
Abstract
Purpose
Prostate cancer (PCa) diagnosis relies on clinical suspicion leading to systematic transrectal ultrasound-guided biopsy (TRUSGB). Multiparametric magnetic resonance imaging (mpMRI) allows for targeted biopsy of suspicious areas of the prostate instead of random 12-core biopsy. This method has been shown to be more accurate in detecting significant PCa. However, the precise spatial accuracy of cognitive targeting is unknown.
Methods
Consecutive patients undergoing mpMRI-targeted TRUSGB with cognitive registration (MRTB-COG) followed by robot-assisted radical prostatectomy were included in the present analysis. The regions of interest (ROIs) involved by the index lesion reported on mpMRI were subsequently targeted by two experienced urologists using the cognitive approach. The 27 ROIs were used as spatial reference. Mapping on radical prostatectomy specimen was used as reference to determine true-positive mpMRI findings. Per core correlation analysis was performed.
Results
Forty patients were included. Overall, 40 index lesions involving 137 ROIs (mean ROIs per index lesion 3.43) were identified on MRI. After correlating these findings with final pathology, 117 ROIs (85 %) were considered as true-positive lesions. A total of 102 biopsy cores directed toward such true-positive ROIs were available for final analysis. Cognitive targeted biopsy hit the target in 82 % of the cases (84/102). The only identified risk factor for missing the target was an anterior situated ROI (p = 0.01).
Conclusion
In experienced hands, cognitive MRTB-COG allows for an accuracy of 82 % in hitting the correct target, given that it is a true-positive lesion. Anterior tumors are less likely to be successfully targeted.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cancer of the prostate (PCa) is now recognized as one of the most important medical issues affecting the male population. PCa is the most common solid neoplasm in Europe and in the USA [1, 2]. It is estimated that about 233,000 men were diagnosed with and 30,000 men died of PCa in 2014 in the USA. One in seven men will be diagnosed with the disease in their lifetime [3]. PCa diagnosis relies on clinical suspicion based on an abnormal digital rectal examination (DRE) and/or elevated serum PSA value, leading to transrectal ultrasound-guided, 12-core random biopsies of the prostate (TRUSGB). However, this technique has several important limitations, especially overdiagnosis of insignificant PCa and undersampling of the anterior/apical region of the prostate, which may lead to missed cancer diagnosis in up to 20 % of men with suspected PCa [4].
In view of this lack of sensitivity and specificity of standard TRUSGB, the use of multiparametric MRI of the prostate has proven useful. Indeed, when the tumor can be identified on MRI, the so-called MRI-targeted biopsy is more likely to detect cancer with fewer cores [5–8]. Indeed, macroscopic lesions visible on MRI are more likely to be targeted and more likely to harbor significant PCa. Reduced cost, decreased infection rate and diminished procedure duration represent potential consequences of using fewer cores. Moreover, MRI-targeted biopsy is less likely to detect insignificant (low volume, low grade) PCa, thus reducing the risk of overdiagnosis and potentially overtreatment of these low-risk tumors. Finally, MRI-targeted biopsy has been shown to accurately correlate with the radical prostatectomy specimen, thus reducing the risk of upgrading or upstaging on final pathology [5, 9, 10].
Despite all these advantages, MRI-targeted biopsy is not yet considered as standard [11]. So far, three targeting options are available [12]: (1) the cognitive approach which is the most widely used technique. MRI-targeted TRUSGB with cognitive registration (MRTB-COG) represents biopsies performed under TRUS guidance, using cognitive registration of prebiopsy mpMRI data, and TRUS imaging, with manual guidance to the target. The cognitive approach requires the physician performing the biopsy to review the MRI separately and cognitively register the suspected lesion location onto ultrasound volume of the prostate to guide the biopsy gun toward the appropriate target [11, 13]. Thus, the likelihood of an MRI lesion being positive for clinically significant PCa if it is targeted at biopsy depends on (a) the accuracy of MRI to detect PCa and (b) the operator’s accuracy in directing the needle toward the target during MRTB-COG; (2) fusion targeting, which uses a dedicated device and software that allow for registration of the MRI with the real-time US images. In order to fuse the MRI picture of the prostate to the real-time US image, which can be deformed because of the intrarectal probe, a registration process (rigid or elastic fusion) is needed. Corresponding landmarks are chosen manually [14]; and (3) in-bore targeting which is achieved with the use of MRI compatible biopsy material. The biopsy is performed during the MRI. While in-bore targeted biopsy has shown promising results [15], it is limited by device availability, time investment and overall and opportunity costs of magnet time [16].
