
Abstract
Objectives
To investigate the association between magnetic resonance imaging (MRI)-based ligamentum teres lesions (LTL) and structural hip degeneration.
Methods
Bilateral 3-T hip MRIs of participants (n = 93 [36 men]; mean age ( ± SD) 51 years ± 15.4) recruited from the community and the orthopedic clinic of a single medical center were included. Clinical and imaging data acquired included hip disability and osteoarthritis outcome scores, semi-quantitative scoring of hip osteoarthritis on MRI (SHOMRI) scores on fluid-sensitive sequences, and cartilage T1ρ/T2 compositional sequences. An MRI-based LTL scoring system, incorporating continuity, thickening, and signal intensity, ranging from 0 (normal) to 4 (complete tear) was constructed. Hip morphological features associated with LTL, based on functional or anatomical relationships to LT, were defined. Relationships between MRI-LT scores and SHOMRI, global/regional cartilage T1ρ/T2, and proposed morphological abnormalities and LTL were explored by mixed effects linear and logistic regression models.
Results
In 82 (46.1%) hips, no pain was documented; 118 (63.4%) and 68 (36.6%) hips were graded as KL-grade ≤ 1 and ≥ 2, respectively. Compared to MRI-LT score = 0 (normal), score = 4 (complete tear) revealed significantly worse subchondral bony degenerative changes for bone marrow lesions (SHOMRI-BML) and subchondral cysts (SHOMRI-sc) (p < 0.001, p = 0.015, respectively). Global acetabular T1ρ, femoral T2 were significantly increased for abnormal MRI-LT scores (p-range = 0.005–0.032). Regional analyses revealed significantly increased T1ρ/T2 in central acetabular/increased T2 in off-central femoral regions (p-range = 0.005–0.046). Pulvinar effusion-synovitis, shallow fovea, and foveal osteophytes were significantly associated with abnormal LT MRI findings (p-range = < 0.001–0.044).
Conclusion
MRI abnormalities of LT are associated with worse SHOMRI-sc/BML scores, indicative of hip osteoarthritis and higher T1ρ and T2 that differ by region. Pulvinar effusion-synovitis and changes in femoral head morphology are associated with LTL.
Clinical relevance statement
Abnormal ligamentum teres findings identified via MRI are associated with structural degenerative changes of the hip joint and alterations in acetabular and femoral cartilage compositions show spatial differences in relation to LTL.
Key Points
-
The clinical significance of common ligamentum teres lesions (LTL) on MRI is not well understood.
-
LTL identified by an MRI-based scoring system is associated with worse biomarkers, indicating more advanced degenerative hip changes.
-
Effusion-synovitis signal at pulvinar, shallow fovea capitis, and foveal osteophytes are associated with LTL on imaging.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of hip osteoarthritis (HOA) is rising, particularly in Europe and North America [1, 2]. The risk factors of HOA are not as well-investigated as in the knee and require more in-depth studies [1, 3]. The ligamentum teres (LT) supports the capsular ligaments of the hip, preventing femoral head subluxation at the extremes of the range of motion. Its tears are associated with hip microinstability and pain, especially in a traumatic setting or in the presence of synovitis [4,5,6,7]. The most common pathology of LT is partial degenerative tearing, constituting up to 88% of all tears [4, 8]. Complete tears are less common and are frequently associated with athletic endeavours, traumatic injuries, or hip dysplasia [5, 9]. Fibers of LT blend with the periosteum of fovea capitis, transverse acetabular ligament, and bony structures of the acetabular notch surrounding the cotyloid fossa and the pulvinar, a synovium-encased fibro-fatty tissue containing small vessels [4, 10,11,12]. Hip hypermobility and capsular laxity have been implicated in LT tears, especially at its femoral insertion [7, 13]. There have been numerous efforts in diagnosing and classifying LT lesions (LTL), most of which rely on surgical outcomes in symptomatic populations [10, 13,14,15]. Ligament injuries arising from ongoing repetitive trauma can lead to an array of abnormalities ranging from small interstitial tearing of collagen fibers to partial or complete disruptions of the ligament substance. This results in stretched and less taut or thick, but weak ligaments even after healing [16]. In the literature, the term “LT pathology” is often reserved for tears [7]. However, histological studies revealed that LT undergoes various degenerative ultrastructural changes which have overlapping findings in magnetic resonance imaging (MRI) [4, 7, 12, 14, 17]. On MRI, a normal LT is hypointense and homogeneous with a smooth contour and striated appearance with two or more bundles. Abnormal MRI findings of LT include: intrinsic signal alterations on T2-weighted (T2W) fat-saturated (FS) images, wavy appearance, hypertrophy and alterations in LT thickness, various degrees of discontinuity, and fraying [4, 12, 18, 19].
