
Abstract
Introduction
Abusive head injuries is a major cause of severe morbidity and the main cause of mortality by head trauma in infants.
Material and methods
Based on published data and their own clinical and medicolegal practice, the authors review briefly the historical roots and emergence of the concept of abusive head injuries (AHI), until the present scientific understanding of shaken baby syndrome (SBS) and Silverman syndrome. They then discuss the present epidemic of denialism and how this challenge to science should be seen as a stimulus to increase research and improve the accuracy of diagnosis and medical practice.
Results
The denial of SBS is especially damaging because it undermines the possibilities of prevention and reparation for victims. The authors expand on AHI being part of a wider context of domestic violence and the prevention of child abuse being part of a broad and long-term endeavor to defend civilization values.
Conclusions
Prevention of AHI is a major challenge for the future. In the fields of science and prevention of child abuse, the input of pediatric neurosurgeons should not be underestimated.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
We are very happy that the journal Child’s Nervous System has entrusted us to edit the present annual issue on abusive head injuries (AHI). Our journal has always stood boldly at the forefront of advances in all domains in which pediatric neurosurgeons are involved and has never shied from controversy and innovative thinking. We are grateful that it continues to serve as a think tank in this particular domain like in many others.
The present issue will deal with many important topics in which recent advances help us in the understanding of the shaken baby syndrome (SBS) and other AHI, their diagnosis, and the actions of prevention to be put in place. It also contains an overview of how pediatric neurosurgeons are involved in the clinical and surgical management, legal proceedings and research on AHI, and how this condition is managed in different parts of the world.
In the present article, we shall briefly review the historical emergence of the knowledge of AHI, the present controversies, and how the future of prevention should become part of the broader picture of the struggle against domestic violence.
Child abuse in history: an overview
The notion of child abuse did not emerge until the child became recognized as an individual person with legal rights. Before that, the child under majority age, and often even later, was considered as totally dependent on the pater familias, who detained on him a right of life and death (jus vitae necisque). Infanticide was widespread in early societies, like Greece (think of the infant Œdipus being exposed to feral beasts) as well as more recently in the pacific islands as a harsh method of population control. Ancient Roman history is dotted with “virtuous” examples of fathers sacrificing their progeny, like the much-celebrated consul Titus Manlius Imperiosus Torquatus slaying his own son for disobeying military orders, as accounted by Livy. This ethos was little improved during the Middle ages and even worsened through a reviving of “antique values” during the Renaissance.
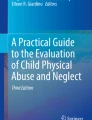
The modern era marks a turning point around the middle of the nineteenth century, illustrated in 1850 (2 years after slavery was definitely abolished in France) by the watercolor by Honoré Daumier (Fig. 1), under the telling title “fatherly discipline” [1]. The artist’s graphic message illustrates the emergence of a new attitude toward domestic violence around this period. Ambroise Tardieu’s medical thesis, published in 1860 (Fig. 2), was the first medical description of the beaten child syndrome, including explicit depictions of fatal AHI; this text was recently made available in English [2]. The first child protection law in France was followed in 1889; however, corporal punishment was not abolished until 1935, and spanking became outlawed only in 2016.

Honoré Daumier: “la correction paternelle” (fatherly discipline) (1851–1852) the Arts institute, Chicago IL. This watercolor captures the drama of child abuse: the incessant cries of the terrified infant, the angry father, the anxious mother, and the seclusion of a jammed home at night

Ambroise Tardieu (right) and the frontispiece (left) of his medical thesis published in 1860
In the last century, the decisive medical breakthrough of roentgenology led to the recognition of characteristic patterns of fractures and the description in 1953 by Frederic Silverman (a radiologist) of the beaten-child syndrome, associating fractures of different ages with intracranial lesions [3]. In 1972 (shortly before the advent of computed imaging), Caffey described the shaken baby syndrome (SBS) associating subdural hematomas (SDH) with retinal hemorrhages (RH) and encephalopathy [4]. From the start, this bold conceptual jump (potentially lethal traumatic lesions without impact) suffered from a dual handicap: to occur in the seclusion of individual homes (as illustrated by Daumier) with no independent witness and the difficulty to reproduce experimentally human infantile lesions in an animal model. The issue was nuanced by the description by AC Duhaime, 15 years later, of an intermediate entity, the shaken-impact syndrome which associated skull fractures with SDH and RH, and carried a dire prognosis (the description was made on autopsy cases) [5]. During the following decades, the concept of SBS was consolidated by the production of a large scientific corpus, with clinical data [6], imaging [7], autopsy findings [8], the confessions of perpetrators [9], corroborated by animal experiments [10], computer models [11], artificial intelligence [12], as well as the occasional video footage caught on video-surveillance [13], and contrary the reduction of cases of SBS after prevention campaigns [14, 15].
