
Abstract
Aim
We sought to explore the impact of surgical wait time (SWT) to robot-assisted radical prostatectomy (RARP) on biochemical recurrence (BCR).
Method
Retrospective review of a prospectively collected database between 2006 and 2015 was conducted on all RARP cases. SWT was defined as period from prostate biopsy to surgery. Primary outcome was the impact on BCR, which was defined as two consecutive PSA ≥ 0.2 ng/dl, or salvage external beam radiation therapy and/or salvage androgen deprivation therapy. Patients were stratified according to D’Amico risk categories. Univariable analysis (UVA) and multivariable analyses (MVA) with a Cox proportional hazards regression model were used to evaluate the effect of SWT and other predictive factors on BCR, in each D’Amico risk group and on the overall collective sample.
Results
Patients eligible for analysis were 619. Mean SWT was 153, 169, 150, and 125 days, for overall, low-, intermediate-, and high-risk patients, respectively. Multivariate analysis on the overall cohort did not show a significant relation between SWT and BCR. On subgroup analysis of D’Amico risk group, SWT was positively correlated to BCR for high-risk group (p = 0.001). On threshold analysis, cut-off was found to be 90 days. SWT did not significantly affect BCR on UVA and MVA in the low- and intermediate-risk groups.
Conclusion
Increased delay to surgery could affect the BCR, as there was a positive association in high-risk group. Further studies with longer follow-up are necessary to assess the impact of wait time on BCR, cancer specific survival and overall survival.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most common cancer for men in North America. In Canada, approximately 24,000 men were diagnosed with prostate cancer and 4100 men deceased from the disease in 2015 [1]. Radical prostatectomy (RP) has been shown to be an effective curative treatment, reducing mortality and metastasis rates [1].
Surgical wait time (SWT) to RP is an important factor to consider. Given budget restraints and ongoing cutbacks, SWT are currently on the rise in Canada. SWT in Ontario had almost doubled between 1980–1995 and 1996–2000 from 55 to 91 days [2]. Prolonged delays have been well documented to increase anxiety; stress and all around decrease their quality of life [3,4,5]. The effect of surgical delay on oncologic prognosis remains a controversial topic and a common question during patient counseling. Association between SWT and biochemical recurrence (BCR) remains equally provocative, with only a limited number of studies reporting a trend towards an increased risk of BCR with surgical delays [6,7,8].
Most analyses performed on such topic were conducted prior to the era of minimally invasive and robotic surgery. There are thus different, novel aspects that are specific to this type of surgery that must be considered. Given that only a few specialized surgeons perform RARP on a limited number of robots in Canada (24 in 2017), concentrated mainly in select metropolitan high-volume centers, and may increase SWT.
Given limitations to resources in a publically funded health care system, we initially explored the impact of surgical wait time (SWT) on adverse pathological outcomes [9]. Herein, we sought to further assess the impact of SWT to robot-assisted radical prostatectomy (RARP) on biochemical recurrence (BCR).
Materials and methods
Patient characteristics
After ethical review board approval, a prospectively collected robot-assisted radical prostatectomy database from two major centers in Montreal (Hôpital du Sacré Cœur de Montréal and Hôpital Saint Luc) was queried to identify all men who underwent RARP between 2006 and 2015. Due to the retrospective nature of the study formal consent is not required. All cases were performed by one of 2 fellowship trained, experienced robotic surgeons using the previously reported technique [10, 11]. Patients who underwent active surveillance (AS) (n = 117), or who were on 5-alpha reductase inhibitors (n = 11) were excluded to accurately assign patients to the correct risk category.
SWT evaluation
Time to surgery was calculated based on the difference between the date of diagnosis by trans-rectal ultrasound (TRUS) prostate biopsy and the date of surgery. Time from biopsy to robotic surgery consultation (date of RARP booking request) and from booking to actual surgery was also calculated for the overall cohort and in each D’Amico risk group. SWT was considered as a continuous variable in the whole analysis.
The primary endpoint in our analysis was biochemical recurrence (BCR), defined as two consecutive PSA ≥ 0.2 ng/dl, or salvage external beam radiation therapy and/or salvage androgen deprivation therapy. BCR-free survival was calculated using the Kaplan–Meier estimator.
