
Abstract
The association of the soluble suppression of tumorigenicity 2 (sST2) and the prognosis of heart failure have been well evaluated. However, little is known about the prediction of sST2 for left ventricular (LV) remodeling in acute coronary syndrome (ACS). We investigated the ability of sST2 to predict LV remodeling following the revascularization of ACS. From May 2019 to December 2020, 95 patients with LV ejection fraction (EF) < 50% who underwent coronary revascularization for ACS (unstable angina, non-ST-elevation myocardial infarction, ST-elevation myocardial infarction) were enrolled. Echocardiography and sST2 were performed at baseline and at a 3-month follow-up. The association between LV remodeling, using the end-diastolic volume index, and sST2 at baseline and at the 3-month follow-up, and the difference between each value was explored. During follow-up, 41 patients showed LV adverse remodeling. The baseline sST2 increased in patients without adverse remodeling (32.05 ng/mL vs. 23.5 ng/mL, p < 0.001), although clinical characteristics were similar between the two groups. During the mean follow-up of 3 months, a significant correlation was found in the changes between sST2 and LV end-diastolic/systolic volume index (r = 0.649; p < 0.001, r = 0.618; p < 0.001, respectively), but not in the changes of LVEF (r = − 0.132, p = 0.204). The use of angiotensin-converting enzyme 2 inhibitors/receptor blockers was higher (90.7% vs. 53.7%, p < 0.001) and sST2 decreased more predominantly in patients without adverse remodeling (23.18 ng/mL vs 26.40 ng/mL, p = 0.003). However, the changes in sST2 and LV volume were not different according to the ACS types (p > 0.05, for all). Estimates of the odds ratio (OR) for remodeling according to the sST2 difference increased substantially with a negative increase in the sST2 difference. Multivariable analysis found that, the difference between the baseline and 3-month sST2 was the most important determinant of LV remodeling following the revascularization of ACS (OR 1.24; 95% confidence interval: 1.09 to 1.41; p = 0.001). In conclusion, an increase in sST2 during follow-up was a useful predictor of LV remodeling.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute coronary syndrome (ACS) has been recognized as one of the leading causes of cardiovascular (CV) death in recent years, and its frequency increases with age and atherosclerosis-related diseases. Hence, as the prevalence of ACS increases, treatment and prevention strategies are being developed to reduce the incidence of associated CV events. However, despite these advances, the occurrence of left ventricular (LV) dysfunction and heart failure (HF) which are frequent complications of ACS, significantly impact CV prognosis.
Decreased LV systolic function can be complicated early or late, even when coronary revascularization is appropriately performed. This can be commonly related to the timing and extent of coronary reperfusion and the inflammatory status associated with ischemic heart disease. Moreover, after acute phase treatment, it is critical to accurately predict the presence and degree of complications related to cardiac dysfunction and to treat it appropriately and preventively. Recently, the soluble suppression of tumorigenicity 2 (sST2) has been recommended as a cardiac biomarker that is able to predict CV prognosis associated with ACS in the current guidelines for HF [1,2,3]. ST2 exists in two forms as a type of interleukin (IL)-1 receptor, of which sST2 endorsed as a class IIb recommendation is involved in CV remodeling, atherosclerosis, hypertension, and the progression of fibrosis [1, 2].
However, in real-world clinical practice, despite the appropriate coronary reperfusion for ACS, cardiac systolic dysfunction observed in the early stage had not yet improved during long-term follow-up and could be progressively worsened, thus resulting in an exacerbation of HF: yet, the prognostic implications of sST2 over time in ACS are not clearly understood. Furthermore, data regarding the role of sST2 even in cases of complete coronary revascularization are limited. Therefore, during a short-term follow-up of 3 months, we aimed to evaluate the relationship between the concentration of sST2 and the extent of LV remodeling in patients with cardiac dysfunction that persisted after complete percutaneous coronary intervention (PCI) for ACS.