While a large body of evidence suggests that the sensitivity and specificity of MRI in detecting significant PCa are high, little is known about the accuracy of the operator in hitting the target during MRTB-COG. The goal of the present study is to evaluate the accuracy of cognitive targeted biopsy in hitting true-positive MRI targets based on the correlation with the final robot-assisted radical prostatectomy (RARP) specimen.
Methods
This study was approved by the Research Ethics Committee of the Jewish General Hospital, McGill University Health Center, Montreal, Canada (study number 14–64). From October 2012 to September 2014, consecutive patients undergoing MRTB-COG of the prostate and subsequently robot-assisted radical prostatectomy (RARP) were included in the present single-center retrospective analysis. Patients in whom MRI demonstrated Likert score 3 or less suspicious lesions were excluded. If MRTB-COG was aimed toward a lesion not considered as the index lesion, this patient was excluded (Fig. 1). Patient’s characteristics including age, familial history of PCa, DRE and PSA value were tabulated in an Excel spread sheet.

Selection process and exclusion criteria
Multiparametric MRI
Four experienced abdominal imaging radiologists were involved in MRI interpretation and reporting. MRI was performed on a Philips Intera 1.5T 8.5.2 ACS scanner (Philips Medical Systems, Best, Netherlands) running software version 3.2.1.1 using the phased-array four-channel SENSE body coil, without endorectal coil, as described previously by our group [17]. Sequences were performed following injection of Buscopan (Hyoscine butyl bromide, Boehringer Ingelheim (Canada) Limited, Burlington, Ontario, Canada) 1 cc of 20 mg/cc IV as previously described. Thereafter Omniscan (Gadodiamide, GE Healthcare Canada, Mississauga, Ontario, Canada) 0.2 mmol/kg 0.5 mmol/cc to a maximum of 20 cc was injected IV and dynamic imaging performed with a 25-s delay.
Based on low signal intensity on T2-weighted images (T2 W), homogeneous early enhancement after Gadodiamide administration (DCE) and/or restricted diffusion on diffusion-weighted images (DWI)/reduced apparent diffusion coefficient (ADC), the likelihood of PCa was determined using the Likert scoring system from 1 to 5 [18]. The index lesion at MRI was defined as the largest suspicious tumor nodule with highest score. All regions of interest (ROIs) involved by the index PCa lesion were reported on MRI, together with prostate volume and index lesion size and volume. The 27 ROIs [18, 19] were used as spatial reference. Only Likert score 4–5 lesions were considered. MRI prostate volume was used to calculate PSA density.
Targeted biopsy
All biopsies were performed under local anesthesia and antibiotic prophylaxis by two experienced urologists (FB and SA) with extensive knowledge of prostatic MRI and having performed over 100 MRTB-COG. Suspicious ROIs involved by the index lesions on MRI were targeted using the cognitive approach. Based on previously published results, patients who underwent side-firing biopsy were excluded from the present analysis [17]. The number of cores per ROIs was left to the operator’s discretion. Each patient underwent between 1 and 7 targeted biopsy (median 2) following standard 12-core TRUSGB. For each target, the precise ROI that was targeted and the primary/secondary Gleason grading were recorded.
Pathology reporting
After fixed in 10 % buffered formalin, each RP specimen was processed according to the modified Stanford technique [20]. Serial cross sections of 3 mm thick were obtained from apex to base. Each specimen was included in standard blocks and submitted completely.
