for the eight who did not survive was sepsis (7/11—63%) and prematurity (1/11—9%). We are unable to determine if prolonged ileus, malnutrition, and/or lack of parenteral nutrition contributed to the death of these patients.
The three patients who survived (5%) underwent primary closure of the abdominal wall defect. These three patients represent a survival rate of 20% for those who underwent any surgical intervention and 27% for those who underwent successful primary closure. The patients who survived were all transferred in from nearby hospitals and underwent surgery within 24 to 48 h of birth. Only one of the three patients who survived was preterm and less than 2500 g in weight. All had uncomplicated gastroschisis and were initially managed with a vented orogastric tube, intravenous fluid therapy, and antibiotics. None of the three survivors required mechanical ventilation (which is not available at our facility for neonates). The herniated bowel was covered with a plastic bag and positioned to minimize mesenteric angulation to avoid intestinal ischemia. Post-operatively, the orogastric tube was left in place and vented to the air. When the column of fluid from the vented tube lowered, feeds were initiated around the 7 to 10 days after surgery. Feedings were administered via the orogastric tube slowly via a syringe pump and advanced as tolerated. The full feeds were achieved around 21 days after surgery. The median time to discharge following surgery was 25 days.
Discussion
In this report, we described our first successful experiences with the management of gastroschisis. While the overall mortality rate for this condition was high (95%), we only attempted closure in 24% of the patients. For those who underwent an attempt at surgical closure, a 20% (3/15) survival rate was noted. Given this early experience, we have been very careful with patient selection given the limited operative and neonatal resources at our facility (especially during the COVID pandemic in 2020).
As in other low- and middle- income countries, we attribute our high mortality rate to deficient prenatal and neonatal care [7]. Prenatal ultrasonography, diagnosis, and monitoring is not available. Not surprisingly, 82% of patients were born outside our institution and transferred to our neonatal unit. Delays in diagnosis, management, and transfer can lead to desiccation/ischemia/edema of the intestines, under-resuscitation, hypothermia, and sepsis [1, 8]. Furthermore, nearly half of the infants in our series were premature and the majority had low birth weight. Our neonatal unit lacks parenteral nutrition, mechanical ventilators, and other components of neonatal intensive care which are helpful in the management of premature and low birth weight infants unable to tolerate enteral feedings [8, 9]. However, we have successfully utilized orogastric tubes to vent the stomach and initiate early enteral feeding. This strategy was adopted from colleagues in Malawi (Eric Borgstein), who utilize the column of gastric contents in the tube to determine the timing for initiation of feedings. Specifically, an open syringe is attached to a feeding tube and situated above the patient. This allows for back pressure of gastric contents, decreases vomiting, and minimizes gastric losses. Once the column of gastric contents lowers, breast milk is added to the syringe with continuous drip to allow for gravity feeding. Daily rectal irrigations with saline are also utilized to stimulate bowel function. From a sepsis standpoint, we have a crowded neonatal unit with many infants sharing incubators limiting best practices for infection control and likely contributing to sepsis.
Another challenge in the management of gastroschisis at our institution is the lack of pre-formed silos with silastic rings to help facilitate bowel coverage and enable gradual reduction of bowel contents. Consequently, we attempt primary closure in the emergency operating rooms, which are in a separate building. This requires that the newborn is transported outdoors (unmonitored) further contributing to the risk of dehydration, hypothermia, and sepsis. If primary closure cannot be achieved, a sutured silo closure is performed using a piece of a urinary drainage bag. However, there have been no patients with silo closure survive to final abdominal wall closure. Management of patients with silo is complicated by challenges with wound care, lack of antibiotics, and difficulty coordinating reductions and return to the OR. Therefore, we have been very selective in those in whom we attempt abdominal wall closure.
Most deaths after surgery occurred within 1 week of the operation suggesting that sepsis and/or other neonatal factors (and not malnutrition) contributed to their death. We have no experience with a bedside skin closure technique (9) and hope that the addition of this approach could help avoid the need for operative intervention, increase the percentage of patients who undergo abdominal wall closure, and improve survival. Unfortunately, we do not have pre-formed silos, which can be a helpful tool to facilitate reduction of bowel when using this and other techniques.
On a broader scale, we should mention that we admitted less than 10% of the estimated 690 gastroschisis births in Mozambique for this 2-year time period. Therefore, there is a need to offer either prenatal diagnosis or expand neonatal capacity to other referral hospitals in the country to improve outcomes for patients with gastroschisis.
Limitations
The study was conducted in Hospital Central de Maputo, therefore, results could not be generalizable to all country.
