
Abstract
Purpose
Hirschsprung’s disease-related short bowel syndrome (HDSBS) is characterized by aganglionosis that extends orally to 75 cm from Treitz’s band. The condition is reported be associated with a high mortality rate of 50–80%. This retrospective study aimed to survey the current trends in HDSBS treatment in Japan.
Methods
Patient data were extracted from the results of a nationwide survey we conducted, resulting in the retrospective collection of the data of 1087 HD patients from 2008 to 2012 in Japan.
Results
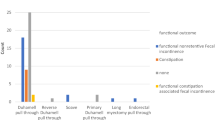
A total of 11 (0.9%) cases of HDSBS were noted. All patients underwent jejunostomy as neonates. Radical procedures performed in five patients (A-colon patch method in four, Duhamel’s procedure in one). Ziegler’s myotomy-myectomy and serial transverse enteroplasty (STEP) were performed in each patient as palliative procedures. No radical operations were performed in 4 of the 11 cases. The mortality rate was 36.4%. Four patients died, 1 patient who underwent STEP and 3 patients who received no radical procedures. The causes of death were sepsis due to enterocolitis or central intravenous catheter infection, and hepatic failure. All patients who underwent radical procedures survived and showed satisfactory outcomes.
Conclusion
HDSBS still showed a high mortality rate, although surgical approaches such as the A-colon patch method resulted in satisfactory outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recently, the treatment of Hirschsprung’ disease (HD) has improved and satisfactory outcomes can be achieved in many cases. However, the management of total colon aganglionosis, especially that with small bowel involvement, remains difficult, and the outcomes are not necessarily satisfactory [1,2,3]. In our report [4], Hirschsprung’s disease-related short bowel syndrome (HDSBS), a condition characterized by aganglionosis extending orally to 75 cm from Treitz’s band, was associated with a high mortality rate of 50–80% in Japan. HDSBS differs from standard SBS due to the lack of a colon, and the outcome of HDSBS patients is worse than that of standard SBS patients. This retrospective study aimed to clarify the current outcomes of HDSBS based on the results of a nationwide survey in Japan.
Patients and methods
This retrospective study was performed according to the Ethical Guideline for Clinical Research published by the Ministry of Health, Labour and Welfare of Japan on July 30, 2003 (revised 2008) and complied with the 1964 Declaration of Helsinki (revised in 2008). The study was approved by the clinical research ethics committee of Kyushu University Hospital (No. 27-273 and 28-155). All subjects gave their informed consent prior to their inclusion in this study.
From 2008 to 2012, we sent questionnaires to 156 pediatric surgery departments at major universities and hospitals throughout Japan. The questionnaires were designed to collect data on the general demographics of patients with HD, as well as their diagnosis, treatment, and outcomes [1]. We received responses concerning 1,087 patients with HD from 156 medical institutions, including 11 (0.9%) patients with HDSBS. We surveyed the general features, surgical management, and outcomes of the 11 patients with HDSBS.
Results
General features
The estimated incidence of HDSBS, which was based on the annual number of cases divided by the annual number of newborns from the annual report provided by the Ministry of Health and Welfare, Japan, was 1/456,412, and the male-to-female ratio was 2.7:1 (Table 1). Patients with a family history of HD accounted for 18.2% of the HDSBS population (Table 1). The incidence of associated anomalies was estimated to be 27.3% (Table 1). Down syndrome was not found among these patients.
Enterostomy
All patients underwent jejunostomy as neonates (Table 2). The average age at the time of jejunostomy was 5 days (median: 2 days).
Radical procedure
Radical procedures were performed in 5 of the 11 HDSBS cases. Among these, 4 underwent procedures using the ascending colon patch method, and one underwent Duhamel’s procedure extending to the sigmoid colon. Two of the 11 cases underwent extended myotomy–myectomy (Ziegler’s procedure; n = 1) and serial transverse enteroplasty (STEP; n = 1) as a palliative radical procedure. The remaining 4 patients did not undergo any radical procedures because it was contraindicated by their condition. Redo operations were performed in three patients (myotomy, n = 2; Ziegler’s procedure, n = 1) (Table 2).
