
Abstract
Background
Low intelligence quotient (IQ) and delayed psychomotor development (DPD) are formidable complications of hydrocephalus. The aim of this study was to evaluate the academic performance and social integration of children operated on for hydrocephalus in Cameroon.
Method
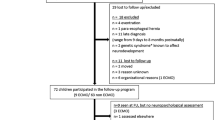
The authors present a cross-sectional study with retrospective data collection from January 2010 to May 2020. All children less than 10 years of age who had undergone surgery for a ventriculo-peritoneal shunt indicated for hydrocephalus with a post-operative evolution of 7 to 10 years and who were attending school were included. Academic performance was assessed using the Wechsler Intelligence Scale for Children IV (WISC IV), and social integration was assessed using the Vineland II score.
Results
Of the 45 children aged 7 to 10 years who attended school and were followed-up, the sex ratio was 1.25 in favor of males. 77.8% of these children had a malformation with paralysis being the most common functional sequela (29%). 73.3% of our patients had good social integration. Fifty-three percent of patients had reduced academic performance, with non-verbal performance being the most frequent (62.2%). Long-term memory was the most impaired, with 73.3% having a very low speed of information processing. Non-verbal performance was the most affected (62.2%) particularly long-term memory. Forty percent had an IQ below 70. The statistically significant determinants of social integration were age, sex, malformative etiology, and good psychomotor development, and the statistically significant determinants of educational delay were age, malformative etiology, IQ below 70, and time to care. Academic performance was reduced in more than half of our patients, but most of them had good social integration.
Conclusion
Early diagnosis and management improve the chances of good psychomotor development and IQ.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hydrocephalus is defined as an abnormal accumulation of cerebrospinal fluid (CSF) in the craniospinal enclosure under a regime of elevated pressure at a given time in its evolution [1]. Hydrocephalus is a common condition in pediatric neurosurgical practice. It is the most common cause of brain surgery in children. The intelligence quotient, or IQ, is the result of a psychometric test intended to provide a standardized quantitative indication of human intelligence. Ventriculo-peritoneal shunt (PVS) is the drainage of excess CSF from the cerebral ventricles into the peritoneal cavity. It is the standard treatment for hydrocephalus and by far the most widely used in sub-Saharan Africa.
In the United States, the rate is between 4 and 10 per thousand live births [2]. In France, it is estimated at 1 in 2000 births [3]. In Yaounde, Cameroon, there are about 1.1 cases of congenital hydrocephalus due to malformation per 1000 births [4].
Intellectual complications and difficulties in social adaptation are among the most serious complications. However, in our country, data on these complications are scarce. The aim of this study was to evaluate the academic performance and social integration of children operated on for hydrocephalus at the Yaounde Central Hospital after a post-operative period of 7 to 10 years.
Method
Data were collected from 2 main sources: operating theatre registers and medical records from the neurosurgery department. Included in the study were hydrocephalic children aged ≤ 10 years, with a minimum post-operative period following VPS of 7 years and attending school.
The parents were contacted by telephone and appointments were scheduled. During these meetings, the parent/child pairs were invited to take part in the study by means of an assessment of academic performance using the WISC IV scale and an assessment of social integration using the Vineland II scale after obtaining informed consent from the parents and assent from the children. For data analysis, quantitative variables were described by the mean and standard deviation. Measures of association were expressed in terms of odds ratio (OR). The results of the statistical tests were considered significant for a p value < 0.05 and a 95% confidence interval and presented in table form.
Results
We examined 45 children. We had 25 boys (56%) and 20 girls (44%) per group, giving a male–female sex ratio of 1.25. In our sample of 45 patients, 56% were aged 10 years and 44% were aged 7 years. Table 1 shows the demographic and social distribution of the parents of children operated on for hydrocephalus.
In our study, the most common cause of hydrocephalus was malformation (77.8%) (Table 2).
Tetra-ventricular hydrocephalus was the most common, with a rate of 64.4%. Most of our cases were referred late (42.2%). Trans-fontanellar ultrasound was the most commonly used imaging test, at 53.3%.
Regarding social integration, the assessment of our study population showed that 25 of our patients (55.6%) were in good general condition, compared with 44.4% who were ill. Regarding patient autonomy, 55.6% of our patients were autonomous. Regarding the socialization of our patients, 32 of them (71.1%) had adequate socialization.
Regarding schooling, most of our patients were behind in their studies, and primary (class) 2 was the class most frequently repeated (24.4%), 15.6% had a normal education, and 4.4% had already reached secondary school (Table 3).