Methods
Study patients
From May 2019 to December 2020, this prospective observational study was conducted, and we screened consecutive enrollment patients who had been referred to the emergency department for coronary PCI at the Keimyung University Dongsan Medical Center. Inclusion criteria for the patients comprised of the following: (1) age older than 18 years; (2) ACS manifested: unstable angina, non-ST-elevation myocardial infarction (NSTEMI), or ST-elevation myocardial infarction (STEMI); (3) successful coronary revascularization of culprit vessel; and (4) LVEF < 50% with regional wall motion abnormality (+) on echocardiography. For the treatment of ACS, PCI was performed based on the current guidelines; specific medications for ischemic heart disease were left to the discretion of the physicians. The patients’ medical history regarding hypertension, diabetes mellitus, ischemic heart disease, stroke, and dyslipidemia was determined. More specifically, their diagnosis of pulmonary disorders, including chronic obstructive pulmonary disease, asthma, and pulmonary fibrosis, was evaluated. According to the present study protocol, patients were regularly followed up in outpatient clinic for 3 months after discharge.
Exclusion criteria for the participating patients comprised the following: (1) the absence of baseline or follow-up results of sST2 or echocardiography; (2) more than moderate severity of valvular disorders; (3) poor image or window of echocardiography; (4) malignancy, severe active infection, or inflammation; and (5) chronic renal replacement therapy, such as dialysis or transplantation. This study was approved by the institutional review board of Keimyung University Dongsan Medical Center (Reference No. 2018-11-024), was registered with ClinicalTrials.gov (NCT03841214), and conformed to the ethical guidelines of the 1975 Declaration of Helsinki. Informed consent was obtained from all recruited patients prior to participation.
Cardiac biomarkers
Baseline sST2 was obtained at the time of study registration before performing PCI and repeated at the 3-month follow-up (± 14 days) in an outpatient clinic. After collecting the patient’s blood, plasma was separated through a centrifuge for 15 min, frozen at − 20 °C to − 80 °C and stored frozen for assays; subsequently, the Critical Diagnostics Presage® ST2 Assay Kits (Critical Diagnostics, San Diego, CA, USA) were applied to measure the sST2 concentration by specific enzyme-linked immunosorbent assay in a 76-well microtiter plate format, as previously described, and the range of the sST2 was 3.1–200.0 ng/mL, with a cutoff level < 35 ng/mL [4,5,6]. In addition, N-terminal pro-B-type natriuretic peptide (NT-ProBNP), creatine kinase-MB (CK-MB), and troponin-I as cardiomyocyte biomarkers and C-reactive protein (CRP) as an inflammatory marker were obtained at the time of ACS diagnosis in the emergency department.
Echocardiography
In all patients, echocardiography was performed at the time of study registry before PCI and at the 3-month follow-up in the outpatient clinic. According to the current guidelines, conventional 2-dimensional imaging, color Doppler, and tissue Doppler were obtained with the patient in the lateral decubitus position. Specifically, the LV end-diastolic (LVEDV)/-systolic volume (LVESV) and LVEF were measured by the modified biplane Simpson’s method, and left atrial volume was measured by the area-length method. The ratio of early diastolic mitral inflow to septal mitral tissue Doppler velocity (E/e’) was calculated. LV adverse remodeling was defined as an increase in LVEDV index at 3 months from baseline. Study patients were classified according to the presence of LV remodeling.
Primary and secondary endpoint
For the primary endpoint, we investigated the correlation between sST2 measurement and changes in LV volume. For the secondary endpoint, we investigated the correlation between sST2 and changes in LV function and sST2’s ability to predict the occurrence of CV events. Clinical CV events were defined as a primary composite of the occurrence of coronary artery revascularization, hospitalization for worsening HF, and CV mortality.
Sample size calculation
The sample size calculation was based on published data in two respects. First, the prior study of Baur et al. [7]. demonstrated that the patient with LV adverse remodeling showed an average increase in the LVEDV of 8 ± 3 ml/m2 or 12 ± 6 ml/m2 for three weeks or one year, respectively. Thus, we hypothesized that the LVEDV index would increase from baseline to 3 months > 20% compared with patients with LV reverse remodeling. An estimated sample size of 76 patients (38 per group) would be required to detect the difference with a statistical power > 80% and a two-sided alpha level of 0.05. Second, the prior study of Kercheva et al. [8] demonstrated that the myocardial infarction patient without LV remodeling showed an average decrease of 48–50% in sST2 concentration change (from 42 ng/mL to 25 ng/mL) for 3–14 days (up to 6 months). Thus, we hypothesized that the sST2 concentration related to LV adverse remodeling would approach the normal range (< 35 ng/mL, a reduction over 20%) from baseline to 3 months compared to that in patients with LV reverse remodeling. An estimated sample size of 90 patients (45 per group) would be required to detect the difference with a statistical power > 80% and a two-sided alpha level of 0.05. Overall, we decided that more than 90 patients should be required in this study.