The denialist epidemics
As a reaction to the widespread diffusion of the concept of SBS and other AHI in medical practice and their legal implications, a growing current of dissent has developed for many years, denying the diagnostic criteria, and even the very existence of the SBS, in spite of the abundant and convergent evidence cited above. This denialist current, often instrumental to vested interests, operates mostly in courts, where it has developed great obstructive powers, but it also pervades more and more the medical literature [16] and has become the purpose of many letters to editor and answers, often in acerbic or even vitriolic tone.
The “triad” polemic is emblematic. The term “triad” (RH, SDH, and encephalopathy) is mostly used not only by denialists [17] but also by contamination, often adopted candidly by others. In our opinion, this is an oversimplification of SBS mostly directed to non-specialists. As Christian and coworkers explain in the present issue, this is a “strawman argument,” in which an enemy is depicted in terms that can be attacked and defeated more easily. The reality of AHI is more complex and subtle, as illustrated in Fig. 3, and we think scientists and clinicians should not allow others to shut them in a box. This so-called triad is in fact an outdated concept, being a historical heritage from a time when only the most severe cases of SBS were identified, and brain “edema” was a common (and ominous) finding. We now know that, hopefully, many cases of SBS are diagnosed without (or before) having cerebral lesions, and only a minority require intensive care and even less are intubated (44.3% and 31.1% respectively in our experience). As a result, the majority of cases of SBS are diagnosed with essentially a dyad: SDH plus traumatic RH. Interestingly, the perpetrators’ confessions show that many children have suffered previous episodes of shaking before appearing on the medical radar screen [9].

Tentative synthesis of the different clinical findings in AHI and how these are analyzed individually and seen in the perspective of one another. Medical students are now well acquainted with the conditional logic of script concordance tests, e.g., if imaging and fundoscopy indicate severe trauma and no impact is visible, then shaking is likely. This diagram suggests that skull fractures will be interpreted differently according to the context, in favor of accidental trauma or shaken-impact syndrome or Silverman's syndrome. This diagram is intent to show that the diagnosis of AHI is more complex but also more nuanced than just identifying the three elements of a so-called triad. OCT, optic coherence tomography
The onus has now shifted toward a precise depiction and rigorous interpretation of the lesions, informed by deep clinical and scholarly knowledge. The diagnostic difficulties cannot be evacuated. As detailed in this issue by Christian and Binenbaum, ophthalmological findings may not be specific to child abuse but clearly indicate severe trauma and, in turn, give sense to the presence of intracranial bleeding and the absence of signs of impact. This is also true for other ill-documented features like spinal lesions, especially lumbar wedge fractures, which are not found in accidental traumas at that age, as detailed in the present issue. The sensitivity and specificity of spinal traumatic lesions might make them as important as RH for the diagnosis of SBS.
Making a medical diagnosis does not consist of ticking boxes but rather making sense of a cluster of positive and negative findings, in the light of a clinician’s experience and scientific knowledge. As we wrote in a previous review [16], the diagnosis of AHI is unequivocal in most of the cases and made rapidly, with all due caution, as should be in an emergency context. Artificial intelligence with unsupervised cluster analysis confirms the clinical experience, showing beautiful segregation of the two groups, accidental and non-accidental [12]. Our Fig. 3 is a tentative synthesis of how the different findings, carefully analyzed individually and seen from the perspective of one another, allowing to make the diagnosis of AHI with confidence. Seen in isolation, all stars may look the same, but constellations can be recognized at first glance.
In our opinion, denying the convergent scientific evidence cannot be achieved without some intellectual biases. As seen recently during the COVID pandemic, dissenting voices, including from the scientific community, are always heard. The most vocal dissenters may be able to build a systemic thought, and their discourse may sound convincing to the public or a jury. They can even develop a parallel current like denialism but cannot claim to represent the medical and scientific community. Overall, denialist epidemics should be perceived as a challenge to improve the accuracy of diagnosis and professional rigor and increase and diffuse scientific knowledge. The controversy becomes an opportunity to sharpen arguments and clarify messages.