The effect of delay on BCR was examined in univariable analysis (UVA) and multivariable analysis (MVA) using the Cox-regression hazard model taking into consideration known prognosticators of BCR. Subgroup analysis was further conducted for all D’Amico risk categories. All statistical tests were 2-sided; R studio software (RSudio Inc, Boston MA, USA) was used in all analyses. A p value < 0.05 was considered statistically significant.
All men were prospectively followed after radical prostatectomy every 4 months for the 1st year, then every 6 months for the 2nd year and on a yearly base thereafter. None of the included patients received adjuvant therapy before proven BCR failure.
Results
Among the identified 687 men eligible for study, after exclusions, 619 had completed demographic, clinical, pathologic, and follow-up data available. Baseline characteristics are presented in Table 1.
The mean and median follow-up was 28 and 22 months, respectively. Disease-specific (BCR-free) survival was 95.1, 86.7, and 82.4% at 1, 3, and 5 years, respectively.
SWT was significantly different among the 3 D’Amico risk groups with mean SWT of, 169.11 CI (157.02; 181.19), 150.67 CI (143.39; 157.94) and, 125.81 CI (108.82; 142.79) days for low, intermediate and high-risk groups, respectively (p < 0.001). To control for this bias, a subgroup analysis was carried on 3 groups: low, intermediate, and high-risk groups.
Upon analyzing the entire study cohort with MVA, higher pathologic Gleason score (< 0.015), ECE (< 0.013) and positive surgical margin (PSM) (< 0.001), were predictors of BCR. However, SWT did not affect BCR on MVA (p = 0.196) (Table 2).
On subgroup analysis, initially reviewing the low-risk group, SWT predicts BCR on UVA p = 0.022 HR = 0.973 (0.950; 0.996). There was no association between SWT and BCR on MVA (p = 0.086) (Table 3).
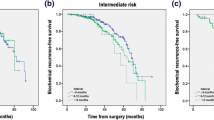
With regards to the intermediate risk group, prolonged SWT was not predictive of BCR (p = 0.991) (Table 4). Independent predictors of BCR in the intermediate-risk group were PSM (p = 0.001), and ECE (p = 0.016).
When analyzing the high-risk group SWT significantly predicts BCR on UVA (p = 0.053). SWT (p = 0.001), and PSM (p = 0.027) increase the risk of BCR (p = 0.001) on MVA (Table 5). Of note 71 patients had high-risk cancer.
Receiver operator characteristics (ROC) cut-off analysis showed a value of 90 days. This value was validated on UVA with Cox-regression model, and on MVA.
Indeed, Kaplan–Meier estimation curve was analyzed for high-risk patients above and below 90 days wait time. Comparison of both curves with likelihood test showed significant difference p = 0.03 (Fig. 1).

Kaplan–Meier plot of BCR-free survival for the high-risk group, stratified according to SWT 90 days cut-off
Discussion
The present study suggests the fact that SWT are prolonged in 2 Canadian academic centers. This fact is comparable to other reported Canadian centers, as already demonstrated in previous reports [2, 9, 12,13,14,15]. Indeed, in 2006, a Canadian consortium of experts recommended a maximum wait time of 90, 60 and 28 days in low, intermediate and high-risk prostate cancer, respectively. The present study showed that wait times largely exceed recommended consensus wait times. On the other hand, it states that it is safe to wait in low- and intermediate-risk groups far above the suggested time frame for low and intermediate risks [16].
Unique to our data is a large, contemporary patient cohort in the era of robotic surgery where a perspective on delays towards surgery in a public health care system, can be further studied. In contrast to our initial publication addressing SWT and its impact on adverse surgical pathology [9], the current study demonstrates that SWT was positively correlated to BCR for high-risk group (p = 0.001), when it exceeds 90 days.