Three experienced uropathologists blinded to the MRI results reviewed all RARP specimens. All foci of carcinoma were traced on glass slides and transposed on the same spatial referential mapping used for MRI. The index lesion was defined as the tumor nodule with greater dimension and/or higher Gleason score. The Gleason score, dimensions and location of all tumors foci were registered. Finally, tumor localization on the specimen was manually reported on the same spatial reference used for MRI reports. PCa mapping on final pathology was used as reference to ensure that each MRI ROIs involved by the index lesion were true-positive finding. Only MRTB-COG cores directed toward such true-positive ROIs were considered. The targeted biopsy was considered as positive if cancer was found in the same targeted ROIs.
Standard descriptive statistics are reported as median (interquartile range) or mean (±SD) for continuous variables depending on the distribution and frequencies, and percentage for categorical variables. They were used for patient’s characteristics and MRI and pathology reporting. Means and standard deviations are given when not otherwise specified. For comparison of positive targets with negative ones, independent t tests or Mann–Whitney U tests were used for continuous variables. Pearson’s Chi-squared tests were used for categorical variables. For the comparison of patients in whom MRTB-COG missed the target versus those in whom ROIs involved by the MRI index lesion were successfully targeted (Table 2), Mann–Whitney U tests and Pearson’s Chi-squared tests were used for continuous and categorical variables, respectively.
Results
Overall, 155 patients underwent RARP during the study period. After applying exclusion criteria, the remaining 40 patients were included in final analysis. The study flow chart and selection process are summarized in Fig. 1. Of those, 36 (90 %) were biopsy-naïve patients and four had had previous TRUSGB in an active surveillance setting. The mean age (±SD) of the cohort was 63 ± 7 years. Mean PSA was 8.18 ± 3.54 ng/ml. Family history was positive in two patients. All other relevant patient’s characteristics are summarized in Table 1.
Multiparametric MRI revealed 17 Likert score 4 (43 %) and 23 Likert score 5 index lesions (57 %), involving 137 ROIs. Index lesions at MRI involved from 1 to 7 ROIs (mean ROIs per MRI index lesion 3.43). Mean mpMRI prostate volume was 39.17 ± 13.38 ml and was similar to the gland volume reported by TRUS (39.40 ± 12.25 ml). The mean PSA density was 0.23 ± 0.12 ng/ml2 (Table 1)
MRTB-COG was performed 71 ± 77 (range 2–329) days after the MRI. The time elapsed between MRTB-COG and RARP was 119 ± 55 (range 42–234) days.
Final pathology revealed one pT2a (2.5 %), 26 pT2c (65 %), 10 pT3a (25 %) and 3 pT3b (7.5 %) PCa, respectively. Bilateral pelvic lymph node dissection was performed in 37/40 patients (93 %). Two (5 %) were pN + (one pT3a and one pT3b). In most of the patients (25/40, 63 %) PCa were graded as Gleason 3 + 4, while Gleason >8 was found in 6/40 patients (15 %) (Table 1). Out of the 40 index lesions identified, 7 strictly involved the anterior prostate (17.5 %), while 15 (37.5 %) only involved the posterior ROIs of the prostate. The remaining 45 % of the index lesions involved both the anterior and posterior prostate. Overall, based on Epstein criteria [21], 100 % of the index lesions were considered as significant PCa. When the ROIs involved by the index tumor on final pathology were correlated with those seen on MRI (n = 137), 117 harbored PCa and were considered as true-positive lesions. Of the 102 cores targeted toward such true-positive ROIs, 84 came back positive for PCa, allowing for an accuracy of 82 % in hitting the index lesion (Fig. 2). The mean percentage of core length involved by cancer was 37 ± 26 %. The Gleason concordance rate between MRTB-COG and final RARP specimen pathology was 59/84 cores (70 %). In 21 cases (25 %), and the Gleason score was upgraded on final specimen pathology, while a downgrading was observed in 4 (5 %) patients. The maximal combined Gleason score discrepancy was 1 point. Of the 18 MRTB-COG (in 11 patients) that missed the target, 10 (56 %) were aimed at the anterior ROIs of the prostate, while 20 (24 %) were aimed toward anterior ROIs in the successful targeted group.