Most of our patients, 53.3%, had repeated more than 2 years. According to the WISC IV test, 51.1% of patients had poor verbal reasoning. Perceptual reasoning was poor in 62.2% of cases. 48.9% had very poor working memory. 73.3% had very poor processing speed. In 22.2% of patients, the verbal comprehension index was normal; the perceptual reasoning index was low at 17.8%. The working memory index was normal in 13.3% and the processing speed index in 15.6%. 33.3% of our patients had an IQ > 90, and 40% an IQ < 70 (Table 4).
A delay of more than 4 months in treatment was associated with academic delay and was statistically significant (p = 0.001). Age was statistically significantly associated with academic delay, while there was no association between gender and academic delay (OR 0.38, (0.09–1.66), p = 0.287). There was an association between malformation and educational delay (p = 0.002).
Tetra-ventricular hydrocephalus was not associated with the risk of educational delay (OR 1.05, (0.25–4.32), p = 0.949). IQ below 70 was significantly associated with educational delay (p = 0.001).
For the significance threshold that we defined in our study population for the p value < 0.05, it occurs that a time limit before treatment of less than 4 months was associated with good social integration (p = 0.006).
Age was also associated with good social integration; this association was statistically significant. There was a statistically significant association between malformative etiology and social integration (p = 0.004). Long-term complications were associated with poor social integration (p = 0.001). Delayed psychomotor development was contributive to poor social integration with a relative risk of 6, and this association was statistically significant (p = 0.005) (Table 5).
Discussion
The male predominance classically described in literature [5,6,7] was found in 56% of cases, with a sex ratio of 1.25. This predominance can be explained by the probable lethality of female fetuses linked to Bicker-Adam syndrome, which is transmitted in a recessive Mendelian manner linked to the X chromosome. In fact, when the female fetus survives, the girl who is born will carry the gene that she will pass on to her boys.
At the time of surgery, most of our patients were less than 6 months old. The early expression of malformative diseases such as hydrocephalus would explain the preponderance of this age group. These age groups are also found in literature through the work carried out by Kante et al. in Mali [8] and Djientcheu et al. in 2011 in Cameroon [9]. At the time of data collection, our patients were aged 7 and 10 years, the ideal age for assessing the performance of a child with hydrocephalus [10].
In our study, 71.1% of patients lived in urban areas. This predominance of urban children may be explained by the fact that people living in large cities have easy access to healthcare.
Although most of the literature describes brain scans as the most commonly performed radiological investigation [11, 12], trans-fontanellar ultrasound was the main investigation performed in our study to confirm the diagnosis involving 24 children (53.3%). This result can be explained by the fact that most of the children who were less than 6 months old at the time of surgery had an open anterior fontanel and could therefore benefit from this examination. In addition, given its low cost, complete safety, and easy handling, this examination was more accessible. Gathura et al. [13] in Kenya found this to be the case. In our study, hydrocephalus originated from malformation in 77.8% of cases, followed by infectious causes in 17.8% of cases. The non-respect of folic acid prophylaxis and genetic mutations could explain the dominance of malformative etiologies. These findings are similar to those of Djientcheu et al. and Mouafo et al. [4, 14]. In contrast, European authors reported a predominance of congenital causes, followed by hemorrhage, then tumor and infectious meningitis. This difference is thought to be linked to the still high prevalence and inadequate management of meningitis in Africa.
The outcome of children with hydrocephalus depends on several factors, among which the time limit before treatment. As has been shown in literature, early treatment before severe irreversible cerebral lesions set in, and before damage caused by intracranial hypertension, is conducive to a good prognosis. In a study by Topczewska-Lach in Poland [15], the aim was to analyze the long-term outcome of children with shunt-treated hydrocephalus, with emphasis laid on their psychomotor development. The later revealed that 30% of the children had an IQ above 90, 24% between 70 and 90, 26% between 50 and 70, and 20% below 50. About general condition, 44.4% of our patients remained sick; our results contradict those of Broalet et al. at Ivory Coast in 2017, who found only 18.4%. These differences may be explained by the delay in management observed in our study, unlike their study where management was earlier [11].
Regarding sociability, 71.1% of our patients were well integrated into society, a result obtained using the Vineland II scale, which is also used by other authors with almost similar results. Hommet et al. in 1999 in France [16] found that the greater majority of their patients had a good social adaptation. Fletcher et al. in the United States also used the Vineland II scale and obtained similar results [17]. These generally good results, despite the cognitive and motor impairments observed in these patients, may be explained by the fact that young children with hydrocephalus are in phase with their development in terms of general social skills; indeed, Rourke et al. in 1994 and Holler et al. in 1995 in the United States [18, 19] demonstrated that older children are more vulnerable than younger children in terms of their adaptive and social behaviors. Older children have more behavioral problems and less developed social skills than younger children. These findings support the idea that as children with hydrocephalus grow older, problems with their ability to manage their behavior and conform to acceptable norms become more apparent.