Similar to previously reported studies on surgical delay, SWT was defined as time interval elapsing between biopsy date and surgical intervention [7, 17,18,19,20]. Furthermore, the overall SWT was divided into time from biopsy to booking (overall mean of 79.21 days) and time from booking to surgery (overall mean of 76.12 days). As it was described in an earlier study [9, 12], these time intervals are relatively long reflecting delays in multiple steps of patient management. As already discussed in our previous report on SWT and CAPRA-S pathology [9], our data demonstrate that time between biopsy and booking consult are similar in all three risk group stratification since this period is not dependent on the surgeon’s influence. However, there is a significant difference in delay from booking consult to treatment, suggesting the influence of surgeons to operate patients with higher risk faster.
In the present study, SWT did not significantly predict BCR in the overall cohort, as was the case in previous report [18, 19, 21,22,23,24]. This holds also true, for low- and intermediate-risk group, once we divided the cohort with the D’Amico risk stratification, which is also concordant with most of the previous studies [7, 22, 25,26,27].
On the other hand, two studies based on D’Amico low-risk patients found that delays greater than 6 months were associated with a significantly higher risk for BCR [8, 28].
Indeed, O’Brien demonstrated that delays above 6 months were associated with higher upgrading (47 vs 27% upstaging to Gleason score 7–10) and higher BCR rates [8]. Same cut-off (6 months) was also reported by Freedland in low-risk category and showed higher BCR rates [28]. Two other studies incorporated also intermediate risk patients and found positive association. Abern et al. analyzed intermediate risk men (D’Amico stratification) and noted that delay above 9 months was associated with higher rates of PSM and BCR [7]. A threshold of 19.2 months was defined by Holmstrom et al. to be associated with higher Gleason grade compared to immediate surgery (3.5 months). No association with BCR was found [29].
Our study strengthens the concept that it is safe to wait for low- and intermediate-risk groups, matching previous reports that found negative association of SWT with BCR.
Previous studies failed to show positive association of SWT to BCR, for high-risk patient operated of radical prostatectomy. The only study validating association of delayed wait time to BCR in high risk patient (T ≥ 2b, PSA > 10, Gleason > 6, > 34–50% positive biopsy cores) was that done by Nguyen but studied exclusively radiation therapy patients [6]. Indeed, delays above 2.5 months were found to be independent predictor of time to BCR. Three series incorporated high-risk patients and found no association [25, 26]. On the other hand, Nam et al. included high-risk patient and found positive association for overall, but also disappeared after adjustment. They concluded that negative results could be due to retrospective bias and limited number of patient [27]. The present study showed that in the high-risk group, waiting beyond 90 days to perform RARP is associated with higher BCR. This holds true after MVA. Based on our results, and in the lack of prospective reports, or retrospective reports with larger number of cases, we recommend operating on patient with high-risk disease before 90 days.
Finally, we need to shine the light on the fact that the present study as well as most of the previous ones, evaluated pathological outcomes or BCR as surrogates for CSS and OS. Only three studies evaluated the effect of wait time on CSS and OS, where no association was found [20, 29, 30].
Our study gives a unique perception on the limitations of universal health system like Canada may have on SWT. This is the first study to show positive association of SWT with BCR for patient operated exclusively by the robot. It defines a cut-off of 90 days.
Study limitations include its retrospective nature, which can include inherent selection biases. From a statistical point of view, inside the high-risk group, number of individuals was relatively limited compared to the number of variables considered. Furthermore, number of high-risk patients was relatively low compared to low- and intermediate-risk patients. We also acknowledge the fact that wait-time is partly dependent on the urologists’ preference and tried to compensate on this selection bias by stratifying the patients by the D’Amico risk groups and adjusting in multivariable analysis. Follow-up time was relatively short concerning the development of BCR especially in low- and intermediate-risk groups. It is also subject to time to event bias depending on the definition of wait time as time from biopsy to BCR.
Conclusion
In the present study, we evaluated SWT for Canadian men in a publically funded, universal healthcare system, its variation between D’Amico risk categories and impact on BCR. Based on our findings, it appears that SWT should be less than 90 days for men with high-risk disease. While surgeon case-selection appears to influence SWT, other factors also require closer evaluation to improve timing to definitive prostate cancer treatment. Further studies are warranted to validated the suggested cut-off and to assess the impact of SWT on cancer-specific survival and overall survival.
