
Abstract
Background
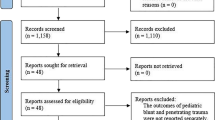
Many pediatric trauma patients are initially evaluated at non-pediatric, non-trauma centers where they undergo CT prior to transfer to a pediatric trauma center. The purpose of this study is to quantify the number of repeat CT and assess the risk of delayed or missed injuries.
Methods
The institutional pediatric trauma registry was queried for patients evaluated from January 2001 to March 2012. All patients who underwent repeat CT within 24 h after transfer were included. General admission, demographic, and outcome data were analyzed.
Results
A total of 6041 patients were transferred from a referring hospital after undergoing CT scans. Five percent of patients underwent repeat CT with a mean age of 6.3 ± 5.7 years. Patients who underwent repeat CT scans had significantly higher Injury Severity Scores and lower Glasgow Coma Scale. CT head was the most commonly repeated. Comparing results of referring CT scans to repeated scans, there was good agreement between results for head CT (κ = 0.69) and moderate agreement for abdominopelvic CT (κ = 0.59). The overall incidence of delayed diagnosis of injuries was 0.7 %.
Conclusion
The low incidence of missed or delayed injuries justifies limiting additional radiation exposure to pediatric trauma patients based on clinical status.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Computed tomography (CT) is a commonly used modality to assess injury in the pediatric trauma patient. An estimated 5–9 million CT examinations are performed annually on children in the United States, with the annual growth of CT use in adults and children approximated at 10 % per year [1]. CT evaluation for trauma continues to increase due to its efficacy as a diagnostic tool, the speed at which it can be performed, and its ability to provide high quality images [2].
The widespread use of CT scans has raised concern with regards to radiation exposure in the pediatric population and the possible risk of future malignancy. Organ doses from CT scans are up to 150–250 times larger than those of corresponding conventional radiography [3]. Children are at even greater risk than adults for a given dose of radiation as their organ tissues are up to ten times more radiosensitive, and they have a longer lifespan for radiation-induced cancer to develop [4].
Pediatric trauma patients are often initially evaluated at non-pediatric, non-trauma centers where they undergo CT prior to transfer to a pediatric trauma center. Many of these patients subsequently undergo duplicate scans after transfer. However, reports on the number of repeated scans after transfer to a trauma center are inconsistent. One study reported duplicate CT scans were performed in 91 % of transferred pediatric trauma patients [5], while another reported that on average 17.9 % of all CT scans were repeated after transfer to the pediatric trauma center [6]. The purpose of this study is to quantify the number of repeat CT scans performed and the resultant incidence of delayed diagnosis or missed injuries in patients transferred to a pediatric trauma center dedicated to minimizing radiation exposure to patients.
Materials and methods
After Institutional Review Board approval (IRB #12-0490), the All Children’s Hospital Johns Hopkins Medicine pediatric trauma registry was queried for all patients evaluated from January 2001 through March 2012. All trauma patients who underwent CT scans at referring hospitals prior to transfer were included. Patients who underwent repeat CT of the head, chest, and/or abdomen and pelvis within 24 h after transfer were further analyzed. General admission, demographic, and outcome data were studied. This included age, Injury Severity Score (ISS) and Glasgow Coma Scale (GCS) obtained from the initial evaluation at our institution, mechanism of injury, hospital distance, transfer CT results, number of repeated scans per body area, and time from emergency department arrival to repeated CT scan. The strength of agreement between the results of referring hospital CT scans and repeat CT scans was also analyzed. The results of referring hospital CT scans were based on the initial radiology interpretation from the referring institution. With regards to interpretation and comparison of results between referring hospital and repeat CT scans, agreement was based on the mutual absence or presence of findings. Results did not have to match exactly in terms of minor detail.