A better understanding of the biomechanics and internal structural changes within the hip joint is crucial for gaining insight into the etiology and progression of HOA, identifying causes that accelerate the disease, and ultimately planning potential interventions. Although showing structural and anatomical resemblance to the anterior cruciate ligament of the knee, unlike its counterpart in the knee, the role of LTL in HOA remains inadequately studied [4]. To date, there are only a few reports from the surgical literature suggesting an increased risk for cartilage lesions with LT tears [8, 20]. However, there are no detailed reports investigating the relationship of various LTL identified on imaging and their associations with hip degenerative changes. MRI could serve as a valuable tool for concurrently evaluating LTL and HOA by enabling direct assessment of LT and providing validated quantitative and semi-quantitative biomarkers for assessment of HOA [21,22,23]. Thus, the primary aim of our study was to define associations between MRI-based abnormalities of the LTL with the semi-quantitative scoring system for hip OA with MRI (SHOMRI) and femoral and acetabular cartilage compositional biomarkers of T1ρ and T2 relaxation. These metrics were employed in many prior studies and were shown to be reliable and sensitive to change [21,22,23,24]. Our secondary aim was to investigate secondary morphological hip findings that could be associated with LTL, based on its anatomy and proposed functions.
Materials and methods
Study participants
Participants were prospectively recruited from the Orthopedic clinic at the University of California San Francisco and from the community via local advertisements. This study was approved by the local Institutional Review Committee. Written informed consent was obtained from all participants. The study population was comprised of healthy controls and individuals with radiographic (Kellgren Lawrence [KL] grade < 4 in both hips, joint space > 2.5 mm) or clinically symptomatic HOA. Anteroposterior radiographs of both hips were acquired at enrollment and scored for KL grades by a senior musculoskeletal radiologist (TML) with more than 25 years of experience. Participants also answered the self-administered hip disability and outcome score (HOOS) questionnaire at enrollment indicating their clinical status [25]. Exclusion criteria included previous hip surgery, knee osteoarthritis (OA), hip trauma within the last three months, intra‐articular injection within the last six months, inflammatory arthropathy, hemochromatosis, hemoglobinopathies, or contraindication for MRI. Furthermore, participants were screened for exclusion if they had radiographic knee OA (KL grade ≥ 2), pain, disability, or limited range of motion in any other location except for the hip.
MRI acquisition
Using a 3.0-T scanner (GE Healthcare) and a 32-channel flexible surface coil (GE Healthcare) bilateral hip MRIs were obtained as described in detail previously [26]. MR imaging included coronal FS-T2W fast spin echo (FSE) (repetition time (TR)/echo time (TE) = 3000/60.0 ms; field of view [FOV] = 20 cm; slice thickness = 4.0 mm; spatial resolution = 4 × 0.39 × 0.39 mm), FS 3D-FSE IW (TR/TE = 1200/20 ms; FOV = 15.3 cm; slice thickness = 0.8 mm; spatial resolution = 0.8 × 0.25 × 0.25 mm) and 3D sagittalT1ρ/T2 magnetization-prepared angle-modulated partitioned k-space spoiled gradient echo snapshots (TSL = 0/15/30/45 ms; TE = 0, 10.4, 20.8, 41.6 ms; FOV = 14 cm; TR = 1.2 s; slice thickness = 4.0 mm; spatial resolution = 4 × 0.55 × 0.55 mm) sequences.
Assessment of direct and indirect ligamentum teres lesions on MRI
“Ligamentum teres lesion” was defined as MRI abnormalities involving LT continuity, thickness, signal intensity or combinations. Coronal FS-T2W FSE and FS-3D-FSE images with multiplanar reconstructions in three orthogonal planes were assessed by two radiologists, with eight and two years of experience (Z.A. and P.J.G.). Discordant readings were adjudicated by a musculoskeletal radiologist with > 25 years of experience (T.M.L). Ten patients were later chosen randomly after a period of > 3 months and images were re-assessed between the two observers (Z.A. and P.J.G.) for intra- and inter-reader reproducibility analysis. Each LT was assessed for its integrity, increased signal intensity, and thickness [4, 18]. Integrity was evaluated as “intact” LT (LT appearing as continuous throughout its entire course); “partial tear” (focal discontinuity or focal/diffuse thinning of LT); and “complete tear” (complete loss of LT continuity) [19]. Focal or diffuse LT thickening and abnormal signal intensity were assessed dichotomously as present or absent. LT thickening was defined as the presence of a focal or diffuse increase in its size with a tubular shape or mass effect on the adjacent pulvinar fat pad. Particular attention was paid to the magic angle artifact near the femoral attachment of LT when assessing signal alteration [4]. Next, a compound MRI score, ranging between 0 and 4, was constructed taking various combinations of the abnormal MRI findings into account (Table 1). Figure 1 demonstrates representative case examples for each score. The rationale for this step was to be able to holistically assess different scenarios of LTL encountered in MRI, which likely point out to various types and combinations of pathologies.