Statistics
Continuous variables with normal distribution are presented as the mean ± standard deviation, or as the median (interquartile range: IQR) when showing a nonnormal distribution. Discrete variables are shown by frequency and percentage. Variables were compared using Student’s t test for continuous variables with a normal distribution, the Mann–Whitney U test for continuous variables with a nonnormal distribution, and analysis of variance (ANOVA) for continuous variables of three groups. A Chi-square test was used for discrete variables. A linear correlation analysis was performed for the changes in sST2 and LV volume. Logistic regression analysis was used to determine factors that might contribute to changes in LV volume. Multicollinearity among covariates was checked before performing multivariable logistic regression; to avoid multicollinearity, the reciprocal of the tolerance between the variables was defined as a variance inflation factor > 3.0. A receiver operating characteristic (ROC) curve analysis was carried out to confirm the predictive validity of sST2 on LV remodeling according to the time of sST2 collection. Comparisons were suggested using odds ratio (OR) for LV adverse remodeling according to the differences in sST2 at baseline and the 3-month follow-up. All analyses were performed using the Statistical Package for Social Science version 13.0 (SPSS Inc, Chicago, Illinois, USA) and STATA version 10.0 (StataCorp LP, College Station, Texas, USA). A p value < 0.05 was considered significant.
Results
Baseline clinical characteristics according to left ventricular remodeling
At the beginning of recruitment, 121 of 174 screened patients were enrolled. After excluding cases with poor echocardiographic imaging (n = 7) and those with an absence of follow-up data (n = 19), a total of 95 patients (mean age: 62.5 ± 11.5 years, 80 males) were entered into the final analysis (Fig. 1). During the study period, 41 patients showed LV adverse remodeling and 54 patients revealed no/reverse remodeling. Baseline clinical characteristics according to LV remodeling are presented in Table 1. There were no differences in terms of baseline clinical characteristics, previous medical illness (including ischemic heart disease and pulmonary disorders), or the manifestation of ACS at the time of study registry between the two groups. Patients without adverse remodeling showed significantly higher concentrations of CK-MB, troponin-I, NT-proBNP, and CRP than those with adverse remodeling. Interestingly, the use of angiotensin-converting enzyme 2 inhibitors (ACEIs) or receptor blockers (ARBs) was more frequently observed in patients without adverse remodeling than in those with adverse remodeling (90.7% vs. 53.7%, p < 0.001). Although the sST2 concentration was significantly higher at baseline, a decrease to normal level was confirmed at the 3-month follow-up in patients without adverse remodeling. However, the sST2 concentration significantly either remained or increased at the 3-month follow-up, rather than at baseline, in patients with adverse remodeling.

Study flow chart. ACS acute coronary syndrome, MI myocardial infarction, PCI percutaneous coronary intervention, LVEF left ventricular ejection fraction, RWMA regional wall motion abnormality, sST2 soluble suppression of tumorigenicity 2, LV left ventricle, CV cardiovascular, HF heart failure
Echocardiographic features according to left ventricular remodeling
There were no differences in terms of LV volume, E/e’ ratio, LVEF, or LA volume at the time of initial enrollment between the two groups. Both LVESV and LVEDV increased in the patients undergoing adverse remodeling during follow-up, but the changes in LVEF showed no significant difference between the patients with or without adverse remodeling. The difference in sST2 concentration did not have a significant correlation with the change in the LVEF (r = − 0.132, p = 0.204), yet it showed a significant correlation with the change in the LVESV-/LVEDV index (r = 0.649; p < 0.001, r = 0.618; p < 0.001, respectively).