Results of treatment
The mortality rate was 36.4%. Four of the 11 patients with HDSBS died, including 3 patients who did not undergo any radical procedures and 1 who underwent STEP (Table 3). The causes of death were sepsis (n = 3) due to enterocolitis or central intravenous catheter infection, and hepatic failure (n = 2) after long-term parenteral nutrition. All five patients who underwent radical procedures survived and showed satisfactory outcomes.
Discussions
According to our findings, HDSBS is a rare variant type of HD. The sex ratio of patients with HDSBS was the same as in a previous report [1]. Among the patients with HDSBS, 18.2% had a family history and the incidence of associated anomalies was 27.3%, which was higher in comparison to the overall HD population [1]; however, none of our patients had Down syndrome.
All patients underwent enterostomy in the neonatal period, which meant that the diagnosis of total aganglionosis with small bowel involvement was difficult to differentiate from congenital hypoganglionosis, immaturity of ganglia, or intestinal atresia.
Standard SBS most often results from a neonatal insult, such as necrotizing enterocolitis, complicated gastroschisis, intestinal atresia, or midgut volvulus. Although SBS is associated with a high mortality rate of up to 37.5% in the first 5 years of life [5], patients with standard SBS often retain their colon [5], which may be why they have an impressive potential for gut adaptation and independence from parenteral nutrition. In contrast, patients with HDSBS often lack a colon, so they may have difficulty achieving gut adaptation, continue to experience diarrhea and malnutrition, and sometimes suffer changes in the gut microbial flora and develop bacterial translocation.
As a definitive operation, many different procedures have been performed for total aganglionosis with small bowel involvement. In our previous report [4], the Martin procedure was the most common surgery; however, the mortality rate was relatively high at 8–12%. On the other hand, the mortality rate among cases in which ascending colon patch procedures are used is low. In our findings, 4 of 11 patients with HDSBS underwent ascending colon patch procedures with satisfactory outcomes. Amerstorfer et al. [6] stated that this procedure has two potential advantage: the preservation of the right colon as an isoperistaltic onlay with its water and electrolyte absorptive capacity as a reservoir between the right colon and ileum, and the preservation of the ileo-cecal valve as a natural barrier to prevent backwash, thereby reducing the incidence of enteritis and associated malabsorption.
Our previous report [1] noted a decrease in the mortality rate for patients with HD, whereas the mortality rate of patients with aganglionosis extending orally to more than 30 cm of the terminal ileum remained high. Importantly, our report showed that HDSBS is still associated with a high mortality rate. In comparison to the results of previous reports [1,2,3,4], the mortality rate of patients with HDSBS decreased from 60 to 80–36.4%. Developments in pediatric nutritional support, the diagnosis and treatment, and the selection of ideal radical operations for HDSBS patients may have played roles in the recent decrease in the mortality rate [2, 7]. However, sepsis was the most frequent cause of death, followed by hepatic failure due to long-term parenteral nutrition. HDSBS patients with hepatic failure may be good candidates for small intestine or multivisceral transplantation [8, 9]. Surgical intestinal lengthening procedures, such as STEP and small intestine or multivisceral transplantation, are considered novel therapies for the management of SBS in children [10]. In addition, in recent years, regenerative medicine (stem cell therapy) and tissue engineering have also been considered as treatments for HD [11, 12].
In conclusion, HDSBS still showed a relatively high mortality rate of 36.4%, although surgical approaches such as the ascending colon patch method resulted in satisfactory outcomes. The further development and indications of new treatment strategies for HDSBS, such as small intestine transplantation and regenerative medicine, are yet called for.
