
Abstract
Purpose
Recurrent chordee (RC) is an important complication of proximal hypospadias repair. In this meta-analysis we compared RC incidence following dorsal plication (DP) versus ventral lengthening (VL).
Methods
We searched the databases to identify all papers between 2001 and 2021 pertaining to proximal hypospadias and recurrent chordee. Duplicate publications, review articles and incomplete articles were excluded. Meta-analysis of heterogeneity was reported with I2 statistics. The pooled outcomes were compared to Chi square/Fishers exact test.
Results
A total of 17 articles were included covering 582 patients. The I2 statistics for prevalence of RC among different publications showed no heterogeneity for DP (I2 = 0%) and low heterogeneity for VL (I2 = 26%). RC was noticed in 31/122 (25.4%; 95% CI 18%–33%) among patients who had DP alone while it was significantly lower, 24/460 (5.3%; 95% CI 4%–8%) when VL was used (p = 0.0001). When compared to DP, all VL techniques had significantly lower incidence of RC. Among the VL techniques lowest incidence of RC was found for ventral corporotomies (4%) followed by small-intestinal- submucosa (SIS 4.2%) and tunica vaginalis flap (TVF)/free graft-TVFG (5%). Among the VL subtypes: the proportion of RC with use of TVF (4/70, 5.7%) and TVFG (3/69, 4.3%) for corporoplasty was comparable (p = 1); single-layer SIS was associated with significantly less RC (1/90, 1.1%) than 4-layer SIS (5/51, 9.8%; p = 0.02).
Conclusion
For correction of severe ventral chordee during primary proximal hypospadias repair, dorsal plication carries a higher risk of recurrence compared to ventral lengthening procedures.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Adequate correction of ventral chordee (VC) is essential during primary repair of proximal hypospadias. While several surgeons omit the important step of artificial erection test to objectively assess the chordee and its correction during primary repair, naked eye estimation is often prone to mistakes[1]. Late occurrence of recurrent chordee (RC) during adolescence has been reported by several authors [2, 3] causing cosmetic disfigurement and painful erections. Inadequate and inappropriate correction of VC during primary procedure is an important cause of RC [4]. Vandersteen and Husmann [5] felt that a successful artificial erection induced at hypospadias surgery may not prevent RC which may occur late due to skin tethering, ventral fibrosis or corporeal disproportion and extensive urethral fibrosis.
There are multiple methods to correct VC during primary proximal hypospadias repair. While dorsal plication (DP) techniques may be applied for VC less than 30 degree [2], the urge to correct proximal hypospadias in one stage may make the surgeon underestimate the degree of chordee and choose DP and urethral plate preservation techniques[6] even in severe cases. Several ventral lengthening (VL) methods like ventral fairy cuts (corporotomy), ventral corporal excision/grafting (corporoplasty) have been used with or without urethral plate preservation [7, 8] for correction of VC more than 30 degree. In this systematic review and meta-analysis we have compared the contemporary outcomes of VC correction techniques during primary proximal hypospadias repair in preventing RC.
Methods
Search strategy
A systematic literature review of publications in English of the following electronic databases was conducted: Cochrane Database, PUBMED, MEDLINE and EMBASE. The following keywords were used: (proximal) AND (hypospadias) AND (chordee OR curvature) AND (recurrence OR complications). The publication date range for studies was from January 2001 to September 2021. Two researchers independently screened articles for the review.
Inclusion and exclusion criteria
We defined study eligibility using the population, intervention, comparator, outcome, and study design approach (PICOS). Population (P) was children with proximal hypospadias which included proximal penile, penoscrotal or perineal opening after degloving of the penis (hypospadias with severe chordee, in whom VC persisted after complete degloving/ventral skin detethering). Articles published before twenty years from present were not included as we were only interested in the contemporary outcomes in the new millennium.
Interventions (I) were chordee correction techniques along with proximal hypospadias. Only articles that mentioned chordee identification and correction technique were included. They included DP technique alone, which may be a midline plication (Baskin) or lateral plication (Nesbit) along with single stage repair; or VL techniques which may be ventral corporotomies, ventral fairy cuts, deep transverse incision of tunica albugenia (DTITA), ventral corporal excisions followed by bridging of the corporal defect (corporoplasty) with tunica vaginalis flap (TVF), tunica vaginalis free graft (TVGF), dermal/dural graft (DF), or small-intestinal submucosa (SIS). Papers not providing clear details of type of hypospadias, type of urethroplasty or VC correction technique were excluded [3, 6,7,8]. Isolated case reports, small case series (< 5), those which included distal hypospadias also [9, 10], and review articles without original data were excluded.