Another limitation of this study is that it is a retrospective study and the hospital does not have electronic health records. Data were collected from a neonatal unit logbook, emergency surgery logbook, and patient charts (with limited accessibility from a medical records department).
Apart from 2019, the study collected data from the first year of the Covid19-pandemic 2020, and gastroschisis management maybe not reflect the reality during 2020 because of the measures implemented in the country to reduce the spread of the infection and health care reference hospital policies.
Conclusion
Gastroschisis is no longer a death sentence in Mozambique. While our mortality rate remains high, we have been able to achieve a 20% survival rate in those who undergo an attempt at surgical closure. Prenatal, neonatal and operative capacity remains limited. Orogastric-tube feeding protocols could help increase the chance of survival until parenteral nutrition becomes available for neonates at our institution. Bedside skin closure techniques that avoid the need for transport to another building to carry out operative closure could increase the number of patients that achieve abdominal wall closure and survive. Ultimately, pre-formed silos would be extremely helpful in the management of patients with gastroschisis.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Ford K, Poenaru D, Moulot O, Tavener K,l. et al (2016) Gastroschisis: Bellwether for neonatal surgery capacity in low resource settings? J Pediatr Surg [Internet]. 51(8):1262–1267
Abdul-Mumin A, Cotache-Condor C, Owusu SA, Grimm A, Mahama H, Wright N et al (2021) A retrospective review of gastroschisis epidemiology and referral patterns in northern Ghana. Pediatr Surg Int 37:1069–1078
Wright NJ, Leather AJM, Ade-Ajayi N, Sevdalis N, Davies J, Poenaru D et al (2021) Mortality from gastrointestinal congenital anomalies at 264 hospitals in 74 low-income, middle-income, and high-income countries: a multicentre, international, prospective cohort study. The Lancet 398(10297):325–339
Shalaby A, Obeida A, Khairy D, Bahaaeldin K (2020) Assessment of gastroschisis risk factors in Egypt. J Pediatr Surg [Internet]. 55(2):292–295
Raymond SL, Hawkins RB, Peter SD, Downard CD, Qureshi FG, Renaud E et al (2020) Predicting Morbidity and Mortality in Neonates Born With Gastroschisis. J Surg Res 245:217–224
Anuário Estatístco Statistical Yearbook 2017 Moçambique [Internet]. 2018. Available from: www.ine.gov.mz
Wesonga AS, Fitzgerald TN, Kabuye R, Kirunda S, Langer M, Kakembo N et al (2016) Gastroschisis in Uganda: opportunities for improved survival. J Pediatr Surg 51(11):1772–1777
Nitzsche K, Fitze G, Rüdiger M, Birdir C (2020) Prenatal prediction of outcome by fetal gastroschisis in a tertiary referral center. Diagnostics 10(8):540
DeUgarte DA, Calkins KL, Guner Y et al (2020) Adherence to and outcomes of a University-consortium gastroschisis pathway. J Pediatr Surg [Internet]. 55(1):45–48
Funding
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject discussed in the manuscript.
Author information
Authors and Affiliations
Contributions
All the authors read and approved the final manuscript. VA: reviewed the literature, contributed to the conception and design of the work, supervised and took part in the data acquisition, conducted the data analysis, drafted the interpretation of the results, wrote the first full draft of the manuscript, and integrated the comments of the co-authors. DADeU: contributed to the conception and design of the work, supervision and took part in the data analysis and interpretation of the results and engaged in the manuscript writing. ID: took part in the data acquisition and substantively commented on the manuscript. MF: took part in the data analysis and interpretation of the results, and substantively commented on the manuscript involved.
Corresponding author
Ethics declarations
Conflict of interest
None reported.
Ethics approval and consent to participate
The study was approved by the Mozambique Institutional Bioethics Committee of the Faculty of Medicine and Maputo Central Hospital (CIBS FM &HCM/ P078-2021). The study was conducted according to the guidelines of the Declaration of Helsinki. The informed consent of all participants was obtained.
Consent for publication
Not applicable.
Informed consent
This study was conducted following the principles of the Declaration of Helsinki. All methods were carried out following relevant regulations and guidelines. This study was approved by the Mozambique Institutional Bioethics Committee of the Faculty of Medicine and Maputo Central Hospital (CIBS FM &HCM/ P078-2021).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Amado, V., Dias, I., Filipe, M. et al. Gastroschisis in Mozambique: current status and priorities for improving care from Hospital Central de Maputo, the largest and referral hospital of the country. Pediatr Surg Int 39, 95 (2023). https://doi.org/10.1007/s00383-023-05376-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s00383-023-05376-3