Examples of MRI-LT scores. Continuous LT with uniform thickness and low signal intensity (arrow) extending between fovea capitis and transverse acetabular ligament on coronal T2-weighted fat-suppressed image (a) representing MRI-LT score 0. Examples for MRI-LT score 1, indicating (b) preserved continuity but thickening (arrow in b), (c) internal signal change (arrow in c) or (d) both (arrow in d). Example of MRI-LT score 2, representing partially torn LT near (arrow) without signal or thickness changes on coronal 3D-FSE image (e). Examples of MRI-LT score 3 (f–h) with partial tear and thickening (f), signal alteration (g), or both (h). Example of MRI-LT score 4 with complete discontinuity of LT from its femoral attachment with abnormal signal intensity remnants (arrow) in its expected location (i)
Additional hip morphological findings (secondary predictors), which could be implicated in the abnormal MRI appearance of LT were defined based on their close anatomical or functional relationships to LT. On the acetabular side, LT has six attachments and surrounds and converges into the cotyloid fossa; on the femoral side, it attaches singly on the fovea capitis of the femoral head [11]. Due to the difficulty of investigating bony structures of a large acetabular surface on MR images, the effusion-synovitis signal in the pulvinar fat pad was considered as an indirect indicator that might signify LTL on non-enhanced MR images (Fig. 2a). On the femoral-side, perifoveal osteophytes (Fig. 2b), subcortical bone marrow lesions (BML) (Fig. 2c) and fovea capitis depth (Fig. 3a) were investigated. [11, 18, 27]. Fovea depth was measured as the distance from the deepest point of the fovea to the tangential line drawn connecting its anterior and posterior borders (Fig. 3a). Based on the functional theory of fluid distribution by LT within the joint, fluid signal surrounding femoral neck leading to distension at joint capsule and/ or joint recesses (joint effusion) (Fig. 2b) [28]) and synovial plicae of the hip (Weitbrecht’s retinaculae) were assessed (Fig. 2d) [29]. To explore the relationships of LTL and fovea capitis morphology and capsular laxity-joint hypermobility theory, anterior joint capsule (AJC) thickness was measured at the level of the mid-femoral neck (Fig. 3b) [4, 13]. Both measurements were performed on axial oblique reformatted 3D-FSE images, in-plane with the long axis of the femoral neck. Other secondary MRI signs were assessed dichotomously.

Effusion-synovitis signal replacing the fat planes in pulvinar (arrows) on coronal FS-T2W image (a). Perifoveal osteophytes (arrows) at the upper and lower margins of fovea capitis are shown on coronal 3D-FS-FSE image (b). The lower osteophyte is displacing the LT. The sharp contrast in signal intensity of the proximal part of the LT at this point (thin arrow) represents a magic angle artifact. Note the joint effusion distending the capsule (asterisk). Bone marrow lesion at the inferior aspect of fovea capitis (arrow) on coronal T2W image (c). Superior neck plica (Weitbrecht’s retinaculum) is shown (arrow) on coronal FS-T2W image (d)

Measurement of fovea capitis depth is depicted on the axial oblique reformatted 3D-FS-FSE image along the long axis of the femoral neck (a). Measurement of the anterior joint capsule is depicted on the same image plane and sequence in (b)
Image processing and analysis for semi-quantitative and quantitative MRI outcomes
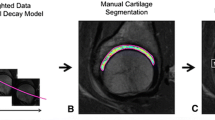
Structural changes related to HOA were assessed using SHOMRI scores in cartilage, bone marrow lesions (BML), subchondral cysts (sc), and labrum domains as described previously [22, 24]. Quantitative assessment was performed using mean femoral and acetabular cartilage T1ρ and T2 relaxation times as described previously [30]. Briefly, each voxel acquired with different TSLs or echo times was mono-exponentially fit with a Levenberg-Marquardt algorithm [31]. Cartilage surfaces were automatically segmented with a single atlas-based approach and radially divided into eight subregions [21]. The segmentation masks were applied to the T1ρ/T2 maps to isolate the voxels of interest. Mean T1ρ and T2 values were calculated across the voxels within the acetabular and femoral cartilage volumes and the eight acetabular and femoral cartilage subregions (MATLAB, The MathWorks, Inc.). Mean global and regional (five regions on femoral head, four regions on acetabular side) T1ρ/T2 measurements were obtained from articular surfaces covered by cartilage (Fig. 4).