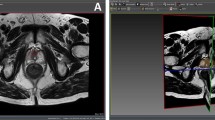
Results of a biopsy-naïve 56-year-old man with PSA of 5.8 ng/ml and a normal DRE who underwent MRGTB. a Prebiopsy MRI suggests a lesion suspicious for PCa in the anterior zone, involving ROIs 9A and 11A (A1, T2-weighted imaging; A2, dynamic contrast enhanced imaging; A3, diffusion-weighted imaging). Likert score 5/5 was given. One cognitive MRGTB targeted 9A, and another one targeted 11A. Both came back positive for Gleason 4 + 3 PCa. b The patient underwent a RARP 55 days after MRGTB. Final pathology showed a 1.5-cm Gleason 4 + 3 adenocarcinoma involving the ROIs 9A and 11A. The picture below represents a slide cut at the level of 9A with the tumor limits marked in red. c The same areas involved by PCa that were marked on the slides were then reported on the Dickinson’s ROIs drawing. In the present patient, MRGTB correlated perfectly with the final pathology
Patients in which MRTB-COG missed the target in at least one ROI (11 men) were then compared to patients in which all MRTB-COG successfully hit their target (29 men, 73 %) in order to identify risk factors for missing the target (Table 2). There was no statistical difference as far as age, PSA, PSA density, time from MRI to MRTB-COG or prostate volume were considered. No significant difference was found in Likert score 5 attributions, index lesion maximal diameter on MRI or final pathology, index lesion volume on MRI and primary Gleason 3 pattern. Anterior located ROIs was the only risk factor for missing the target [10/18 (56 %) versus 20/84 (24 %), p = 0.01] (Table 2).
Discussion
The present study demonstrates that MRTB-COG directed toward true-positive foci hit the target with 82 % accuracy. To our knowledge, this is the first study addressing this specific question. The main strength of the present analysis relies on the use of radical prostatectomy specimen as standard reference, together with the adoption of a standard spatial reference for reporting the precise location of PCa on both MRI and final pathology. The sensitivity of MRI in detecting index lesions of significant PCa (100 %) might seem high in the present study. It is obviously biased by the inclusion criteria for this study and including patients with negative MRI but positive standard 12-core biopsy who would undergo RARP would probably lower the sensitivity. This result should therefore be interpreted with caution. While the body of evidence favoring MRTB-COG versus TRUSGB is growing [5, 8], most of these studies are limited by the absence of radical prostatectomy specimens as the standard reference. Therefore, one cannot determine whether the absence of cancer on MRTB-COG is related to the inability of the operator to hit the target or whether the operator actually hit the intended target, but which turned out to be a false-positive lesion. So far, the reported accuracy of MRGTB in detecting PCa ranges between 60 and 70 % [5, 9]. However, mpMRI false-positive rates up to 15 % have been reported [22] and most studies do not report the accuracy using a spatial reference standard.
Baco et al. [23] recently reported on the accuracy of MRI-targeted biopsy using MRI-US image fusion in characterizing the index lesion. Patient’s characteristics were similar to our cohort, except that only 31 % of their patients were biopsy-naïve. As in our study, they used step-sectioned RARP specimen as standard reference. They found a 95 % concordance between index tumor location on MRI-targeted biopsy and RARP specimen and a 90 % concordance for the primary Gleason pattern. Since the authors did not consider all ROIs involved by the index lesions but rather the tumor center of the index lesion (lowest ADC value) as one target, it is difficult to extrapolate the exact ROIs spatial accuracy.