Comparison of left ventricular volume changes stratified by acute coronary syndrome
A comparison of brief characteristics of study patients stratified by the index diagnosis of ACS is presented in Table 2 including the differences in important medications, cardiac biomarkers, and echocardiographic parameters. As expected, patients with NSTEMI and STEMI had higher CK-MB and troponin-I levels compared to those of UA patients. However, the groups were similar for cardiac medications and sST2 concentrations at baseline and follow-up; hence, the changes in sST2 levels of all groups were not different according to the ACS types. The manifestation of index ACS did not show a difference in relation to LV volume changes from baseline to the follow-up period (p > 0.05, for all). In contrast, an increase in LVEF during follow-up resulted in small but significant changes in UA and NSTEMI patients compared with STEMI patients; as of yet, LV remodeling could not be differentiated between the three groups.
Predictor of left ventricular remodeling
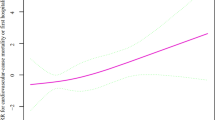
Univariable logistic regression analysis, which was performed to determine LV remodeling, revealed that the use of ACEIs/ARBs, CRP level, both baseline and follow-up sST2 concentration, and their differences (i.e., the follow-up minus initial sST2) were significant variables (Table 3). On multivariable analysis, after considering the multicollinearity between the follow-up sST2 and the follow-up minus initial sST2, the use of ACEIs/ARBs and the difference in sST2 concentration between baseline and 3-month follow-up were significant independent factors for determining LV remodeling. When constructing an ROC curve to confirm the validity of a change in sST2 over time for predicting LV remodeling, the difference between sST2 at baseline and follow-up was the most predictive and valid (AUC = 0.891, p < 0.001) (Fig. 2). Based on these findings, the adjusted OR for LV remodeling was estimated according to the change in sST2 concentration difference. Figure 3 shows that the greater the sST2 concentration difference was reversed (the more sST2 concentration was increased at the time of follow-up), the more LV adverse remodeling progression was observed.

Receiver operating characteristic curve analysis to explore the discriminating validity of sST2 at baseline and at the 3-month follow-up, as well as the difference between each concentration, which was used to detect left ventricular remodeling

Estimates of adjusted odds ratio (OR) with 95% confidence intervals for the incidence of left ventricular remodeling associated with the difference in sST2 concentration between baseline and follow-up as a continuous concentration variable. The reference of sST2 difference was 0. There was a significant increase in OR with increasing sST2 concentration during follow-up, whereas a constant OR was noted in the case of sST2 decreasing over time. Data adjusted for age, angiotensin-converting enzyme 2 inhibitor/receptor blocker, left ventricular ejection fraction, and cardiac markers (creatine kinase-MB isoenzyme and troponin-I). The red squares represent the odds ratio and the red lines represents the 95% confidence intervals
Clinical outcomes
With respect to the clinical outcomes related to sST2, CV death and coronary revascularization occurred on days 72 and 102 in two patients, respectively. Compared to the concentration of baseline sST2, the 3-month follow-up sST2 increased from 31.4 ng/mL to 47.2 ng/mL, and 26.4 ng/mL to 28.1 ng/mL. Although progression of LV adverse remodeling appeared in these two patients, no statistical significance could be found for the association with sST2 concentration because of the low incidence of CV events.
Discussion
In this study, we showed a correlation between the difference in sST2 and the extent of LV remodeling in patients with persistent cardiac dysfunction following successful PCI for ACS.
Production of sST2
ST2, an IL-1 receptor family member, has two forms, namely, the ST2 transmembrane receptor ligand (ST2L) located in the cell membrane and the soluble receptor (sST2) [9]. While the binding of IL-33 and ST2L enhances its CV protective role, sST2, which is generated in cardiomyocytes, binds with IL-33 and inhibits the effect of IL-33/ST2L when exposed to stimuli, such as inflammation, fibrosis, or stress [10, 11]. In particular, sST2 is known to be expressed at least five times more in myocardial fibroblasts than in myocardial cells [11, 12]. Therefore, sST2 plays the role of a stress hormone involved in LV remodeling; by interacting with IL-33, it can influence the development of cardiomyocyte inflammation and vascular atherosclerosis [4]. However, sST2 could be increased in pulmonary diseases (asthma, pulmonary fibrosis), autoimmune diseases (rheumatic arthritis), collagen vascular disease, and sepsis in addition to CV disorders [4, 12].