Sub-regions of femoral and acetabular cartilage surfaces on sagittal-oblique reformatted FS-3D IW FSE‐ image. Solid arcs represent T2 relaxation times and dashed arcs represent T1ρ relaxation times. Red arcs indicate that for all MRI-LT scores > 0, there were significant increases in the respective compositional cartilage outcome. Orange arcs indicate subregions where there were significant increases in compositional cartilage outcomes for more than one type of abnormal MRI-LT score (increased signal/ and or thickening [MRI-LT score = 1] or partial/complete LT tears [MRI-LT scores = 2–3/4]. Yellow arcs indicate subregions where there were significant increases in compositional cartilage outcomes for only MRI-LT score = 2, representing partial LT tears. Gray arcs represent subregions of cartilage where no significant relationships were found between MRI-LT scores and compositional cartilage outcomes
Statistical analysis
Statistical analyses were performed using STATA version 18 software (StataCorp LP) with significance set to p < 0.05. Descriptive statistics for continuous variables were means ± standard deviation (SD) and frequencies and percentages for categorical variables. Inter- and intra-reader reproducibility were assessed by calculating weighted Cohen’s Kappa and using cluster-resampled bootstrapping with 1000 repetitions to derive a 95% CI while accounting for clustered observations (two hips per person).
Outcome variables were categorized as primary and exploratory to address potential issues arising from multiple testing. For the primary aim (assessing the relationship between LTL and semi-quantitative and quantitative MRI biomarkers of HOA), the predictors were MRI-LT scores; the primary outcome measures were SHOMRI scores, global mean acetabular and femoral T1ρand T2-relaxation times. For exploratory purposes, secondary outcome variables for aim 1 were regional T1ρ and T2-relaxation times.
For the secondary aim (assessing associations between secondary morphological hip findings that could be associated with LTL based on its anatomy and function), the predictors were binary direct MRI findings of LT (tear, abnormal signal intensity, and thickening). Outcome variables were pulvinar effusion-synovitis, osteophytes, and BML at the fovea, joint effusion, synovial plicae count, AJC thickness, and fovea depth.
Mixed effects models with continuous predictors (MRI-LT scores) and continuous outcomes were employed to test for trends. Mixed effects linear and logistic models with a random effect for participant (accounting for two hips per person) were used to assess the relationships between predictors and continuous outcomes (i.e., global mean T1ρ/T2-relaxation times) and binary outcomes (i.e., pulvinar effusion-synovitis) respectively. Adjusted mean values and beta (B)-coefficients were reported. Unstandardized beta (B) coefficients represent the magnitude and direction of the difference in a continuous outcome variable (i.e., SHOMRI scores, T1ρ/T2 measurements) for each one-unit increase in the predictor variable. The odds ratios (OR) indicate the odds that an outcome will occur given the presence of the predictor variable, compared to the odds of it occurring given its absence. All models were adjusted for age, body mass index (BMI), and sex.
Results
The cohort included 93 individuals (36 men) with a mean age and BMI of 51 ± 15.4 years (range = 23–79) and 24.3 ± 3.6 kg/m2. A total of 118 hips (63.4%) were graded as KL grade ≤ 1 and 68 hips (36.6%) as KL grade ≥ 2. According to the HOOS pain questionnaire, 82 hips (46.1%) scored 100 out of 100, indicating no pain.
Upon MR image review, one participant was diagnosed with bilateral congenital absence of the LT and excluded from analyses related to MRI-LT scores. Table 2 summarizes the descriptive statistics of direct MRI findings of LTL, hip morphological findings proposed to be secondarily implicated in LTL, MRI-LT scores, and clinical and radiological hip findings.
There were no significant associations between age, sex or BMI, and MRI-LT scores (p = 0.130, p = 0.362 and p = 0.074, respectively). Women had significantly thicker AJC (β = 0.49, [95% CI = 0.07, 0.91], p = 0.022). Joint effusion showed positive (OR = 0.087 [95% CI = 0.76, 0.98], p = 0.026) and synovial plicae count showed inverse relationships with BMI (β = −0.03, [95% CI = −0.07, −0.002], p = 0.037).
Weighted kappa for inter-rater agreement was 0.48 (p = 0.003 [95% CI = 16–79.9]). The intra-rater reliability of the composite scores revealed kappa values of 0.52 (p < 0.001 [95% CI = 21.1–83.3]) for observer 1 and of 0.54 (p < 0.001 [95% CI = 30.3–77.4]) for observer 2.
Results for primary aim: relationships between MRI-LT scores and quantitative and semiquantitative MRI outcomes
The trend analysis showed that higher MRI-LT scores were associated with greater SHOMRI scores (β = 0.89 [0.17, 1.60], p = 0.016) and higher femoral T2 values (β = 0.61 [0.13, 1.09], p = 0.013).