Over the last decade, several quality improvement measures have been incorporated into the care of the trauma patient with the goal of reducing the number of CT scans performed. This was a gradual process that took place over several years as we instituted several efforts to reduce the use of CT scans overall at our institution. Successful implementation of the modalities used to reduce the number of scans performed centered on a multidisciplinary approach involving members of multiple clinical services and administrative personnel. Some of the modalities used to limit the number of repeated scans at our institution include: radiologists who are committed to reviewing transferred scans and who are trained on multiple software platforms, use of web-based systems that push digital images directly to our institution, and use of couriers for obtaining outside CT scans when they are not transported with the patient. Our radiologists are not blinded to the referring institutions CT scan interpretation when they review transferred scans. During the daytime hours, an attending pediatric radiologist is available to interpret transferred scans. During the night time hours, CT scans are read by an outside service with many of these scans again reviewed the following day by our attending pediatric radiologist for final interpretations. When requested, radiologists formally report the interpretation of the outside CT scan and this is included as part of the patient’s medical record.
Data analysis was performed by a trained statistician. Demographic and clinical characteristics are summarized as counts (percentages) for categorical variables and mean [with standard deviation (SD)] or median (range) for continuous variables. Comparisons between repeated and non-repeated CT scan groups were performed using χ 2 test or Fisher’s exact test for categorical variables and Student’s t tests or Wilcoxon–Mann–Whitney test for continuous variables. Kappa (κ) statistics with corresponding 95 % confidence interval (CI) were used to evaluate the strength of agreement between the CT results of referring hospital scans to those that were repeated. Statistical analyses were performed using SAS 9.3 and all statistical tests were two-sided with the threshold for significance set at p ≤ 0.05.
Results
During the study period, a total of 8658 patients were transferred to our pediatric trauma center. Of these, 6041 patients underwent CT scan at a referring hospital prior to transfer. Repeat CT scans following transfer were performed in 288 patients (5 %). The mean age of patients who underwent repeat CT scans was significantly lower (6.3 versus 7.2, p < 0.01) compared to patients who did not undergo repeat CT. Patients who underwent repeat CT were found to have significantly higher Injury Severity Scores (12.2 versus 8.7, p < 0.01) and significantly lower Glasgow Coma Scale (13 versus 14, p < 0.01) compared to patients who did not undergo repeat CT (Table 1).
Hospital distance from the referring hospital to our trauma center was compared for patients who underwent repeat CT scans and to patients who did not undergo a duplicate CT. Mean hospital distance was 49.2 ± 36 miles for patients who did not undergo repeat CT scans, compared to 69 ± 40.6 miles for patients who underwent repeat CT scans (p < 0.01). Mechanism of injury was also analyzed for patients who underwent repeat CT scans. Patients who underwent duplicate scans were significantly more likely to present after motorized trauma, penetrating injuries, or assault compared to patients who did not undergo repeat CT. Repeated scans were less likely to be performed after lower impact traumas such as falls, non-motorized trauma, or sports related injuries (Fig. 1).

Mechanism of injury comparison between transferred pediatric trauma patients who did not undergo repeat CT scan to patients who underwent repeat CT scan
When evaluating the number of CT scans repeated per body region, it was noted that CT head was the most commonly repeated at 20 %, followed by abdominopelvic CT at 10 %, and chest CT at 4 % (Fig. 2). The mean time to repeat head CT was 238 ± 284 min (median 112, range 2–1318), mean time to repeat chest CT was 335 ± 415 min (median 134, range 15–1430), and mean time to repeat abdominopelvic CT was 162 ± 221 min (median 38, range 15–556) (Table 2).

Number of scans repeated per body area
The results of the referring facility CT scans were then compared to those that were repeated to determine the agreement of outcomes between the two results. We observed a good agreement (κ = 0.69, 95 % CI 0.58–0.8) between referring hospital results and repeated scan results for head CT scans. A moderate agreement (κ = 0.59, 95 % CI 0.35–0.83) between referring hospital results and repeated scan results was observed for abdominopelvic CT scans. There were too few CT chest scans that were repeated to perform any statistical analysis (Fig. 3).