The optimal method for targeting MRI areas suspicious for PCa remains to be determined. Software-based fusion of MR images during real-time ultrasound imaging represents an alternative to MRTB-COG, which is likely to reduce operator-related variations and to increase accuracy. Puech et al. [8] compared cognitive versus MRI-US fusion targeted biopsy and found no difference in overall cancer detection rate (53 vs. 47 %, no p value given). More recently, Wysock et al. prospectively demonstrated that fusion biopsy was more often histologically informative than MRTB-COG, although overall cancer detection rate was similar (32 vs. 26.7 %, p = 0.14) [16]. Both studies were limited by the lack of radical prostatectomy specimen reference as standard. One must keep in mind that our study assessed the per core targeting accuracy, and therefore, the comparison to per MRI target statistics is limited. Our study demonstrates that, in experienced hands, MRTB-COG represents a reliable method, with an accuracy of 82 % in hitting true-positive targets. Interestingly, the only risk factor for missing the target was anterior situated lesions. This area is known to be more difficult to target and limited biopsy core length has been associated with anterior zone PCa undersampling and underdiagnosis [24, 25]. We believe that the use of image fusion of MRI with US is likely to increase the success rate and precise targeting in this region.
While the correlation between MRI and final pathology was not the primary aim of the present study, an interesting finding merits special attention. The mean largest index lesion diameter on MRI was 1.56 ± 0.82 cm. The corresponding mean largest index lesion diameter on final pathology was 2.02 ± 0.58 cm. After applying the usually accepted average linear shrinkage factor of 4.5 %, the corresponding pathological size is 2.11 cm. This observation raises the issue of underestimation of the size/volume of the index lesion, which might be of utmost importance when focal therapy is considered. Discrepancies exist when index lesion volume correlation between MRI and pathology is considered, and more studies are needed to determine the real value of MRI in treatment planning and extend of “safety” margin for focal treatments [26–28].
The issue of discrepancy between biopsy Gleason score and RARP specimen Gleason score merits special attention. Schreiber et al. [29] recently showed that the Gleason concordance rate between standard biopsy and radical prostatectomy specimen was only about 55 %. This retrospective study involved over 30,000 patients. They concluded that there continues to be significant up and downgrading from biopsy. The adoption of targeted biopsy should be able to reduce this grading migration and increase the concordance with final specimen pathology. In our study, the Gleason concordance rate was higher (59/84 cores; 70 %). In 21 cores (25 %), the Gleason score was upgraded on final specimen pathology, while a downgrading was observed on 4 (5 %) cores. No combined Gleason score discrepancy over 1 point (i.e., Gleason score 3 + 3 = 6 at biopsy and Gleason 4 + 4 = 8 at final RARP pathology) was found. We believe that although up- and downgrading remain a limitation in determining successful targeting, discrepancy of 1 point in combined Gleason score is acceptable and those were therefore considered as successful hits.
Despite the present results being encouraging, careful interpretation is needed. MRI reading and reporting were performed by four experienced uroradiologists; MRTB-COG was undertaken by two experienced urologists. Therefore, the present results might not be applicable to all centers. The fact that no central MRI review was undertaken explains the absence of interobserver variability assessment, which can be seen as a limitation. However, a concordance kappa index of 0.665 in MRI scoring system was previously reported by our group [17]. Forty patients representing 102 cores were included in the final analysis. Bias related to this highly selected small sample size cannot be excluded. The retrospective nature of this study explains the high exclusion rate. Whole-mount step-section analysis of radical prostatectomy specimen represents the gold standard in characterizing PCa. This method is not used as the standard approach in our institution, and this can be seen as a limitation. However, since no volumetric calculation was performed in this analysis, we believe that the modified Stanford represents a valid processing for tumor location and mapping.
In conclusion, given a technically adequate mpMRI which is interpreted by an experienced radiologist, an experienced physician performing a MRTB-COG targeted toward a Likert score 4–5 index lesion will hit that lesion in 100 % of the cases. When spatial accuracy based on regions of interest is taken into consideration, MRTB-COG allows for a correct sampling of 82 % of the pathologic ROIs. These encouraging results add another piece of evidence favoring MRTB-COG as a valid and accurate method to precisely detect and map PCa. Further research will aim at evaluating other targeting methods such as software fusion targeting and in-bore targeting to assess their superiority in PCa detection.