References
Taguchi T, Obata S, Ieiri S (2017) Current status of Hirschsprung’s disease: based on a nationwide survey of Japan. Pediatric Surg Int 33(4):497–504. https://doi.org/10.1007/s00383-016-4054-3
Hukkinen M, Koivusalo A, Merras-Salmio L, Rintala RJ, Pakarinen MP (2015) Postoperative outcome and survival in relation to small intestinal involvement of total colonic aganglionosis. J Pediatric Surg 50(11):1859–1864. https://doi.org/10.1016/j.jpedsurg.2015.05.017
Ruttenstock E, Puri P (2009) A meta-analysis of clinical outcome in patients with total intestinal aganglionosis. Pediatric Surg Int 25(10):833–839. https://doi.org/10.1007/s00383-009-2439-2
Ieiri S, Suita S, Nakatsuji T, Akiyoshi J, Taguchi T (2008) Total colonic aganglionosis with or without small bowel involvement: a 30-year retrospective nationwide survey in Japan. J Pediatric Surg 43(12):2226–2230. https://doi.org/10.1016/j.jpedsurg.2008.08.049
Wales PW, de Silva N, Kim JH, Lecce L, Sandhu A, Moore AM (2005) Neonatal short bowel syndrome: a cohort study. J Pediatric Surg 40(5):755–762. https://doi.org/10.1016/j.jpedsurg.2005.01.037
Amerstorfer EE, Fasching G, Till H, Huber-Zeyringer A, Höllwarth ME (2015) Long-term results of total colonic agangliosis patients treated by preservation of the aganglionic right hemicolon and the ileo-cecal valve. Pediatric Surg Int 31(8):773–780. https://doi.org/10.1007/s00383-015-3743-7
Pakarinen MP, Kurvinen A, Koivusalo AI, Ruuska T, Mäkisalo H, Jalanko H, Rintala RJ (2013) Surgical treatment and outcomes of severe pediatric intestinal motility disorders requiring parenteral nutrition. J Pediatric Surg 48(2):333–338. https://doi.org/10.1016/j.jpedsurg.2012.11.010
Ueno T, Wada M, Hoshino K, Sakamoto S, Furukawa H, Fukuzawa M (2013) A national survey of patients with intestinal motility disorders who are potential candidates for intestinal transplantation in Japan. Transpl Proc 45(5):2029–2031. https://doi.org/10.1016/j.transproceed.2013.01.092
Bond GJ, Reyes JD (2004) Intestinal transplantation for total/near-total aganglionosis and intestinal pseudo-obstruction. Semin Pediatric Surg 13(4):286–292. https://doi.org/10.1053/j.sempedsurg.2004.10.016
Schwartz MZ (2013) Novel therapies for the management of short bowel syndrome in children. Pediatric Surg Int 29(10):967–974. https://doi.org/10.1007/s00383-013-3404-7
Doğan SM, Kılınç S, Kebapçı E, Tuğmen C, Gürkan A, Baran M, Kurtulmuş Y, Ölmez M, Karaca C (2014) Mesenchymal stem cell therapy in patients with small bowel transplantation: single center experience. World J Gastroenterol WJG 20(25):8215–8220. https://doi.org/10.3748/wjg.v20.i25.8215
El-Nachef W, Grikscheit T (2014) Enteric nervous system cell replacement therapy for hirschsprung disease: beyond tissue-engineered intestine. Eur J Pediatric Surg 24 (03):214–218. https://doi.org/10.1055/s-0034-1376311
Acknowledgements
The authors wish to thank all the doctors in the 156 pediatric surgery departments at major universities and hospitals throughout Japan for replying to the questionnaires. This study was supported by a grant from The Ministry of Health, Labour and Welfare of Japan (Health and Labour Sciences Research Grants for Research on Intractable Diseases (H26-045)). The authors also thank Brian Quinn for his comments and help with the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All subjects gave their informed consent prior to their inclusion in this study. This retrospective study was also approved by the clinical research ethics committee of Kyushu University Hospital (No. 27-273 and 28-155).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The Japanese Study Group for Hirshsprung’s disease: Satoshi Obata, Satoshi Ieiri, Takashi Akiyama, Naoto Urushihara, Hisayoshi Kawahara, Masayuki Kubota, Miyuki Kono, Yuji Nirasawa, Shohei Honda, Masaki Nio, Tomoaki Taguchi.
Rights and permissions
About this article

Cite this article
Obata, S., Ieiri, S., Akiyama, T. et al. Nationwide survey of outcome in patients with extensive aganglionosis in Japan. Pediatr Surg Int 35, 547–550 (2019). https://doi.org/10.1007/s00383-019-04462-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-019-04462-9