Mixed effects models revealed significant results for SHOMRI-BML and sc scores for MRI-LT score 4 (p < 0.001 and p = 0.015, respectively) compared to MRI-LT score 0. Mean global acetabular T1ρ values were significantly greater for all MRI-LT scores > 0. Scores indicating partial tears (2 and 3) showed significant positive associations with greater mean global femoral T2 (Table 3).
Results from post-estimation analysis for regional differences on femoral and acetabular cartilage surfaces revealed that femoral T2 was significantly greater in the posterior-inferior aspect (region 2) for MRI-LT scores > 0 (p-range: [< 0.001–0.028]). Compared to MRI-LT score = 0 (normal MRI findings), for MRI-LT scores > 0, mean acetabular T2 and T1ρ were significantly greater in the anterior-central (region 4) (p-range: [0.001–0.021]) and central (region 5) (p-range: [0.016–0.040]) regions, respectively (Fig. 4). Results for exploratory analyses are presented in the Supplementary Table.
Results for secondary aim: relationships between hip morphological findings and MRI-abnormalities of LT
The OR of having pulvinar effusion-synovitis was significantly higher with all LTL (Table 4). The OR of having foveal osteophytes was 5.5 times higher with LT tears (95% CI = 1.8, 16.3, p = 0.002). Fovea capitis depth was greater in the presence of LT thickening by 0.40 mm (95% CI = 0.01, 0.79, p = 0.044) and in the presence of LT signal abnormality by 0.45 mm (95% CI = 0.09, 0.82, p = 0.014). It was diminished by 0.46 mm (95% CI = −0.81, −0.10, p = 0.011) with LT tear.
Discussion
Using a composite scoring system that assesses the cardinal MRI features of LT, continuity, altered thickness and signal intensity, we observed that complete tears of LT are associated with worse SHOMRI-BML and SHOMRI-sc scores, indicating later stages of HOA whereas, milder forms of LTL, including various combinations of signal or thickness alterations or partial tears were linked to significantly higher mean acetabular T1ρ and mean femoral T2 relaxation times, which might reflect earlier changes in the joint cartilage surfaces before full-scale cartilage loss is evidenced. The lack of significant associations for SHOMRI-cartilage and labrum scores might be due to our relatively healthy study population. Moreover, we identified that effusion-synovitis signal at the pulvinar, foveal osteophytes and altered depth of fovea capitis were associated with abnormal LT imaging findings.
LT assessment has historically been focused on its tears [19, 32, 33]. However, histological studies confirmed overlapping abnormal MRI findings for ultrastructural changes such as hemorrhage, mucoid or fibromatous degeneration, chronic inflammatory infiltrates, osteo/chondroid metaplasia within LT [12, 17]. Thus, an intact LT may not always be entirely normal. In fact, the thickness of LT depends on its degeneration pattern [12]. In this study, in addition to LT integrity, we investigated the significance of LT thickening, which may represent hypertrophy and/ or degeneration, and increased signal, which may represent partial tear, degeneration, or synovitis. The simple and clinically adaptable composite scoring system, enables assessment of the LT holistically as it incorporates these three MRI findings, potentially bridging the gap between macroscopic findings and confounding signal changes due to microscopic alterations within the ligament ultrastructure.
Tightening of LT causes femoral head to be pulled inside the acetabulum [7, 11]. Its resection results in increased hip adduction, revealing biomechanical alterations with loss of LT functionality [34]. Perumal et al have reported a greater rate of total hip arthroplasty for patients with LT lesions compared to those without [35]. Our results imply a temporal relationship as part of a spectrum of internal derangements, where MRI-LTL scores indicative of milder LTL (MRI-LT scores 2–3) are associated with earlier HOA changes, represented by cartilage compositional alterations, whereas MRI-LTL score of 4 (complete tear), is associated with more advanced HOA, evidenced by structural subchondral bony changes. Thus, gradually diminished functionality of LT, characterized by MRI abnormalities could lead to altered biomechanics of the femoral head within the acetabular fossa.
Additionally, our results suggest that there could also be spatial differences, evidenced by regional differences in T1ρ and T2 measurements of femoral and acetabular cartilage, in various scenarios of LTL. Reports from surgical literature indicate a spatially selective distribution for cartilage lesions in patients with and without LT tears. To the best of our knowledge, there are only two prior studies investigating the regional cartilage alterations in patients with LT tears and both were carried out exclusively on patients with femoroacetabular impingement (FAI). Of these studies, Chahla et al reported higher incidences of chondral defects on femoral head at perifoveal and weight-bearing regions compared to peripheral zones [8] and Kaya et al reported cartilage lesions at anterior superior zone of acetabulum and lateral zones of femur, attributing their results to be FAI-specific [20]. Our results from a cohort more representative of the general population, support surgical literature in differential involvement of acetabular and femoral cartilage regions.