Comparator I was between DP and VL techniques of chordee correction. Outcomes (O) analyzed was RC during follow-up after primary proximal hypospadias repair. RC was either diagnosed by the surgeon during outpatient follow-up/during the second procedure or complained by the patient/parent during the follow-up. Papers which did not provide the follow-up duration or incidence of RC in the complication were excluded. Papers focusing on RC management alone could not be used in the meta-analysis on RC incidence without a denominator.
Study appraisal and synthesis
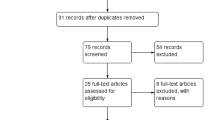
Study design (S) followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) criteria [11]. Study selection was performed through two levels of screening. In the first level, abstracts were reviewed for the inclusion and exclusion criteria. In the second level screening, all articles filtered through the first level were read in their entirety and the same inclusion and exclusion criteria applied. Figure 1 describes the methodology followed in this systematic review and meta-analysis.

PRISMA flow chart depicting study selection and inclusion
Risk of bias analysis
Risk of bias (ROB) analysis was performed for each article by two authors separately and vetted using robvis tool [12] before inclusion in the meta-analysis. Six factors were assessed. Clarity of study population (pediatric), type of hypospadias (proximal), details on incidence of RC and duration of follow-up were expected to be essential and have low ROB. Urethroplasty technique and VC correction technique were considered important and was expected to have low or medium ROB. Following ROB analysis four papers [13,14,15,16] which combined both VL and DP techniques were considered to have high overall ROB and were excluded.
Data analysis
Meta-analysis of proportions was carried out using MetaXL 5.3 (Epigear International © 2010–2016). Heterogeneity was reported with I2 statistics, with 0–25% not important, 25–50% moderate, 50–75% substantial, and 75–100% considerable. Forest plot was constructed to compare the pooled prevalence of complications in different VC correction methods used to treat proximal hypospadias. Statistical analysis comparing proportions was performed with Chi square test or Fisher’s test when the values were small. The difference was considered statistically significant if the p value was < 0.05.
Results
Study selection
Figure 1 shows the study selection process. Among 69 articles identified on screening, 16 articles were excluded as they were duplicates or editorials or commentaries without data. Due to inadequate data on primary repair/RC incidence 12 articles were excluded. Further 12 articles with errors, 3 review articles and 5 small case series (less than five patients) were excluded. After leaving further 4 articles due to overlapping VC correction techniques (ROB), a total of 17 articles [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] were included in this meta-analysis. All the studies reported children who typically underwent primary hypospadias repair between 9–18 months of age. All articles mentioned intra operative artificial erection test to assess VC & RC. Four articles [34,35,36,37] reporting only late RC and its management were excluded but were discussed separately as they did provide some useful information. The authors were from across the globe from many countries, as shown by the geographical origin of the included articles: USA, UK, Canada, Egypt, Japan and Turkey.
Risk of bias (ROB) analysis
Figure 2 shows the traffic light plot representing ROB of each article considered in the study. Four papers had high ROB as they described both DP & VL and were not included in the meta-analysis. In two studies with medium ROB [17, 20] only details regarding DP were considered; as the remaining patients had a combination of procedures to correct chordee. All the remaining included articles had an acceptable overall ROB.

Risk of bias (ROB) analysis. Four articles with high overall ROB (two techniques VL and DP combined) were not included in the meta-analysis. Among two articles with medium ROB (VL or DP but described separately) data describing either one technique clearly was derived
Meta-analysis
Figure 3 shows the forest plot for all included publications. The I2 statistics for prevalence of RC among different publications showed no heterogeneity for DP (I2 = 0%) and low heterogeneity for VL (I2 = 26%). Publication bias studied with DOI plot showed Luis Furuya-Kanamori (LFK) index of 0.26 for DP and 0.69 for VL suggesting no asymmetry among papers making a good case for pooled meta-analysis with fixed effects model.

Forest plot comparing DP and VL techniques. Squares represent % of RC and horizontal line, the 95% confidence interval. The heterogeneity was low in both groups
The pooled data from 17 articles covered a total of 582 patients with proximal hypospadias and severe VC. Table 1 describes the type of urethroplasty, primary VC correction technique and incidence of RC. The follow-up duration ranged from 12–120 months. Among all the included patients RC was reported in 55/582 patients which amounted to 9.4% (95% CI 7%–12%).