Clearly, the scientific response to the challenge can only be articulated in the scientific idiom. Science is not a matter of belief but a collective endeavor based on probabilities rather than certainty, in order to assess realities which appear more complex as we study them. Justice speaks a totally different language, but which may sound falsely similar. As an example, scientific uncertainty should not be mistaken with judicial doubt, and conviction has distinct meanings in a scientific or judicial context. Scientific truth cannot be ruled by decree, like in the old days of the Soviet Union, when scientists suffered under the yoke of the infamous Trofim Lyssenko. As a consequence, a legal outcome cannot be held as confirming or infirming a medical diagnosis: insufficient legal proof against an accused is in no way a proof that the victim was not abused.
The prevention of SBS
Denial of the very existence of SBS is a major impediment for the prevention of this severe, avoidable, and thus unacceptable condition. Several information and prevention campaigns have been launched for many years, using diverse media. While some of these registered successes [14, 15], others failed to identify a decrease in the incidence of AHI at their close [18, 19]. We think that the incidence of AHI is an imperfect criterion to assess the impact of preventive campaigns because the information broadcast to the public also increases awareness among the healthcare and social personnel so that the expected decrease in abuse can be offset by an increase in diagnostic exhaustiveness. The net benefit of this awareness, however, is that less severe cases are diagnosed, prompting child protection, and abuse does not repeat and become severe or even fatal. We think information and prevention campaigns should be continued and amplified, and the gold standard to evaluate their results should be the AHI-related mortality.
The cost of AHI to society is huge. In 2012, medical and hospital costs alone were approximately US $48,000 for one child [20]; when rehabilitation, education, and justice expenditures are added, the figure rises to US $2.6 million [21]. These figures set the stage for the funding of preventive measures. In the present issue, Raza and the Montreal team present the cost–benefit ratio of prevention; as always in medicine, preventing is much cheaper than treating.
Opinions diverge regarding the target of prevention: since AHI occurs in all layers of society, the general feeling is that prevention should address the whole population [22]. Such is the target of the Canadian crying plan, consisting visits in maternity wards to provide information to both parents of all newborns; it is essential that both parents are involved since 70% of perpetrators are male. On the other hand, since risk factors have been identified for AHI, like young parental age, low education, mother-at-home, single mother, as well as perinatal difficulties, in particular hospitalization at birth resulting in defective bonding [23], these criteria identify a population requiring targeted prevention. For this reason, the Canadian crying plan organizes postnatal targeted follow-up consultations. Certainly, prevention should not be monolithic, and a close follow-up of families with identified weaknesses is warranted.
The challenge of low-grade domestic violence
The incidence of AHI is evaluated by counting the new patients hospitalized for clinically significant lesions; however, among that number, it is increasingly recognized that many children survived several episodes of shaking before admission [9]. We can infer that the medically diagnosed cases of AHI represent in fact the tip of the iceberg. In one study, 2.6% of mothers surveyed admitted having shaken their baby; the authors concluded “For every 1 child who sustains a serious injury as a result of shaking, an estimated 150 children may be shaken and go undetected” [24]. In turn, these cases of low-grade physical abuse are only one feature of a backdrop of domestic violence. In the present issue, Raza et al. show that shaking often occurs in a context of ordinary domestic violence and that other forms of violence, including “educative,” sexual, intra-parental violence, and harassment, are the ordinary background of SBS. Overall, we understand that the prevention of AHI must be part of a larger endeavor. It has also been established that an abused child has a higher risk of becoming a child abuser [25, 26]. “Violence begets violence” (Mt 26:52). Breaking the cycle of violence is thus the next frontier.
We can find inspiration from what can be hailed as a success story: the repression of road violence. Traffic accidents, which in France alone peaked at about 18,000 deaths in 1970, have decreased to 2541 in 2020, while, at the same time, road traffic grew by a factor of 2.62 [27]. These impressive if incomplete results were obtained through a relentless effort combining investment, education, repression, and incitation. We are convinced that a similar, large-scale long-run effort can yield similar results regarding domestic violence, with unforeseeable benefits regarding the society as a whole. The benefits of education are already demonstrated, showing a decrease in intrafamilial violence over time [28]. This also values the role of justice services and child protection agencies, whose action is not just to punish crimes and protect victims, but also to organize follow-up with parental guidance and prevention of secondary damage.