Domb et al emphasized the significance of acetabular morphology in LT tears [36]. Furthermore, in a previous cadaveric study, LT thickness was found to be associated with larger fovea depth and width and with inferior bony proliferations at the foveal margin [12]. Our results support that foveal morphology is significant in relation to LTL. We observed that fovea capitis is smaller with LT tears, which could either be an adaptive secondary remodeling or the underlying cause of LTL. In addition, osteophytes at fovea were also significantly associated with LT tears. However, we did not observe significant relationships between foveal BML and LTL, confirming previous MRA studies [19].
We found that the pulvinar effusion-synovitis, near acetabular-sided attachment of LT, is implicated in all forms of LT abnormalities (thickening, altered signal, and tear), which is a novel, complementary imaging indicator of LTL. Animal models showed that ligament failure occurs by an initial peel-off from the acetabular side, followed by avulsion from the femoral head [37]. Using MRA, Chang et al reported a large pulvinar and/or ligamentum plica in about 18%, and highlighted the significance of non-fat-suppressed images to distinguish tears of LT from ligament plicae but effusion-synovitis signal within the pulvinar in relations to LTL was not reported previously [19]. In this study, we did not see any associations for the number of plicae and LTL but there was an inverse relationship between synovial plicae number and BMI which needs further investigation. On the other hand, joint effusion was more common in patients with higher BMI which is in line with previous quantitative reports on hip effusion [38].
Hips with tears of LT have almost four times higher likelihood of being diagnosed with capsular laxity at arthroscopy [39]. Female predominance in LT tears was previously attributed to the higher frequency of joint laxity in women [8, 39]. In this study, using AJC thickness as a potential surrogate for hip hypermobility we tried to investigate these relationships. Our results indicate a thicker AJC in females by about 0.5 mm, but no significant relationships between AJC and LTL. This may result from differences in study populations where the current study is not restricted to surgical patients or it may merely reflect the limitation of AJC thickness to indicate joint laxity.
As opposed to arthroscopy-based studies, one of the strengths of this study was bilateral assessment of hips which better allowed us to study the spectrum of LT changes in a population with a wide age range. However, the lack of surgical validation of the proposed MRI-LT scoring system or histological verification of LTL constitutes a significant limitation of this study and requires further research for validation. Furthermore, reproducibility tests revealed only moderate inter-/intra-rater agreement, which emphasizes the challenge of assessing LT on MRI. In addition, we did not evaluate acetabular morphology since this was beyond the score of this study. Also, it is not possible to infer causal relationships in the cross-sectional design, thus, it is still unclear whether degenerative LT tears are the cause or the outcome of HOA. Furthermore, we might have underscored the number of plicae due to inadequate joint distension on routine MRI. Last, as this is the first study systematically investigating the significance of LTL and is thus hypothesis-forming in nature, we refrained from applying statistical adjustments for multiple comparisons, we acknowledge that our findings will require subsequent validation.
In conclusion, this proof-of-concept study indicates that increasing abnormal LT changes are associated with progressive acetabular and cartilage compositional changes, while complete LT tears are associated with subchondral changes such as bone marrow lesions and subchondral cysts in the later stages of OA assessed by SHOMRI. While these results serve to generate hypotheses and require further validation, they underscore the significance of MRI in assessing LT in HOA. Secondary MRI findings, particularly pulvinar effusion-synovitis, shallow fovea capitis, and perifoveal osteophytes are also associated with LT MRI abnormalities, which could be helpful diagnostic clues.