References
Boyle P, Ferlay J (2005) Cancer incidence and mortality in Europe, 2004. Ann Oncol 16(3):481–488
SEER Stat Fact Sheets: Prostate Cancer (2015) [cited; Available from: http://seer.cancer.gov/statfacts/html/prost.html
Howlader N NA, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (2013) SEER Stat Fact Sheets: Prostate. Cited; Available from: http://seer.cancer.gov/statfacts/html/prost.html#incidence-mortality
Salami SS, Ben-Levi E, Yaskiv O, Ryniker L, Turkbey B, Kavoussi LR et al (2015) In patients with a previous negative prostate biopsy and a suspicious lesion on magnetic resonance imaging, is a 12-core biopsy still necessary in addition to a targeted biopsy? BJU Int 115(4):562–570
Moore CM, Robertson NL, Arsanious N, Middleton T, Villers A, Klotz L et al (2013) Image-guided prostate biopsy using magnetic resonance imaging-derived targets: a systematic review. Eur Urol 63(1):125–140
Siddiqui MM, Rais-Bahrami S, Turkbey B, George AK, Rothwax J, Shakir N et al (2015) Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 313(4):390–397
Le JD, Stephenson S, Brugger M, Lu DY, Lieu P, Sonn GA et al (2014) Magnetic resonance imaging-ultrasound fusion biopsy for prediction of final prostate pathology. J Urol 192(5):1367–1373
Puech P, Rouviere O, Renard-Penna R, Villers A, Devos P, Colombel M et al (2013) Prostate cancer diagnosis: multiparametric MR-targeted biopsy with cognitive and transrectal US-MR fusion guidance versus systematic biopsy–prospective multicenter study. Radiology 268(2):461–469
Pokorny MR, de Rooij M, Duncan E, Schroder FH, Parkinson R, Barentsz JO et al (2014) Prospective study of diagnostic accuracy comparing prostate cancer detection by transrectal ultrasound-guided biopsy versus magnetic resonance (MR) imaging with subsequent MR-guided biopsy in men without previous prostate biopsies. Eur Urol 66(1):22–29
Siddiqui MM, Rais-Bahrami S, Truong H, Stamatakis L, Vourganti S, Nix J et al (2013) Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur Urol 64(5):713–719
Moore CM, Kasivisvanathan V, Eggener S, Emberton M, Futterer JJ, Gill IS et al (2013) Standards of reporting for MRI-targeted biopsy studies (START) of the prostate: recommendations from an international working group. Eur Urol 64(4):544–552
Marks L, Young S, Natarajan S (2013) MRI-ultrasound fusion for guidance of targeted prostate biopsy. Curr Opin Urol 23(1):43–50
Puech P, Ouzzane A, Gaillard V, Betrouni N, Renard B, Villers A et al (2014) Multiparametric MRI-targeted TRUS prostate biopsies using visual registration. BioMed Res Int 2014:819360
Logan JK, Rais-Bahrami S, Turkbey B, Gomella A, Amalou H, Choyke PL et al (2014) Current status of magnetic resonance imaging (MRI) and ultrasonography fusion software platforms for guidance of prostate biopsies. BJU Int 114(5):641–652
Bjurlin MA, Meng X, Le Nobin J, Wysock JS, Lepor H, Rosenkrantz AB et al (2014) Optimization of prostate biopsy: the role of magnetic resonance imaging targeted biopsy in detection, localization and risk assessment. J Urol 192(3):648–658
Wysock JS, Rosenkrantz AB, Huang WC, Stifelman MD, Lepor H, Deng FM et al (2014) A prospective, blinded comparison of magnetic resonance (MR) imaging-ultrasound fusion and visual estimation in the performance of MR-targeted prostate biopsy: the PROFUS trial. Eur Urol 66(2):343–351
Ploussard G, Aronson S, Pelsser V, Levental M, Anidjar M, Bladou F (2014) Impact of the type of ultrasound probe on prostate cancer detection rate and characterization in patients undergoing MRI-targeted prostate biopsies using cognitive fusion. World J Urol 32(4):977–983
Dickinson L, Ahmed HU, Allen C, Barentsz JO, Carey B, Futterer JJ et al (2011) Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur Urol 59(4):477–494