Comparison of RC incidence between DP and VL techniques
Table 2 summarizes the pooled outcomes of VC correction techniques. Among patients who had DP alone as primary technique 31/122 had RC with an incidence of 25.4% (95% CI 18%–33%). Among patients who had VL as primary technique 24/460 had RC with an incidence of 5.3% (95% CI 4%–8%). VL techniques were associated with a significantly lower incidence of RC (p = 0.0001) compared to DP.
Comparison of different VL technique
Among the VL techniques lowest incidence of RC (Table 2) was found for ventral corporotomies (4%) followed by SIS (4.2%) and TVF/TVFG (5%). Dermal/dural graft had 10.9% incidence of RC. When compared to DP, all VL techniques had significantly lower incidence of RC (p < 0.00001 for ventral corporotomy/TVF/TVFG/SIS; p = 0.028 for dermal/dural graft) but there was no significant difference within VL techniques.
Comparison of VL subtypes
The proportion of RC with use of TVF (4/70, 5.7%) and TVFG (3/69, 4.3%) for corporoplasty was comparable with no statistically significant difference (p = 1). Although overall RC with SIS was comparable with other VL techniques, within SIS subgroup: single-layer SIS was associated with significantly less RC (1/90, 1.1%) than 4-layer SIS (5/51, 9.8%; p = 0.02).
Etiology and management of RC
Although RC management is not the aim of this meta-analysis, we felt the four excluded publications [34,35,36,37] on RC management may be worth reporting separately (Table 3). Among 170 patients with RC, 100 (59%) were following DP and 33 (19%) were following VL. In 74 (43%) the type of primary VC correction technique was unclear. Skin scarring and ventral subcutanenous fibrosis were reported to be cause of RC in 73 (43%) of patients. In 54 (31%) of patients skin detethering ± DP was performed to correct RC. Corporal disproportion was reported in 42/56 (75%) in one study [35] which recommended staged repair with ventral corporotomies to treat RC.
Discussion
Ventral chordee is an important aspect to be addressed during proximal hypospadias repair. Skin detethering alone released VC in 19%, while in 31% it persisted but less than 30 degree and in 50% it was more than 30 degree [1]. The incidence of RC varies from 0 – 30% depending on the length of follow-up and the method of assessment [17, 25]. Several authors [2, 38, 39] have felt that poor intra operative assessment of VC and post-operative documentation of RC are responsible for under reporting of this particularly devastating complication. It is easy to underestimate lesser degrees of bending, as up to 30 degree of curvature can be easily mistaken to be inconspicuous on visual inspection [35]. While failure to perform artificial erection or objectively assess chordee using a goniometer during primary repair is an important reason to miss VC, inadequate/inappropriate correction of VC is an equally important cause. A survey [40] of pediatric urologists regarding VC correction reported that DP was their preferred management in those up to 40 degree of chordee.
DP was initially described by Nesbit on lateral aspects of corpora and was further modified by Baskin to include only midline 12 O’ clock plication to safe guard nerves. In this meta-analysis we found that when DP was used to correct chordee in primary proximal hypospadias, it was associated with 25% incidence of RC and this was five times more than that found with VL procedures (5.3%). Braga[25] in a multivariate analysis also reported high odds (OR 4.5) of developing RC following DP compared to VL.
There are several VL procedures to correct severe chordee associated with proximal hypospadias. VL procedures like fairy cuts on corpora (corporotomy) and wide excision of corpora with grafting (corporoplasty) have gained popularity over the years for severe VC [18,19,20, 28]. In this meta-analysis we found that all VL procedures had significantly reduced incidence of RC. Among the various VL procedures, transverse ventral corporotomies had the lowest incidence (4%) of recurrent chordee while dermal/dural grafts had the highest (10.9%). While using tunica vaginalis for corporoplasty, it may be used as a vascularised flap (TVF) or as a free graft (TVFG). We found no difference in outcome between either TVF or TVFG, thereby supporting the use of the simpler TVFG which is easier to harvest and carries less risk of complications like twist, testicular ascent and acquired chordee/torsion known with TVF. Similarly, we also found that 4-layer SIS had higher risk of RC, probably due to fibrosis and graft contracture [24].