Based on these findings, sST2 is believed to be useful for predicting CV prognosis, including CV death and rehospitalization, primarily in patients with HF [1]. Since sST2 production is mainly affected by myocardial tension (stretch), fibrosis, and inflammation, it can be helpful for providing information on chronic progressive CV disorders (e.g., chronic HF), rather than ischemic coronary artery disease (CAD) [13]. These findings serve as evidence supporting the concept that the treatment guideline of HF recommends measuring sST2 to predict prognosis rather than the diagnosis of HF [1,2,3].
Basis for sST2 to predict left ventricular volume changes in remodeling
In animal experimental studies, IL-33/sST2 plays a role in LV remodeling of myocardial infarction by controlling the Yin-Yang 1 transcription factor [14]; clinically, sST2 measured in the early stage of acute myocardial infarction has shown a better correlation with LV remodeling than NT-ProBNP [8]. This is because an increased sST2 in the early stage of acute myocardial infarction (within 7 days of diagnosis or at the time of discharge) is produced mainly by fibroblasts. In general, since the main process of LV remodeling depends on myocardial fibroblasts or fibrosis, the explosive production of sST2, a biomarker that reflects fibroblast activation, can be considered a more useful index than NT-ProBNP, which responds to hemodynamic stress in a viable myocardium [15]. In addition, sST2 in the acute stage is also known to better predict LV remodeling in 3 months [16]. Thus, sST2 concentration in the acute phase may provide more important information about LV remodeling than at the chronic phase over several months [15, 17, 18]. Provided that acute myocardial infarction may be accompanied by systolic and diastolic dysfunction, sST2 could be used more frequently in cases of HF with LV remodeling in ACS than other cardiac biomarkers [17].
sST2 is often elevated in cases of myocardial injury from ACS, in which alternations in LV volume, the hallmark of LV remodeling, are the result of LV ischemic deformation and appear to be a compensatory response to changes in LV myocardial contractility to maintain stroke volume or cardiac output in patients with ACS [19, 20]. LVEF, otherwise known as a systolic functional indicator, seems to be inaccurate in defining LV global function caused by chronic HF because of those compensatory mechanisms [19]. The changes in LVEF are not synonymous with changes in contractility. Less importance of LVEF can be based on the mismatch between LVEF and stroke volume (or the presence of HF with preserved LVEF), and the poor correlation between LVEF and the severity of HF symptoms [20, 21]. The sST2 elevation in the acute phase is considerably due, in part, to myocardial cell damage, which may occur markedly within the first 4 weeks [22]. However, even after the acute phase, the sST2 concentration may continue to rise or be maintained, depending on the degree of myocardial fibrosis or inflammatory reaction accompanying the ischemic insult.
In the present study, it was noted that the baseline sST2 concentration was higher in patients without LV adverse remodeling. Given the simultaneous elevations of CK-MB, troponin-I, NT-ProBNP and CRP, it was speculated that direct myocardial damage due to ACS at the time of enrollment was greater than that of patients undergoing LV adverse remodeling; additionally, hemodynamic and inflammatory injury was estimated to be higher in the acute phase. However, the chronic progression of LV adverse remodeling, despite adequate revascularization in the acute phase, could be explained by the ongoing predominance of fibrosis following ischemic insult. These findings can be compatible with a prior basis upon which to provide a weak correlation between sST2 and myocardial enzymes [23].