Measurement of agreement between referring facility CT scan results compared to repeat CT scan results after transfer
Of the 6041 patients transferred to our pediatric trauma center after undergoing CT scan at a referring hospital, 42 patients were found to have missed injuries resulting in an overall incidence of missed or delayed diagnosis of 0.7 % over the 11 year study period. The mean age for this cohort was 9.5 ± 5.2 (0.2–17) years, mean ISS was 15.7 ± 10 (1–41) and mean GCS was 12 ± 5 (3–15). Of the 42 patients with missed injuries, 15 (36 %) had undergone repeat CT scan. This includes the 13 false negative scans that were found to be positive on repeat imaging as illustrated in Fig. 3. Of the remaining two patients who underwent repeat CT, one was found to have an orthopedic injury on extremity plain film (extremity fracture). The second was a maxillofacial injury (mandibular condylar fracture) which was read as positive by our radiologist interpretation of the referring facility imaging and not on the repeat head CT. Table 1 describes in detail the type of missed injury by body region and how the injuries were detected. There was one death in the missed injury cohort secondary to a closed head injury and respiratory failure following a motor vehicle collision trauma. However, the missed injuries noted in this patient were orthopedic extremity injuries and likely did not contribute to the mortality.
When evaluating the number of repeated CT scans performed per year, there has been a decreasing trend, with less than 4 % of scans repeated per year over the last 4 years (Fig. 4a). We appreciate this decrease in number of scans repeated, as we have maximized our radiation reducing measures. When evaluating the number of missed injuries per year, there was no increase in the number of missed injuries with the observed decrease in the number of repeat CT scans performed. There were no incidences of missed injuries over the last 3 years (Fig. 4b).

A Percent of repeated CT scans per year from 2001 to 2012. b Percent of missed injuries per year from 2001 to 2012
Discussion
In this large single institutional study of trauma patients, we observed that 5 % of CT scans were repeated after transfer. The literature has reported a wide range of repeated scans with 18–91 % of CT scans repeated after transfer to a trauma center [4–7]. The reasons or indications for repeated CT scans commonly reported include: images not transferred with the patient, technical difficulties in reviewing films, images are inadequate, incomplete, or of poor quality, changes in clinical condition, further evaluation of injuries identified on outside scans, or physician preference [4]. Following such practice results in increased radiation exposure to patients, increased cost, and increased risk of contrast nephropathy. The opposing argument is the potential for delay in diagnosis, delay in transfer, and prolonged time to definitive treatment when pediatric trauma patients undergo CT scans at referring institutions prior to transfer to a pediatric trauma center [4, 5].
We believe our observed proportion of repeated CT scans is lower than previously reported because our trauma center is dedicated to minimizing radiation exposure to patients and as such has employed a number of protocols with the goal of reducing the number of CT scans performed. Many of these modalities address the reasons for obtaining repeat CT scans that have been reported in the literature. The radiologists at our institution are dedicated to reviewing CT scans performed at referring hospitals. This is beneficial in that it allows the radiologist to determine if the imaging is adequate or if there is a need for repeat scan for further evaluation. It may also contribute to our low incidence of missed injury. We utilize web-based systems that allow referring hospitals to push digital images directly to our institution. This allows for quick access to these images for review and eliminates the issue of incompatibility with transferred images on CDs. When patients arrive to our institution without imaging, all possible efforts are made to obtain these scans by communicating with the referring facility and using couriers to transport the images. Importantly, our trauma team is aware of our efforts to reduce CT imaging in pediatric patients. The decision for the need for CT scans is made after a thorough evaluation of the trauma patient and is largely based on the clinical status of the patient in combination with the mechanism of injury. This practice holds true for repeated CT scans for which the necessity of a duplicate scan is determined by the attending physician that is ultimately responsible for the clinical care of the patients. This may be the trauma surgery, emergency room, or neurosurgery attending.
It is important to note that repeat CT scans for certain body regions may be appropriate or necessary, such as CT scans of the head to assess for progression of injury. Our finding that head CT is the most frequently repeated scan is consistent with that reported in the literature. One study found that 90 % of patients required duplicate head CT scans within 4 h [5]. Hartin et al. reported that 21 % of patients underwent repeat head CT, with 80 % of these done in a continuum of care to monitor progression of a lesion or due to a change in the patient’s condition [6]. The incidence of repeated head CT in our experience was 20 % and is consistent with standard of care for documented head injuries.