Haffner J, Lemaitre L, Puech P, Haber GP, Leroy X, Jones JS et al (2011) Role of magnetic resonance imaging before initial biopsy: comparison of magnetic resonance imaging-targeted and systematic biopsy for significant prostate cancer detection. BJU Int 108(8 Pt 2):E171–E178
Stamey TA, Freiha FS, McNeal JE, Redwine EA, Whittemore AS, Schmid HP (1993) Localized prostate cancer. Relationship of tumor volume to clinical significance for treatment of prostate cancer. Cancer 71(3 Suppl):933–938
Epstein JI, Chan DW, Sokoll LJ, Walsh PC, Cox JL, Rittenhouse H et al (1998) Nonpalpable stage T1c prostate cancer: prediction of insignificant disease using free/total prostate specific antigen levels and needle biopsy findings. J Urol 160(6 Pt 2):2407–2411
Bains LJ, Studer UE, Froehlich JM, Giannarini G, Triantafyllou M, Fleischmann A et al (2014) Diffusion-weighted magnetic resonance imaging detects significant prostate cancer with high probability. J Urol 192(3):737–742
Baco E, Ukimura O, Rud E, Vlatkovic L, Svindland A, Aron M et al (2015) Magnetic resonance imaging-transectal ultrasound image-fusion biopsies accurately characterize the index tumor: correlation with step-sectioned radical prostatectomy specimens in 135 patients. Eur Urol 67(4):787–794. doi:10.1016/j.eururo.2014.08.077
Baco E, Rud E, Ukimura O, Vlatkovic L, Svindland A, Matsugasumi T et al (2014) Effect of targeted biopsy guided by elastic image fusion of MRI with 3D-TRUS on diagnosis of anterior prostate cancer. Urol Oncol 32(8):1300–1307. doi:10.1016/j.urolonc.2014.07.014
Ukimura O, Coleman JA, de la Taille A, Emberton M, Epstein JI, Freedland SJ et al (2013) Contemporary role of systematic prostate biopsies: indications, techniques, and implications for patient care. Eur Urol 63(2):214–230
Cornud F, Khoury G, Bouazza N, Beuvon F, Peyromaure M, Flam T et al (2014) Tumor target volume for focal therapy of prostate cancer-does multiparametric magnetic resonance imaging allow for a reliable estimation? J Urol 191(5):1272–1279
Valerio M, Ahmed HU (2014) Re: tumor target volume for focal therapy of prostate cancer-does multiparametric magnetic resonance imaging allow for a reliable estimation?: F. Cornud, G. Khoury, N. Bouazza, F. Beuvon, M. Peyromaure, T. Flam, M. Zerbib, P. Legmann, N. B. Delongchamps J Urol 2014; 191: 1272–1279. J Urol 192(4):1297–1298
Turkbey B, Mani H, Aras O, Rastinehad AR, Shah V, Bernardo M et al (2012) Correlation of magnetic resonance imaging tumor volume with histopathology. J Urol 188(4):1157–1163
Schreiber D, Wong AT, Rineer J, Weedon J, Schwartz D (2015) Prostate biopsy concordance in a large population-based sample: a surveillance, epidemiology and end results study. J Clin Pathol. doi:10.1136/jclinpath-2014-202767
Ethical standard
The present study was approved by the Research Ethics Committee of the Jewish General Hospital, McGill University Health Center, Montreal, Canada (Study Number 14–64). Our study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. No informed consent was necessary for this retrospective study. Details that might disclose the identity of the subjects under study were omitted.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Yannick Cerantola and Eléonore Haberer have contributed equally to this work and are considered as co-first authors.
Franck Bladou and Maurice Anidjar have contributed equally to this work and are considered as co-last authors.
Rights and permissions
About this article

Cite this article
Cerantola, Y., Haberer, E., Torres, J. et al. Accuracy of cognitive MRI-targeted biopsy in hitting prostate cancer-positive regions of interest. World J Urol 34, 75–82 (2016). https://doi.org/10.1007/s00345-015-1588-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-015-1588-2