Concerning the working memory index, 48.9% of our patients obtained a very poor score, 37.8% obtained a poor score, and only 13.3% obtained a normal score. Christine Cull and colleagues in 2008 in Canada [20] also used the Wechsler intelligence scale and obtained similar results: 50.1% had a low capacity for retaining information. Another study using a tool other than the Wechsler intelligence scale also obtained a low result. According to Wanters and Wanters, these results depend on the ability to use semantics to encode and retain information. These results can be attributed to the fact that hydrocephalus patients are affected by amnesic disorders due to lesions of the temporal lobe similar to those found in amnesic patients [21, 22].
Concerning the processing speed index, 73.3% of our patients had a very low data processing speed. Cull et al. in their 2008 study using the same tool found 61.1%. These results may be explained by the fact that hydrocephalus patients process visual-spatial information more slowly [20]. These results may also be explained by the fact that 40% of our patients had an IQ below 70; Dennis et al., 1981 in Canada [10], obtained a better result (21%) because only patients with an IQ above 90 were included in their study.
Regarding IQ, 40% of our patients had an IQ below 70. These results are similar to those of Soare et al. who found a rate of 37% [23], and in contradiction with the results of Billard in 2008 who found a rate of 75% [24] also, Casey et al. in London [25] found that 53% of their patients had an IQ above 80; Hoppe-hirsch et al. in France [26] found 32% with an IQ above 90. These discrepancies can be explained by the fact that the neuropsychological study highlights frequent IQ heterogeneity due to deficits in constructive cognitive skills such as visuo-spatial skills, the presence of epilepsy, and the cause of the hydrocephalus. Post meningeal and post hemorrhagic neonatal hydrocephalus are often considered to have the worst intellectual prognosis. Similarly, in the case of fetal hydrocephalus, the intellectual prognosis is more severe because of cerebral atrophy caused by prolonged distension or because of associated lesions [24].
Conclusion
The long-term academic performance of these children depends on how early they are diagnosed, how early they receive treatment, the quality of the treatment, the etiology of the hydrocephalus, associated malformations, and their parents’ income and level of education.
Non-verbal performance was the most affected and was due to lesions of the white matter of the right hemisphere or to surgical maneuvers. As for verbal performance, our patients’ language was fluent, with a rich vocabulary and good syntax; however, it was poorly adapted.
Primary two was the most repeated class; very few of them had a normal curriculum and were already in secondary school. The verbal reasoning index, perceptual reasoning index, working memory index, and processing speed index were normal in a quarter of our patients.
The IQ was below 70 in 40% of our patients, due to the attention, cognitive, and visuo-spatial difficulties observed in these patients and to poor non-verbal performance. Delay in treatment, age, malformative etiology, and IQ were determinants that increased the risk of educational delay, with a statistically significant difference. Similarly, age, malformative etiology, and delayed psychomotor development had a significant influence on social integration.
Data availability
No datasets were generated or analyzed during the current study.
References
Moutard ML, Fallet-Blanco C (2004) Foetal malformative neurological pathologies pédiatric. EMC Pediatry 7(3):210–213
Abena A, Dongmo L, Kagmeni Gaggini J, Carama M, Mbede J (1994) L’hydrocéphalie en milieu pédiatrique à Yaoundé, Cameroun : étude de 69 cas. Ann Pédiatr 41(4):249–252
Awad El (1992) Infantile hydrocephalus in the south-western region of Saudi Arabia Ann Trop Paediatr 12(3):335
Kamla JI, Kamgaing N, Fongang EN, Fondop J, Billong S, Djientcheu V (2017) Epidémiologie des Malformations Congénitales Visibles à la Naissance à Yaoundé. Health Sci Dis 2(2):67–68
Venkataramana NK, Mukundan CR (2011) Evaluation of functional outcomes in congenital hydrocephalus. J Pediatr Neurosci 6(1):4–12