Conclusions
We think pediatric neurosurgeons should be more involved than ever in the domain of AHI, where their knowledge and skill on neurotrauma and cerebrospinal fluid disorders are much in demand and also get more involved in legal expertise and research. From what has been developed above, we see that much has been done, but we understand that much more remains to be done. We also can view the present challenges of AHI as a test to our society: can science defend its values? Can civilization, which is based on the control of violence, break its cycle? We are not at the beginning of the end, not even at the end of the beginning.
Availability of data and materials
We the authors commit ourselves to provide all data upon request.
References
Vinchon M (2006) Honoré Daumier and child abuse. Childs Nerv Syst 22:635. https://doi.org/10.1007/s00381-006-0109-4
Roche AJ, Fortin G, Labbé J, Brown J, Chadwick D (2005) The work of Ambroise Tardieu: the first definitive description of child abuse. Child Abuse Negl 29(4):325–334. https://doi.org/10.1016/j.chiabu.2004.04.007 (Epub 2005 Apr 26 PMID: 15917075)
Kempe CH, Silverman FN, Steele BF, Droegmueller W, Silver HK (1962) The battered-child syndrome. JAMA 7(181):17–24. https://doi.org/10.1001/jama.1962.03050270019004 (PMID: 14455086)
Caffey J (1972) On the theory and practice of shaking infants. Its potential residual effects of permanent brain damage and mental retardation. Am J Dis Child 124(2):161–169. https://doi.org/10.1001/archpedi.1972.02110140011001 (PMID: 4559532)
Duhaime AC, Gennarelli TA, Thibault LE, Bruce DA, Margulies SS, Wiser R (1987) The shaken baby syndrome. A clinical, pathological, and biomechanical study. J Neurosurg 66(3):409–4. https://doi.org/10.3171/jns.1987.66.3.0409 (PMID: 3819836)
Vinchon M, de Foort-Dhellemmes S, Desurmont M, Delestret I (2010) Confessed abuse versus witnessed accidents in infants: comparison of clinical, radiological, and ophthalmological data in corroborated cases. Childs Nerv Syst 26(5):637–645. https://doi.org/10.1007/s00381-009-1048-7 (Epub 2009 Nov 28 PMID: 19946688)
Adamsbaum C, Rambaud C (2012) Abusive head trauma: don’t overlook bridging vein thrombosis. Pediatr Radiol 42(11):1298–1300. https://doi.org/10.1007/s00247-012-2434-y (Epub 2012 Aug 12 PMID: 22885602)
Rambaud C (2015) Bridging veins and autopsy findings in abusive head trauma. Pediatr Radiol 45(8):1126–1131. https://doi.org/10.1007/s00247-015-3285-0 (Epub 2015 Feb 20 PMID: 25698365)
Adamsbaum C, Grabar S, Mejean N, Rey-Salmon C (2010) Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics 126(3):546–555. https://doi.org/10.1542/peds.2009-3647 (Epub 2010 Aug 9 PMID: 20696720)
Finnie JW, Blumbergs PC, Manavis J, Turner RJ, Helps S, Vink R, Byard RW, Chidlow G, Sandoz B, Dutschke J, Anderson RW (2012) Neuropathological changes in a lamb model of non-accidental head injury (the shaken baby syndrome). J Clin Neurosci 19(8):1159–1164. https://doi.org/10.1016/j.jocn.2011.12.019 (Epub 2012 Jun 15 PMID: 22705132)
Roth S, Raul JS, Ludes B, Willinger R (2007) Finite element analysis of impact and shaking inflicted to a child. Int J Legal Med 121(3):223–228. https://doi.org/10.1007/s00414-006-0129-3 (Epub 2006 Nov 8 PMID: 17091312)
Boos SC, Wang M, Karst WA et al (2022) Traumatic head injury and the diagnosis of abuse: a cluster analysis. Pediatrics 149(1):e2021051742
Fox news: mother whose child was abused… https://www.fox7austin.com/news/mother-whose-child-was-abused-by-mckinney-daycare-worker-wants-more-access-to-surveillance-video-for-parents last consulted on July 20th, 2022