Despite adequate correction (confirmed by repeating artificial erection test) of VC during primary repair, RC is known to develop around adolescence in a proportion of patients [33, 34, 36]. While most papers included in this meta-analysis reported a follow-up of 5–10 years, adolescent outcomes were hardly reported. Husmann [41] raised concerns regarding possibility of erectile dysfunction in patients undergoing urethral plate division or VL procedures. In the present meta-analysis, we have not looked at the incidence of erectile dysfunction following these penile straightening procedures, because it was not reported by many authors. Future research should focus on whether this can be reduced by choosing one VL procedure over the other.
One of the important limitations of this study is variation in urethroplasty techniques. Some authors performed urethral plate elevation[17] and ventral incisions along with a single stage repair and we had to exclude those numbers. Some added DP to this step to prevent ventral shortening again [13,14,15,16] and we had to exclude them as well. Some papers on VL reported both single stage urethroplasty and staged procedure [21, 23, 29] following urethral plate division. Thus the surgeon’s preference over hypospadias correction technique was highly subjective and prone to bias. Despite these limitations, as we excluded papers with high ROB we had pure data on either DP alone or VL alone to compare RC rates.
Documentation of finer details at primary procedure and strict follow-up up to adulthood is the only way to gain more knowledge on this subject over the years. While some authors have mentioned that penile length is shorter in hypospadiac children [42] others have reported it to be normal [43]. Special attention to assess penile length, both dorsally and ventrally before and after surgery, could help assess this important patient centric aspect. Hayashi [23] felt 15% VC was insignificant, while in a survey by Bologna [40] up to 20% chordee was considered insignificant. Bologna [40] reported that VL was opted only for chordee above 50% while Schlomer [44] recommended VL for chordee above 45%. This approach has changed of late and now more surgeons are opting for VL for chordee above 30 – 40% [19, 26]. Hypospadiologists should introspect whether they are under-estimating the degree of VC and overdoing DP in an overzealous attempt at a single stage procedure. In this regard the authors support artificial erection test and objective measurement of VC with a goniometer before taking the major decision on the type of VC correction technique during primary hypospadias repair.
Conclusions
For correction of ventral chordee during primary proximal hypospadias repair, dorsal plication carries a higher risk of recurrence compared to ventral lengthening procedures. It is essential to objectively measure the extent of chordee and choose the ideal VC correction technique based on the best available evidence.
References
Snodgrass W, Prieto J (2009) Straightening ventral curvature while preserving the urethral plate in proximal hypospadias repair. J Urol 182:1720–1725. https://doi.org/10.1016/j.juro.2009.02.084
Moscardi PRM, Gosalbez R, Castellan MA (2017) Management of high-grade penile curvature associated with hypospadias in children. Front Pediatr. https://doi.org/10.3389/fped.2017.00189
Lam PON, Greenfield SP, Williot P (2005) 2-Stage repair in infancy for severe hypospadias with chordee: long-term results after puberty. J Urol 174:1567–1572. https://doi.org/10.1097/01.ju.0000179395.99944.48
Huang L-Q, Ge Z, Ma G (2020) Commentary: recurrent chordee in 59 adolescents and young adults following childhood hypospadias repair. J Pediatr Urol 16:521–522. https://doi.org/10.1016/j.jpurol.2020.06.005
Vandersteen DR, Husmann DA (1998) Late onset recurrent penile chordee after successful correction at hypospadias repair. J Urol 160:1131–1133. https://doi.org/10.1016/S0022-5347(01)62716-2
Pfistermüller KLM, Manoharan S, Desai D, Cuckow PM (2017) Two-stage hypospadias repair with a free graft for severe primary and revision hypospadias: a single surgeon’s experience with long-term follow-up. J Pediatr Urol 13:35.e1-35.e7. https://doi.org/10.1016/j.jpurol.2016.08.014