One of the novel findings in this study was that the use of ACEIs or ARBs, which are known to inhibit LV adverse remodeling, was higher in patients without LV adverse remodeling. Although there were limited data about the relationship between ACEIs/ARB and sST2 concentration, a decrease in sST2 concentration and LVEF change were demonstrated by ARBs (sacubitril/valsartan) or ACEIs in patients with LV systolic dysfunction [24, 25]. Together with our results, these findings could suggest that the sST2 concentration may be affected by ACEIs/ARB that alter the profibrotic signaling pathway [26]. Since the inhibition of LV remodeling is frequently affected by these medications, it can be considered that the sST2 concentration was decreased at the time of follow-up. sST2 rises in the first few hours due to a decrease in coronary flow and decreases thereafter, and sST2 resurgence would not be observed if there were no complications associated with HF after ACS. As shown in the current study, a small decrease or resurgence in sST2 at the time of follow-up may indicate that LV remodeling can be driven by inflammatory or fibrotic reactions rather than CAD. Instead, the lack of significant differences in sST2 changes was irrespective of the index ACS manifestations, which may suggest that the changes in sST2 cannot be explained simply by a higher burden of ischemia. Therefore, even though the marked increase in baseline sST2 was caused by direct myocardial injury of ACS and LV dysfunction, it could be expected that LV remodeling may be inhibited in cases with continuously decreasing sST2 during follow-up.
Clinical implication of sST2
The measurement of sST2 at admission for acute CV disease can help not only diagnose HF, but also predict LV dysfunction that may occur later. As binding of sST2/IL-33 is mainly related to LV remodeling, the progression of atherosclerosis in CAD, failure to regulate the immune system, the remodeling of fatty tissue, or accelerated inflammation, sST2 may be advantageous for predicting prognosis over other cardiac biomarkers, such as NT-ProBNP, CK-MB, and troponin-I, in cases of CV disease accompanied by HF [27].
In the current study, we observed an extremely low area under the curve of the baseline sST2 concentration for the prediction of LV remodeling. Considering this finding, the role of baseline sST2 in the acute stage of ACS and its clinical implications remains unknown. Even though a significant difference in baseline sST2 was noted between the two groups, it seems not insufficient for the prediction of the ongoing progression of LV remodeling over time. Most likely, the concentration of sST2 in the acute phase of CV disease is believed to be a stretch marker due to the direct effects of the disease on the myocardium; however, in the subacute or chronic stable phase, follow-up of sST2 is considered an indicator of ongoing persistent fibrosis, which is followed by activation of myocardial fibroblasts, rather than a stretch marker [13]. Moreover, as the concentration change of sST2 shows a good correlation with the change in LV volume, it is expected to be useful for determining the therapeutic effect of HF medications. Particularly, when using an ACEIs or ARB, which are known to prevent LV remodeling, it is believed that sST2 reduction during follow-up can reflect the suppression of LV remodeling. Therefore, the difference between sST2 at baseline and follow-up would make sense and provide more value for identifying high risk for adverse LV remodeling.
Limitation
There were several limitations to be addressed in the current study. First, the study consisted of a relatively small number of recruited patients. Therefore, it was not possible to derive meaningful results regarding the CV prognostic ability of sST2 because of the low incidence of CV events. Second, since we targeted patients with impaired systolic function in ACS, there could be a limitation in generalizing the results of this study regardless of systolic function. Third, sST2 concentrations were not compared with NT-ProBNP, which has traditionally been used for the diagnosis and prognosis of HF. Fourth, we could not clarify when sST2 should be measured to determine LV remodeling after ACS. Last, LV remodeling was not defined as a percent change in LV volume but as the absolute value of the difference between consecutive LV volume measurements at baseline and follow-up. Postinfarct LV adverse remodeling is commonly defined as a 20% increase in LVEDV [28, 29]. However, the current definition of LV remodeling seems to be uncertain and controversial [30]: different patient populations, parameters, or imaging techniques. Considering the exploration of the quantitative correlation of sST2 concentration and LV volume changes, we believed that the absolute value of the change in LV volume would be appropriate to reflect the changes in sST2 concentration rather than the percent change. Nevertheless, it is necessary to carry out large-scale studies to compare sST2 with other biomarkers and to determine the efficacy of sST2 in a large number of patients in the future.
Conclusions
Despite appropriate PCI treatment, regional wall motion abnormalities can often be observed as a complication of ACS. This study confirmed that LV volume changes correlate well with differences in sST2 concentration. Therefore, sST2 concentration may serve as a useful cardiac biomarker for determining the efficacy of HF medications in predicting or suppressing the progression of LV remodeling in clinical practice. However, more research is needed regarding the ability of sST2 to predict the prognosis of CV events.