Abbreviations
- AJC:
-
Anterior joint capsule
- BMI:
-
Body mass index
- FS:
-
Fat-saturated
- FSE:
-
Fast spin echo
- HOA:
-
Hip osteoarthritis
- LT:
-
Ligamentum teres
- LTL:
-
Ligamentum teres lesions
- MRI:
-
Magnetic resonance imaging
- OA:
-
Osteoarthritis
- SHOMRI:
-
Scoring of hip osteoarthritis on MRI
- T2W:
-
T2-weighted
References
Fan Z, Yan L, Liu H et al (2023) The prevalence of hip osteoarthritis: a systematic review and meta-analysis. Arthritis Res Ther 25:51. https://doi.org/10.1186/s13075-023-03033-7
Fu M, Zhou H, Li Y et al (2022) Global, regional, and national burdens of hip osteoarthritis from 1990 to 2019: estimates from the 2019 Global Burden of Disease Study. Arthritis Res Ther 24:8. https://doi.org/10.1186/s13075-021-02705-6
Juhakoski R, Heliövaara M, Impivaara O et al (2009) Risk factors for the development of hip osteoarthritis: a population-based prospective study. Rheumatology 48:83–87. https://doi.org/10.1093/rheumatology/ken427
Cerezal L, Kassarjian A, Canga A et al (2010) Anatomy, biomechanics, imaging, and management of ligamentum teres injuries. Radiographics 30:1637–1651. https://doi.org/10.1148/rg.306105516
Byrd JWT, Jones KS (2004) Traumatic rupture of the ligamentum teres as a source of hip pain. Arthroscopy 20:385–391. https://doi.org/10.1016/j.arthro.2004.01.025
Phillips AR, Bartlett G, Norton M, Fern D (2012) Hip stability after ligamentum teres resection during surgical dislocation for cam impingement. HIP Int 22:329–334. https://doi.org/10.5301/HIP.2012.9250
Martin RL, McDonough C, Enseki K et al (2019) Clinical relevance of the ligamentum teres: a literature review. Int J Sports Phys Ther 14:459–467. https://doi.org/10.26603/ijspt20190459
Chahla J, Soares EAM, Devitt BM et al (2016) Ligamentum teres tears and femoroacetabular impingement: prevalence and preoperative findings. Arthroscopy 32:1293–1297. https://doi.org/10.1016/j.arthro.2016.01.045
Philippon MJ, Kuppersmith DA, Wolff AB, Briggs KK (2009) Arthroscopic findings following traumatic hip dislocation in 14 professional athletes. Arthroscopy 25:169–174. https://doi.org/10.1016/j.arthro.2008.09.013
Bardakos NV, Villar RN (2009) The ligamentum teres of the adult hip. J Bone Joint Surg Br 91-B:8–15. https://doi.org/10.1302/0301-620X.91B1.21421
Mikula JD, Slette EL, Chahla J et al (2017) Quantitative anatomic analysis of the native ligamentum teres. Orthop J Sports Med 5:232596711769148. https://doi.org/10.1177/2325967117691480
Sampatchalit S, Barbosa D, Gentili A et al (2009) Degenerative changes in the ligamentum teres of the hip: cadaveric study with magnetic resonance arthrography, anatomical inspection, and histologic examination. J Comput Assist Tomogr 33:927–933. https://doi.org/10.1097/RCT.0b013e318199d89e
O’Donnell JM, Arora M (2018) A novel and simple classification for ligamentum teres pathology based on joint hypermobility. J Hip Preserv Surg 5:113–118. https://doi.org/10.1093/jhps/hnx039
Gray AJR, Villar RN (1997) The ligamentum teres of the hip: an arthroscopic classification of its pathology. Arthroscopy 13:575–578. https://doi.org/10.1016/S0749-8063(97)90182-1
Botser IB, Martin DE, Stout CE, Domb BG (2011) Tears of the ligamentum teres: prevalence in hip arthroscopy using 2 classification systems. Am J Sports Med 39:117–125. https://doi.org/10.1177/0363546511413865
Hodgson RJ, O’Connor PJ, Grainger AJ (2012) Tendon and ligament imaging. Br J Radiol 85:1157–1172. https://doi.org/10.1259/bjr/34786470
Dehao BW, Bing TK, Young JLS (2015) Understanding the ligamentum teres of the hip: a histological study. Acta Ortop Bras 23:29–33. https://doi.org/10.1590/1413-78522015230101030
Blankenbaker DG, De Smet AA, Keene JS, del Rio AM (2012) Imaging appearance of the normal and partially torn ligamentum teres on hip MR arthrography. AJR Am J Roentgenol 199:1093–1098. https://doi.org/10.2214/AJR.12.8630
Chang CY, Gill CM, Huang AJ et al (2015) Use of MR arthrography in detecting tears of the ligamentum teres with arthroscopic correlation. Skeletal Radiol 44:361–367. https://doi.org/10.1007/s00256-014-2082-4
Kaya M, Suziki T, Minowa T, Yamashita T (2014) Ligamentum teres injury is associated with the articular damage pattern in patients with femoroacetabular impingement. Arthroscopy 30:1582–1587. https://doi.org/10.1016/j.arthro.2014.06.013
Pedoia V, Gallo MC, Souza RB, Majumdar S (2017) Longitudinal study using voxel-based relaxometry: association between cartilage T1ρ and T2 and patient reported outcome changes in hip osteoarthritis. J Magn Reson Imaging 45:1523–1533. https://doi.org/10.1002/jmri.25458