Long CJ, Chu DI, Tenney RW et al (2017) Intermediate-term followup of proximal hypospadias repair reveals high complication rate. J Urol 197:852–858. https://doi.org/10.1016/j.juro.2016.11.054
McNamara ER, Schaeffer AJ, Logvinenko T et al (2015) Management of proximal hypospadias with 2-stage repair: 20-year experience. J Urol 194:1080–1085. https://doi.org/10.1016/j.juro.2015.04.105
Chertin B, Koulikov D, Fridmans A, Farkas A (2004) Dorsal tunica albuginea plication to correct congenital and acquired penile curvature: a long-term follow-up. BJU Int 93:379–381. https://doi.org/10.1111/j.1464-410x.2003.04621.x
Yosef YB, Binyamini J, Matzkin H, Ben-Chaim J (2004) Midline dorsal plication technique for penile curvature repair. J Urol 172:1368–1369. https://doi.org/10.1097/01.ju.0000138341.68365.b6
Liberati A, Altman DG, Tetzlaff J et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700–b2700. https://doi.org/10.1136/bmj.b2700
McGuinness LA, Higgins JPT (2021) Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods 12:55–61. https://doi.org/10.1002/jrsm.1411
Al-Adl AM, Abdel Aal AM, El-Karamany TM, Noureldin YA (2020) Two-stage repair of proximal hypospadias with moderate to severe chordee using inner preputial skin graft: prospective evaluation of functional and cosmetic outcomes. World J Urol 38:2873–2879. https://doi.org/10.1007/s00345-020-03075-5
Tiryaki S, Ələkbərova V, Dokumcu Z et al (2016) Unexpected outcome of a modification of Bracka repair for proximal hypospadias: high incidence of diverticula with flaps. J Pediatr Urol 12:395.e1-395.e6. https://doi.org/10.1016/j.jpurol.2016.04.046
Springer A, Subramaniam R (2012) Split dorsal dartos flap transposed ventrally as a bed for preputial skin graft in primary staged hypospadias repair. Urology 79:939–942. https://doi.org/10.1016/j.urology.2012.01.006
Rynja SP, de Jong TPVM, Bosch JLHR, de Kort LMO (2018) Proximal hypospadias treated with a transverse preputial island tube: long-term functional, sexual, and cosmetic outcomes. BJU Int 122:463–471. https://doi.org/10.1111/bju.14234
Snodgrass W, Bush N (2021) Recurrent ventral curvature after proximal TIP hypospadias repair. J Pediatr Urol 17:222.e1-222.e5. https://doi.org/10.1016/j.jpurol.2020.11.030
Badawy H, Dawood W, Soliman AS et al (2020) Staged repair of proximal hypospadias: reporting outcome of staged tubularized autograft repair (STAG). J Pediatr Surg 55:2710–2716. https://doi.org/10.1016/j.jpedsurg.2020.07.023
Snodgrass W, Bush N (2017) Staged tubularized autograft repair for primary proximal hypospadias with 30-degree or greater ventral curvature. J Urol 198:680–686. https://doi.org/10.1016/j.juro.2017.04.019
Pippi Salle JL, Sayed S, Salle A et al (2016) Proximal hypospadias: a persistent challenge. Single institution outcome analysis of three surgical techniques over a 10-year period. J Pediatr Urol 12:28.e1-28.e7. https://doi.org/10.1016/j.jpurol.2015.06.011
Miguel C, Rafael G, Joshi D et al (2011) Ventral corporal body grafting for correcting severe penile curvature associated with single or two-stage hypospadias repair. J Pediatr Urol 7:289–293. https://doi.org/10.1016/j.jpurol.2011.03.008
Hayn MH, Bellinger MF, Schneck FX (2009) Small intestine submucosa as a corporal body graft in the repair of severe chordee. Urology 73:277–279. https://doi.org/10.1016/j.urology.2008.08.489
Hayashi Y, Kojima Y, Mizuno K et al (2010) Demonstration of postoperative effectiveness in ventral lengthening using a tunica vaginalis flap for severe penile curvature with hypospadias. Urology 76:101–106. https://doi.org/10.1016/j.urology.2009.08.080
Leslie JA, Cain MP, Kaefer M et al (2008) Corporeal grafting for severe hypospadias: a single institution experience with 3 techniques. J Urol 180:1749–1752. https://doi.org/10.1016/j.juro.2008.03.091
Braga LHP, Lorenzo AJ, Bägli DJ et al (2008) Ventral penile lengthening versus dorsal plication for severe ventral curvature in children with proximal hypospadias. J Urol 180:1743–1748. https://doi.org/10.1016/j.juro.2008.03.087
Badawy H, Morsi H (2008) Long-term followup of dermal grafts for repair of severe penile curvature. J Urol 180:1842–1845. https://doi.org/10.1016/j.juro.2008.04.082