References
Aimo A, Januzzi JL, Bayes-Genis A, Vergaro G, Sciarrone P, Passino C, Emdin M (2019) Clinical and prognostic significance of sST2 in heart failure: JACC review topic of the week. J Am Coll Cardiol 74:2193–2203
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW, Westlake C (2017) 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 70:776–803
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL (2013) 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 128:1810–1852
Kakkar R, Lee RT (2008) The IL-33/ST2 pathway: therapeutic target and novel biomarker. Nat Rev Drug Discov 7:827–840
Ky B, French B, McCloskey K, Rame JE, McIntosh E, Shahi P, Dries DL, Tang WH, Wu AH, Fang JC, Boxer R, Sweitzer NK, Levy WC, Goldberg LR, Jessup M, Cappola TP (2011) High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ Heart Fail 4:180–187
Dieplinger B, Januzzi JL Jr, Steinmair M, Gabriel C, Poelz W, Haltmayer M, Mueller T (2009) Analytical and clinical evaluation of a novel high-sensitivity assay for measurement of soluble ST2 in human plasma–the presage ST2 assay. Clin Chim Acta 409:33–40
Baur LH, Schipperheyn JJ, van der Wall EE, van der Velde EA, Schalij MJ, van Eck-Smit BL, van der Laarse A, Voogd PJ, Sedney MI, Reiber JH, Bruschke AV (1997) Beneficial effect of enalapril on left ventricular remodelling in patients with a severe residual stenosis after acute anterior wall infarction. Eur Heart J 18:1313–1321
Kercheva M, Ryabova T, Gusakova A, Suslova TE, Ryabov V, Karpov RS (2019) Serum soluble ST2 and adverse left ventricular remodeling in patients with st-segment elevation myocardial infarction. Clin Med Insights Cardiol 13:1179546819842804
Iwahana H, Yanagisawa K, Ito-Kosaka A, Kuroiwa K, Tago K, Komatsu N, Katashima R, Itakura M, Tominaga S (1999) Different promoter usage and multiple transcription initiation sites of the interleukin-1 receptor-related human ST2 gene in UT-7 and TM12 cells. Eur J Biochem 264:397–406
Ciccone MM, Cortese F, Gesualdo M, Riccardi R, Di Nunzio D, Moncelli M, Iacoviello M, Scicchitano P (2013) A novel cardiac bio-marker: ST2: a review. Molecules 18:15314–15328
Sanada S, Hakuno D, Higgins LJ, Schreiter ER, McKenzie AN, Lee RT (2007) IL-33 and ST2 comprise a critical biomechanically induced and cardioprotective signaling system. J Clin Invest 117:1538–1549
Dattagupta A, Immaneni S (2018) ST2: current status. Indian Heart J 70:S96–S101
Pascual-Figal DA, Lax A, Perez-Martinez MT, del Carmen A-L, Sanchez-Mas J, Network GREAT (2016) Clinical relevance of sST2 in cardiac diseases. Clin Chem Lab Med 54:29–35
Asensio-Lopez MC, Lax A, Fernandez del Palacio MJ, Sassi Y, Hajjar RJ, Januzzi JL, Bayes-Genis A, Pascual-Figal DA (2019) Yin-Yang 1 transcription factor modulates ST2 expression during adverse cardiac remodeling post-myocardial infarction. J Mol Cell Cardiol 130:216–233
Petyunina VO, Kopytsya PM, Berezin AE (2018) Elevated levels of circulating soluble ST2 at discharge predict late adverse ventricular remodeling in patients with ST-segment elevation myocardial infarction. Biomed Res Ther 5:2863–2875
Bière L, Garcia G, Guillou S, Larcher F, Furber A, Willoteaux S, Mirebeau-Prunier D, Prunier F (2018) ST2 as a predictor of late ventricular remodeling after myocardial infarction. Int J Cardiol 259:40–42
Aleksova A, Paldino A, Beltrami AP, Padoan L, Iacoviello M, Sinagra G, Emdin M, Maisel AS (2019) Cardiac biomarkers in the emergency department: the role of soluble ST2 (sST2) in acute heart failure and acute coronary syndrome-there is meat on the bone. J Clin Med 8:270