One retrospective cohort study found that 66 % of pediatric trauma patients who underwent CT scans at a referring hospital met criteria for immediate transfer to a pediatric trauma center without pre-transfer CT imaging. They found that 45 % of patients less than 10 years of age who were transferred had CT scans that were negative for any injury and noted that 27 % of patients underwent duplicate CT within 4 h of arrival [8]. In our experience, 16 % of patients who underwent repeat CT scan after transfer, had negative findings on head, chest, or abdominopelvic CT scans at the referring hospital. It was noted that 9 % of head CT scans and 7 % of abdominopelvic CT scans initially read as positive at a referring hospital were not found to have injuries noted on repeat imaging.
There were significantly more duplicate scans performed when patients were transferred from referring facilities that were of further distance from the trauma center. There may be an increased pressure to screen patients to assess for appropriateness of transfer or fear of missing significant, life-threatening injuries prior to a long distance transfer. However, these patients may then be subjected to repeat imaging after arrival to the trauma center if these images are not transferred with the patient, if they are inadequate or incomplete, if there are changes in the patient’s clinical condition, or for further evaluation of injuries identified on outside scans. Significantly more duplicate scans were also performed in patients with higher ISS, lower GCS, and after more significant mechanisms of injuries. This is similar to what has been reported in the literature with patients presenting with more severe injuries undergoing a higher number of repeat imaging [9].
When comparing the results of the referring facility head and abdominopelvic CT scans to those that were repeated at our institution, it was determined that there was substantial agreement between the two results for head CT and moderate agreement between the two results for abdominopelvic CT. One prospective study of 410 consecutive trauma patient transfers noted that up to 13 % of patients had different CT results on repeat imaging. Two thirds that were initially read as abnormal at the referring institution, were read as normal on repeat imaging, while one third initially read as normal at the referring institution, were read as abnormal on repeat imaging [9].
Over the 11-year study period, the overall incidence of missed or delayed diagnosis for patients who underwent CT scans at referring hospitals prior to transfer to our pediatric trauma center was 0.7 %. Of those patients with missed injuries, 15 (36 %) had undergone a repeat CT scan. Thirteen were found to have a positive result on repeat CT after an initial negative scan from the referring hospital, seven were noted to be positive following re-interpretation of the referring hospital scan, four were found on a late initial scan, and eighteen were orthopedic injuries noted after obtaining extremity films. One retrospective study of 382 pediatric trauma patients reported that up to 38 % of patients were found to have injuries on repeat CT scans. However, of patients undergoing repeat scans, ten arrived without imaging from a referring hospital and four arrived with imaging but with no official review by a radiologist at the referring trauma center. It was noted that no missed injuries were found in patients that arrived with imaging that was reviewed by a radiologist in the trauma center [7]. There is a low incidence of missed injury in patients whose CT scans are reviewed by a radiologist. This practice, with proper protocols, therefore, may reduce the number or need for repeat CT imaging.
The extent of radiation exposure in the pediatric population is of great interest. Recent literature has expressed concerns regarding the increasing number of CT scans performed and subsequent increase in radiation exposure to patients in this population. The radiation exposure from an abdominopelvic CT scan is equivalent to approximately 100–250 chest radiographs [3]. One report estimated the development of approximately one fatal cancer for every 1000 CT scans performed in children [3]. This was based on a study by Brenner et al. that reported a potential of 500 cases of fatal cancers from the CT scans performed on children less than 15 years old annually [10]. Recognition of this potential cancer risk has prompted the development of programs such as ALARA (as low as reasonably achievable) in 2001 and the Image Gently Campaign, which strive to raise awareness and reduce radiation exposure in children [11, 12]. We, therefore, encourage other institutions to investigate their own CT imaging practices and to take a proactive approach in minimizing radiation exposure in the pediatric population.