Elmore JM, Kirsch AJ, Scherz HC, Smith EA (2007) Small intestinal submucosa for corporeal body grafting in severe hypospadias requiring division of the urethral plate. J Urol 178:1698–1701. https://doi.org/10.1016/j.juro.2007.05.090
Braga LHP, Pippi Salle JL, Dave S et al (2007) Outcome analysis of severe chordee correction using tunica vaginalis as a flap in boys with proximal hypospadias. J Urol 178:1693–1697. https://doi.org/10.1016/j.juro.2007.03.166
Kajbafzadeh A-M, Arshadi H, Payabvash S et al (2007) Proximal hypospadias with severe chordee: single stage repair using corporeal tunica vaginalis free graft. J Urol 178:1036–1042. https://doi.org/10.1016/j.juro.2007.05.062
Weiser AC, Franco I, Herz DB et al (2003) Single layered small intestinal submucosa in the repair of severe chordee and complicated hypospadias. J Urol 170:1593–1595. https://doi.org/10.1097/01.ju.0000083863.01634.e1
Soergel TM, Cain MP, Kaefer M et al (2003) Complications of small intestinal submucosa for corporal body grafting for proximal hypospadias. J Urol 170:1577–1579. https://doi.org/10.1097/01.ju.0000083802.87337.af
Ritchey ML, Ribbeck M (2003) Successful use of tunica vaginalis grafts for treatment of severe penile chordee in children. J Urol 170:1574–1576. https://doi.org/10.1097/01.ju.0000083694.44384.39
Gershbaum MD, Stock JA, Hanna MK (2002) A case for 2-stage repair of perineoscrotal hypospadias with severe chordee. J Urol 168:1727–1728. https://doi.org/10.1097/01.ju.0000027276.83141.8b (discussion 1729)
Abosena W, Talab SS, Hanna MK (2020) Recurrent chordee in 59 adolescents and young adults following childhood hypospadias repair. J Pediatr Urol 16:162.e1-162.e5. https://doi.org/10.1016/j.jpurol.2019.11.013
Snodgrass W, Bush NC (2019) Persistent or recurrent ventral curvature after failed proximal hypospadias repair. J Pediatr Urol 15:344.e1-344.e6. https://doi.org/10.1016/j.jpurol.2019.03.028
Howe AS, Hanna MK (2017) Management of 220 adolescents and adults with complications of hypospadias repair during childhood. Asian J Urol 4:14–17. https://doi.org/10.1016/j.ajur.2016.09.010
Yucel S, Sanli A, Kukul E et al (2006) Midline dorsal plication to repair recurrent chordee at reoperation for hypospadias surgery complication. J Urol 175:699–703. https://doi.org/10.1016/S0022-5347(05)00186-2
Pfistermuller KLMLM, McArdle AJJ, Cuckow PMM (2015) Meta-analysis of complication rates of the tubularized incised plate (TIP) repair. J Pediatr Urol 11:54–59. https://doi.org/10.1016/j.jpurol.2014.12.006
Babu R, Chandrasekharam VVS (2021) Meta-analysis comparing the outcomes of single stage (foreskin pedicled tube) versus two stage (foreskin free graft and foreskin pedicled flap) repair for proximal hypospadias in the last decade. J Pediatr Urol. https://doi.org/10.1016/j.jpurol.2021.05.014
Bologna RA, Noah TA, Nasrallah PF, McMahon DR (1999) Chordee: varied opinions and treatments as documented in a survey of the American academy of pediatrics, section of urology. Urology 53:608–612. https://doi.org/10.1016/S0090-4295(98)00656-6
Husmann DA (2021) Erectile dysfunction in patients undergoing multiple attempts at hypospadias repair: etiologies and concerns. J Pediatr Urol 17:166.e1-166.e7. https://doi.org/10.1016/j.jpurol.2020.12.002
Moriya K, Nakamura M, Nishimura Y et al (2016) Factors affecting post-pubertal penile size in patients with hypospadias. World J Urol 34:1317–1321. https://doi.org/10.1007/s00345-016-1763-0
Fievet L, Harper L, Chirpaz E et al (2012) Penile length is comparable in boys with and without hypospadias. J Pediatr Urol 8:493–496. https://doi.org/10.1016/j.jpurol.2011.10.006
Schlomer BJ (2017) Correction of residual ventral penile curvature after division of the urethral plate in the first stage of a 2-stage proximal hypospadias repair. Curr Urol Rep 18:13. https://doi.org/10.1007/s11934-017-0659-x
Funding
Nil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Nil.
Ethical approval
IRB exempted.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Babu, R., Chandrasekharam, V.V.S. A meta-analysis comparing dorsal plication and ventral lengthening for chordee correction during primary proximal hypospadias repair. Pediatr Surg Int 38, 389–398 (2022). https://doi.org/10.1007/s00383-022-05065-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-022-05065-7