Frank Netter H (1999) Atlas d’anatomie hummaine
Bc W (2013) Congenital idiopathic hydrocephalus of infancy: the results of treatment by endoscopic third ventriculostomy with or without choroid plexus cauterization and suggestion for how it works. Chidls Nerv Syst 29(6):35–40
Boubou K (2000) Prise en charge chirurgicale des hydrocéphalies non traumatiques chez les enfants de 0 à 24 mois. Thèse Med Bamako 7(8):22–30
de Paul Djientcheu V, Nguefack S, Mouafo TO, Mbarnjuk AS, Yamgoue TY, Bello F et al (2011) Hydrocephalus in toddlers: the place of shunts in sub-Sahara African countries. Childs Nerv Syst 27(12):2097–100
Dennis F, Netley S, Harwood-Nash H, Hoffman H (1999) The intelligence of hydrocephalic children. Archs Neurol 3(8):607–615
Broalet M, Drogba L, Kaoudi AM, Konan S, Konan L, BourgiH HaroY, Ba Zézé V (2016) Profil épidémiologique et étiologique de l’hydrocéphalie de l’enfant au service de neurochirurgie du CHU de Yopougon à Abidjan. Afrique BioMédicale 21(2):4–1
Abdelrahim Z (2012) Hydrocéphalie du nouveau-né et du nourrisson à propos de 78 cas. Thèse de médecine Fès 13(7):31–58
Gathura E, Poenaru D, Bransford R, Albright AL (2010) Outcomes of ventriculoperitoneal shunt insertion in Sub-Saharan Africa: clinical article. J Neurosurg Pediatr 6(4):329–335
Mouafo Tambo F, Chiabi A, Walburga Y, Sosso M, Djientcheu V, Mbarnjuk S et al (2011) Our experience in the management of infantile hydrocephalus: a study on thirty-five regrouped cases in Yaoundé, Cameroon. African J Paediatr Surg Medknow Publications Media Pvt 8(2):199
Topczewska-Lach E, Lenkiewicz T, Olański W (2005) Zaborska A Quality of life and psychomotor development after surgical treatment of hydrocephalus. Eur J Pediatr 15(1):2–5
Hommet C, Billard C, Gillet P, Barthez MA, Lourmiere JM, Santini JJ, de Toffol B, Corcia P, Autret A (1999) Neuropsychologic and adaptive functioning in adolescents and young adults shunted for congenital hydrocephalus. J Child Neurol 14(3):144–150
Fletcher JM, Bohan TP, Brandt M, Brookshire B, Beaver S, Francis DJ, Davidson K, Thompson NM, Miner ME (2004) Verbal and nonverbal skill discrepancies in hydrocephalic children. J Clin Exp Neuropsychol 14(6):593–609
Donders J, Canady AI (1990) Rourke Psychometric intelligence after infantile hydrocephalus. A critical review and reinterpretation. Childs Nerv Syst 6(3):148–154
Holler KA, Fennell EB, Crosson B, Boggs SR, Mickle JP (1995) Neuropsychological and adaptive functioning in younger versus older children shunted for early hydrocephalus. Child Neuropsychol 1(1):63–73
Cull C (2008) Wyke, Memory function of children with spina bifida and shunted hydrocephalus. Dev Med Child Neurol 2(6):177–183
Andersson S, Persson EK, Aring E, Lindquist B, Dutton GN, Hellström A (2006) Vision in children with hydrocephalus. Dev Med Child Neurol 48(10):836–841
Parsons JG (2001) An investigation into the verbal facility of hydrocephalic children with special reference to vocabulary, morphology and fluency. Devi Med Child Neur Suppl 10(9):110
Raimondi AJ, Soare P (1999) Intellectual development in shunted hydrocephalic children. Am J Dis Child 12(7):64
Billard C, Santini JJ, Gillet P, Nargeot MC, Adrien JL (2008) Long-term prognosis of hydrocephalus with reference to 77 children. Pedi- atric Neuroscience 12(8):219–225
Casey AT, Kimmings EJ, Kleinlugtebeld AD, Taylor WA (1997) Harkness WF, Hayward The long-term outlook for hydrocephalus in childhood. A ten-year cohort study of 155 patients. Pediatr Neurosurg 27(2):63–70
Hoppe-Hirsch E, Laroussinie F, Brunet L, Sainte-Rose C, Renier D, Cinalli G, Zerah M (1998) Pierre-Kahn A (1998) Late outcome of the surgical treatment of hydrocephalus. Child’s Nerv Syst 14(9):97–99
Author information
Authors and Affiliations
Contributions
Haman Oumarou was the study designer and manuscript writer. Ndome Toto: data collection and statistics analysis. Bello Figuim: Data interpretation. Djientcheu Vincent: Supervisor of the study.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
O., H.N., O., N.T., Figuim, B. et al. Evaluation of academic performance and social integration of children operated for hydrocephalus in Cameroon. Childs Nerv Syst 40, 1777–1782 (2024). https://doi.org/10.1007/s00381-024-06360-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-024-06360-5