Miñana G, Núñez J, Bayés-Genís A, Revuelta-López E, Ríos-Navarro C, Núñez E, Chorro FJ, López-Lereu MP, Monmeneu JV, Lupón J, Bodí V (2018) ST2 and left ventricular remodeling after ST-segment elevation myocardial infarction: a cardiac magnetic resonance study. Int J Cardiol 270:336–342
MacIver DH (2010) Is remodeling the dominant compensatory mechanism in both chronic heart failure with preserved and reduced left ventricular ejection fraction? Basic Res Cardiol 105:227–234
Fabijanovic D, Milicic D, Cikes M (2019) Left ventricular size and ejection fraction: are they still relevant? Heart Fail Clin 15:147–158
Mele D, Nardozza M, Ferrari R (2018) Left ventricular ejection fraction and heart failure: an indissoluble marriage? Eur J Heart Fail 20:427–430
Sánchez-Más J, Lax A, Asensio-López Mdel C, Fernandez-Del Palacio MJ, Caballero L, Santarelli G, Januzzi JL, Pascual-Figal DA (2014) Modulation of IL-33/ST2 system in postinfarction heart failure: correlation with cardiac remodelling markers. Eur J Clin Invest 44:643–651
Kohli P, Bonaca MP, Kakkar R, Kudinova AY, Scirica BM, Sabatine MS, Murphy SA, Braunwald E, Lee RT, Morrow DA (2012) Role of ST2 in non-ST-elevation acute coronary syndrome in the MERLIN-TIMI 36 trial. Clin Chem 58:257–266
Huang G, Zhai J, Huang X, Zheng D (2018) Predictive value of soluble ST-2 for changes of cardiac function and structure in breast cancer patients receiving chemotherapy. Medicine (Baltimore) 97:e12447
Nougué H, Pezel T, Picard F, Sadoune M, Arrigo M, Beauvais F, Launay JM, Cohen-Solal A, Vodovar N, Logeart D (2019) Effects of sacubitril/valsartan on neprilysin targets and the metabolism of natriuretic peptides in chronic heart failure: a mechanistic clinical study. Eur J Heart Fail 21:598–605
Zile MR, O’Meara E, Claggett B, Prescott MF, Solomon SD, Swedberg K, Packer M, McMurray JJV, Shi V, Lefkowitz M, Rouleau J (2019) Effects of sacubitril/valsartan on biomarkers of extracellular matrix regulation in patients with HFrEF. J Am Coll Cardiol 73:795–806
Vianello E, Dozio E, Tacchini L, Frati L, Corsi Romanelli MM (2019) ST2/IL-33 signaling in cardiac fibrosis. Int J Biochem Cell Biol 116:105619
Bolognese L, Neskovic AN, Parodi G, Cerisano G, Buonamici P, Santoro GM, Antoniucci D (2002) Left ventricular remodeling after primary coronary angioplasty: patterns of left ventricular dilation and long-term prognostic implications. Circulation 106:2351–2357
Bulluck H, Go YY, Crimi G, Ludman AJ, Rosmini S, Abdel-Gadir A, Bhuva AN, Treibel TA, Fontana M, Pica S, Raineri C, Sirker A, Herrey AS, Manisty C, Groves A, Moon JC, Hausenloy DJ (2017) Defining left ventricular remodeling following acute ST-segment elevation myocardial infarction using cardiovascular magnetic resonance. J Cardiovasc Magn Reson 19:26
Bière L, Donal E, Jacquier A, Croisille P, Genée O, Christiaens L, Prunier F, Gueret P, Boyer L, Furber A (2016) A new look at left ventricular remodeling definition by cardiac imaging. Int J Cardiol 209:17–19
Acknowledgements
This work was supported by the research promoting grant from the Keimyung University Dongsan Medical Center in Korea. The authors would like to also acknowledge J-H Jeon, RN and S-Y Kim, RN for their significant contribution to this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Park, S., Kim, IC., Kim, H. et al. Ability of soluble ST2 to predict left ventricular remodeling in patients with acute coronary syndrome. Heart Vessels 37, 173–183 (2022). https://doi.org/10.1007/s00380-021-01905-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-021-01905-z