There are some limitations to our study. This was performed at a single pediatric trauma center, making it difficult to generalize to the entire trauma population. The greatest limitation is the retrospective nature of the study, which may affect a number of areas of our analysis. We relied on our institutional trauma registry to obtain data on patients. Per this registry, 6041 underwent CT scans at the referring hospitals prior to transfer. There is the possibility that some patients may have been scanned at the referring hospital and their images not transferred and therefore not included in the cohort of patients who underwent CT scans at the outlying facility. This may underestimate our rate of repeated CT scans. Another limitation is the inability to determine the exact indication for obtaining repeat CT imaging at our institution. We are unable to determine if scans were repeated due to missing or inadequate imaging or secondary to a change in the clinical status of the patients. Again, with our efforts to minimize the number of scans with the above-mentioned modalities and limiting scans based on clinical status and trauma team evaluation we infer that scans were repeated only when clinically indicated or when referring scans were incomplete, unable to be obtained, or insufficient for analysis. Lastly, we are unable to determine specifically during which level of care missed or delayed injuries occur; whether it is from erroneous interpretations from the referring institutions or at our institution.
Conclusion
The incidence of repeated CT scans over an 11-year period was 5 %, with a decreasing trend in the number of scans repeated over the last 4 years. This decrease in number of repeated scans has not resulted in an increase in missed injuries. Patients undergoing repeat CT scans were younger in age, presented with higher acuity injuries, and presented after more significant mechanisms of injury. In conclusion, in a pediatric trauma center that has implemented radiation reduction protocols for the evaluation of trauma patients, the need for repeat imaging is minimal. This approach results in an incidence of missed injury of 0.7 %. With the application of such protocols, it is possible to avoid routine, repeat CT scans in transferred pediatric trauma patients.
References
National Cancer Institute. http://www.cancer.gov/cancertopics/causes/radiation/radiation-risks-pediatric-CT. Reviewed June 7, 2012. Accessed Aug 10 2013
Tepper B, Brice JH (2013) Evaluation of radiation exposure to pediatric trauma patients. J Emerg Med 44(3):646–652
Rice HE, Frush DP, Farmer D, Waldhausen JH (2007) Review of radiation risks from computed tomography: essentials for the pediatric surgeon. J Pediatr Surg 42:603–607
Liepert AE, Cochran A (2011) CT utilization in transferred trauma patients. J Surg Res 170:309–313
Chwals WJ, Robinson AV, Sivit CJ, Alaedeen D, Fitzenrider E, Cizmar L (2008) Computed tomography before transfer to a level I pediatric trauma center risks duplication with associated increased radiation exposure. J Pediatr Surg 43:2268–2272
Hartin CW, Jordan JM, Gemme S, Glick PL, Caty MG, Ozgediz DE, Bass KD (2013) Computed tomography scanning in pediatric trauma: opportunities for performance improvement and radiation safety. J Surg Res 180:226–231
Cook SH, Fielding RJ, Phillips JD (2010) Repeat abdominal computed tomography scans after pediatric blunt abdominal trauma: missed injuries, extra cost, and unnecessary radiation exposure. J Pediatr Surg 45:2019–2024
Benedict LA, Paulus JK, Rideout L, Chwals WJ (2014) Are CT scans obtained at referring institutions justified prior to transfer to a pediatric trauma center? J Pediatr Surg 49:184–188
Haley T, Ghaemmaghami V, Loftus T, Gerkin RD, Sterrett R, Ferrara JJ (2009) Trauma: the impact of repeat imaging. Am J Surg 198:858–862
Brenner D, Elliston C, Hall E, Berdon W (2001) Estimated risks of radiation induced fatal cancer from pediatric CT. Am J Roentgenol 176:289–296
The alliance for radiation safety in pediatric imaging. Image Gently Campaign. http://www.imagegently.org/Home.aspx. Revised Jan 1 2014. Accessed Aug 10 2013
Slovis TL (2002) The ALARA (as low as reasonably achievable) concept in pediatric CT intelligent dose reduction. Multidiscipliary conference organized by the Society of Pediatric Radiology. August 18–19, 2001. Pediatr Radiol 32:217–317
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Farach, S.M., Danielson, P.D., Amankwah, E.K. et al. Repeat computed tomography scans after pediatric trauma: results of an institutional effort to minimize radiation exposure. Pediatr Surg Int 31, 1027–1033 (2015). https://doi.org/10.1007/s00383-015-3757-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-015-3757-1