Barr RG, Barr M, Rajabali F, Humphreys C, Pike I, Brant R, Hlady J, Colbourne M, Fujiwara T, Singhal A (2018) Eight-year outcome of implementation of abusive head trauma prevention. Child Abuse Negl 84:106–114. https://doi.org/10.1016/j.chiabu.2018.07.004 (Epub 2018 Aug 1 PMID: 30077049)
Fujiwara T (2015) Effectiveness of public health practices against shaken baby syndrome/abusive head trauma in Japan. Public Health 129(5):475–482. https://doi.org/10.1016/j.puhe.2015.01.018 (Epub 2015 Mar 3 PMID: 25744111)
Vinchon M, Noulé N, Karnoub MA (2022) The legal challenges to the diagnosis of shaken baby syndrome or how to counter 12 common fake news. Childs Nerv Syst 38(1):133–145. https://doi.org/10.1007/s00381-021-05357-8 (Epub 2021 Sep 25 PMID: 34564748)
Lynøe N, Elinder G, Hallberg B, Rosén M, Sundgren P, Eriksson A (2017) Insufficient evidence for ‘shaken baby syndrome’ - a systematic review. Acta Paediatr 106:1021–1027. https://doi.org/10.1111/apa.13760 (Epub 2017 Mar 1 PMID: 28130787)
Dias MS, Smith K, DeGuehery K, Mazur P, Li V, Shaffer ML (2005) Preventing abusive head trauma among infants and young children: a hospital-based, parent education program. Pediatrics 115(4):e470–e477
Zolotor AJ, Runyan DK, Shanahan M, Durrance CP, Nocera M, Sullivan K et al (2015) Effectiveness of a statewide abusive head trauma prevention program in North Carolina. JAMA Pediatr 169(12):1126–1131
Peterson C, Xu L, Florence C, Parks SE, Miller TR, Barr RG et al (2014) The medical cost of abusive head trauma in the United States. Pediatrics 134(1):91–99
Miller TR, Steinbeigle R, Lawrence BA, Peterson C, Florence C, Barr M et al (2018) Lifetime cost of abusive head trauma at Ages 0–4, USA. Prev Sci 19(6):695–704
Tursz A, Cook JM (2014) Epidemiological data on shaken baby syndrome in France using judicial sources. Pediatr Radiol 44(Suppl 4):S641–S646
Vinchon M (2017) Shaken baby syndrome: what certainty do we have? Childs Nerv Syst 33(10):1727–1733. https://doi.org/10.1007/s00381-017-3517-8 (Epub 2017 Sep 6 PMID: 29149395)
Theodore AD, Chang JJ, Runyan DK, Hunter WM, Bangdiwala SI, Agans R (2005) Epidemiologic features of the physical and sexual maltreatment of children in the Carolinas. Pediatrics 115(3):e331–e337
Glasser M, Kolvin I, Campbell D, Glasser A, Leitch I, Farrelly S (2001) Cycle of child sexual abuse: links between being a victim and becoming a perpetrator. Br J Psychiatry 179:482–494; discussion 495-7. https://doi.org/10.1192/bjp.179.6.482 (PMID: 11731348)
Lang K, Liel C, Lux U, Kindler H, Vierhaus M, Eickhorst A (2022) Child abuse potential in young German parents: predictors, associations with self-reported maltreatment and intervention use. Child Psychiatry Hum Dev 53(3):569–581. https://doi.org/10.1007/s10578-021-01157-y (Epub 2021 Mar 17. PMID: 33730359; PMCID: PMC9107397)
National interministerial observatory for road security [Observatoire national interministériel de la sécurité routière], 2022 https://www.onisr.securite-routiere.gouv.fr/outils-statistiques/series-statistiques, last consulted on August 9th, 2022
Clément ME, Chamberland C, Bouchard C (2016) Prevalence, co-occurrence and decennial trends of family violence toward children in the general population. Can J Public Health 106(7 Suppl 2):eS31–eS37. https://doi.org/10.17269/cjph.106.4839 (PMID: 26978698; PMCID: PMC6972253)
Author information
Authors and Affiliations
Contributions
Prs Matthieu Vinchon and Federico Di Rocco both made contribution in the collection of clinical data, discussions, and redaction of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Vinchon, M., Di Rocco, F. Abusive head injuries in infants: from founders to denialism and beyond. Childs Nerv Syst 38, 2275–2280 (2022). https://doi.org/10.1007/s00381-022-05671-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-022-05671-9