References
Canadian Cancer Society’s Advisory Committee on Cancer Statistics. Canadian Cancer Statistics 2015. Toronto, ON: Canadian Cancer Society; 2015. Google Search. https://www.google.com/search?q=google+tranlate&ie=utf-8&oe=utf-8#q=Canadian+Cancer+Society%E2%80%99s+Advisory+Committee+on+Cancer+Statistics.+Canadian+Cancer+Statistics+2015.+Toronto,+ON:+Canadian+Cancer+Society;+2015.&*. Accessed 12 March 2017
Siemens DR, Schulze KM, Mackillop WJ et al (2005) A population-based study of the waiting times for prostatectomy in Ontario. Can J Urol 12:2568–2574
Dale W, Bilir P, Han M, Meltzer D (2005) The role of anxiety in prostate carcinoma: a structured review of the literature. Cancer 104:467–478. doi:10.1002/cncr.21198
Gray RE, Fitch MI, Phillips C et al (1999) Presurgery experiences of prostate cancer patients and their spouses. Cancer Pract 7:130–135
Stevens C, Bondy SJ, Loblaw DA (2010) Wait times in prostate cancer diagnosis and radiation treatment. Can Urol Assoc J 4:243–248
Nguyen PL, Whittington R, Koo S et al (2005) The impact of a delay in initiating radiation therapy on prostate-specific antigen outcome for patients with clinically localized prostate carcinoma. Cancer 103:2053–2059. doi:10.1002/cncr.21050
Abern MR, Aronson WJ, Terris MK et al (2013) Delayed radical prostatectomy for intermediate-risk prostate cancer is associated with biochemical recurrence: possible implications for active surveillance from the SEARCH database. Prostate 73:409–417. doi:10.1002/pros.22582
O’Brien D, Loeb S, Carvalhal GF et al (2011) Delay of surgery in men with low risk prostate cancer. J Urol 185:2143–2147. doi:10.1016/j.juro.2011.02.009
Zanaty M, Alnazari M, Lawson K et al (2017) Does surgical delay for radical prostatectomy affect patient pathological outcome? A retrospective analysis from a Canadian cohort. Can Urol Assoc J 11:265–269
Valdivieso RF, Hueber P-A, Zorn KC (2013) Robot assisted radical prostatectomy: how I do it. Part I: patient preparation and positioning. Can J Urol 20:6957–6961
Valdivieso RF, Hueber P-A, Zorn KC (2013) Robot assisted radical prostatectomy: how I do it. Part II: surgical technique. Can J Urol 20:7073–7078
Saad F, Finelli A, Dranitsaris G et al (2006) Does prolonging the time to prostate cancer surgery impact long-term cancer control: a systematic review of the literature. Can J Urol 13(Suppl 3):16–24
Tran K, Sandoval C, Rahal R et al (2015) Wait times for prostate cancer treatment and patient perceptions of care in Canada: a mixed-methods report. Curr Oncol Tor Ont 22:361–364. doi:10.3747/co.22.2795
Simunovic M, Thériault M-E, Paszat L et al (2005) Using administrative databases to measure waiting times for patients undergoing major cancer surgery in Ontario, 1993–2000. Can J Surg J Can Chir 48:137–142
Simunovic M, Gagliardi A, McCready D et al (2001) A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario. CMAJ Can Med Assoc J J Assoc Med Can 165:421–425
Canadian Surgical Wait Times (SWAT) Initiative (2006) Consensus document: recommendations for optimal surgical wait times for patients with urological malignancies. Can J Urol 13(Suppl 3):62–64
Berg WT, Danzig MR, Pak JS et al (2015) Delay from biopsy to radical prostatectomy influences the rate of adverse pathologic outcomes. Prostate 75:1085–1091. doi:10.1002/pros.22992
Korets R, Seager CM, Pitman MS et al (2012) Effect of delaying surgery on radical prostatectomy outcomes: a contemporary analysis. BJU Int 110:211–216. doi:10.1111/j.1464-410X.2011.10666.x
Vickers AJ, Bianco FJ, Boorjian S et al (2006) Does a delay between diagnosis and radical prostatectomy increase the risk of disease recurrence? Cancer 106:576–580. doi:10.1002/cncr.21643
Sun M, Abdollah F, Hansen J et al (2012) Is a treatment delay in radical prostatectomy safe in individuals with low-risk prostate cancer? J Sex Med 9:2961–2969. doi:10.1111/j.1743-6109.2012.02806.x
Dall’Era MA, Cowan JE, Simko J et al (2011) Surgical management after active surveillance for low-risk prostate cancer: pathological outcomes compared with men undergoing immediate treatment. BJU Int 107:1232–1237. doi:10.1111/j.1464-410X.2010.09589.x
Van den Bergh RCN, Steyerberg EW, Khatami A et al (2010) Is delayed radical prostatectomy in men with low-risk screen-detected prostate cancer associated with a higher risk of unfavorable outcomes? Cancer 116:1281–1290. doi:10.1002/cncr.24882
Lee DK, Allareddy V, O’donnell MA et al (2006) Does the interval between prostate biopsy and radical prostatectomy affect the immediate postoperative outcome? BJU Int 97:48–50. doi:10.1111/j.1464-410X.2006.05861.x
Phillips JJ, Hall MC, Lee WR, Clark PE (2007) Does a delay in initiating definitive therapy affect biochemical recurrence rates in men with clinically localized prostate cancer? Urol Oncol 25:196–200. doi:10.1016/j.urolonc.2006.06.004
Graefen M, Walz J, Chun K-HF et al (2005) Reasonable delay of surgical treatment in men with localized prostate cancer-impact on prognosis? Eur Urol 47:756–760. doi:10.1016/j.eururo.2005.02.004
Khan MA, Mangold LA, Epstein JI et al (2004) Impact of surgical delay on long-term cancer control for clinically localized prostate cancer. J Urol 172:1835–1839
Nam RK, Jewett MAS, Krahn MD et al (2003) Delay in surgical therapy for clinically localized prostate cancer and biochemical recurrence after radical prostatectomy. Can J Urol 10:1891–1898
Freedland SJ, Kane CJ, Amling CL et al (2006) Delay of radical prostatectomy and risk of biochemical progression in men with low risk prostate cancer. J Urol 175:1298–1302. doi:10.1016/S0022-5347(05)00646-4
Holmström B, Holmberg E, Egevad L et al (2010) Outcome of primary versus deferred radical prostatectomy in the National Prostate Cancer Register of Sweden Follow-Up Study. J Urol 184:1322–1327. doi:10.1016/j.juro.2010.06.008
Andrews SF, Horwitz EM, Feigenberg SJ et al (2005) Does a delay in external beam radiation therapy after tissue diagnosis affect outcome for men with prostate carcinoma? Cancer 104:299–304. doi:10.1002/cncr.21184
Author information
Authors and Affiliations
Contributions
MZ: Project development, Data collection and management, Data analysis, Manuscript writing and editing. MA: Project development, Data collection and management. KA: Manuscript writing and editing. KL: Manuscript writing and editing. MA: Project development Manuscript editing. ER: Data collection and management. AA: Data collection and management. PAH: Project development Manuscript editing. CT: Manuscript editing. MM: Manuscript editing. FS: Project development, Manuscript editing. RP: Manuscript editing. PIK: Project development. AE-H: Project development, Data collection and management, Manuscript writing and editing. KCZ: Project development, Data collection and management, Manuscript writing and editing.
Corresponding author
Ethics declarations
Research involving human participants and/or animals
This study is a retrospective. For this type of study formal consent is not required.
Conflict of interest
All authors have no conflict of interest to declare.
Rights and permissions
About this article

Cite this article
Zanaty, M., Alnazari, M., Ajib, K. et al. Does surgical delay for radical prostatectomy affect biochemical recurrence? A retrospective analysis from a Canadian cohort. World J Urol 36, 1–6 (2018). https://doi.org/10.1007/s00345-017-2105-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-017-2105-6