Lee S, Nardo L, Kumar D et al (2015) Scoring hip osteoarthritis with MRI (SHOMRI): a whole joint osteoarthritis evaluation system: scoring hip osteoarthritis with MRI. J Magn Reson Imaging 41:1549–1557. https://doi.org/10.1002/jmri.24722
Roach KE, Souza RB, Majumdar S, Pedoia V (2023) Local patterns in 2-year T1ρ and T2 changes of hip cartilage are related to sex and functional data: a prospective evaluation on hip osteoarthritis participants. J Magn Reson Imaging 57:1042–1053. https://doi.org/10.1002/jmri.28347
Neumann J, Zhang AL, Schwaiger BJ et al (2019) Validation of scoring hip osteoarthritis with MRI (SHOMRI) scores using hip arthroscopy as a standard of reference. Eur Radiol 29:578–587. https://doi.org/10.1007/s00330-018-5623-8
Klässbo M, Larsson E, Mannevik E (2003) Hip disability and osteoarthritis outcome score. An extension of the Western Ontario and McMaster Universities Osteoarthritis Index. Scand J Rheumatol 32:46–51. https://doi.org/10.1080/03009740310000409
Roach KE, Pedoia V, Lee JJ et al (2021) Multivariate functional principal component analysis identifies waveform features of gait biomechanics related to early‐to‐moderate hip osteoarthritis. J Orthop Res 39:1722–1731. https://doi.org/10.1002/jor.24901
Armfield DR, Towers JD, Robertson DD (2006) Radiographic and MR imaging of the athletic hip. Clin Sports Med 25:211–239, viii. https://doi.org/10.1016/j.csm.2005.12.009
Mitchell D, Rao V, Dalinka M et al (1986) MRI of joint fluid in the normal and ischemic hip. AJR Am J Roentgenol 146:1215–1218. https://doi.org/10.2214/ajr.146.6.1215
Nguyen MS, Kheyfits V, Giordano BD et al (2013) Hip anatomic variants that may mimic pathologic entities on MRI: nonlabral variants. AJR Am J Roentgenol 201:W401–W408. https://doi.org/10.2214/AJR.12.9861
Wyatt C, Kumar D, Subburaj K et al (2015) Cartilage T1ρ and T2 Relaxation Times in Patients with Mild-to-Moderate Radiographic Hip Osteoarthritis: T1ρ and T2 Relaxation Times in Hip OA. Arthritis Rheumatol 67:1548–1556. https://doi.org/10.1002/art.39074
Li X, Wyatt C, Rivoire J et al (2014) Simultaneous acquisition of T1ρ and T2 quantification in knee cartilage: repeatability and diurnal variation. J Magn Reson Imaging 39:1287–1293. https://doi.org/10.1002/jmri.24253
Cerezal L, Carro LP, Llorca J et al (2015) Usefulness of MR arthrography of the hip with leg traction in the evaluation of ligamentum teres injuries. Skeletal Radiol 44:1585–1595. https://doi.org/10.1007/s00256-015-2210-9
Datir A, Xing M, Kang J et al (2014) Diagnostic utility of MRI and MR arthrography for detection of ligamentum teres tears: a retrospective analysis of 187 patients with hip pain. AJR Am J Roentgenol 203:418–423. https://doi.org/10.2214/AJR.13.12258
Demange MK, Kakuda CMS, Pereira CAM, Sakaki MH (2007) Influence of femoral head ligament on hip mechanical function. Acta Ortop Bras 15:187–190. https://doi.org/10.1590/S1413-78522007000400002
Perumal V, Woodley SJ, Nicholson HD et al (2022) Ligamentum teres lesions are associated with poorer patient outcomes in a large primary hip arthroscopy cohort of 1935 patients. Arthrosc Sports Med Rehabil 4:e1363–e1372. https://doi.org/10.1016/j.asmr.2022.04.024
Domb BG, Martin DE, Botser IB (2013) Risk factors for ligamentum teres tears. Arthroscopy 29:64–73. https://doi.org/10.1016/j.arthro.2012.07.009
Wenger D, Miyanji F, Mahar A, Oka R (2007) The mechanical properties of the ligamentum teres: a pilot study to assess its potential for improving stability in children’s hip surgery. J Pediatr Orthop 27:408–410. https://doi.org/10.1097/01.bpb.0000271332.66019.15
Ahedi H, Aitken D, Blizzard L et al (2020) Quantification of hip effusion-synovitis and its cross-sectional and longitudinal associations with hip pain, MRI findings and early radiographic hip OA. BMC Musculoskelet Disord 21:533. https://doi.org/10.1186/s12891-020-03532-7
Lindner D, El Bitar YF, Jackson TJ et al (2014) Sex-based differences in the clinical presentation of patients with symptomatic hip labral tears. Am J Sports Med 42:1365–1369. https://doi.org/10.1177/0363546514532226
Acknowledgements
The authors wish to express their sincere gratitude to Dr. Rupsa Bhattacharjee, Dr. Misung Han and Dr. Jusuk Lee for their assistance in facilitating access to imaging information.
Funding
This study has received funding by the National Institutes of Health R01 AR069006, and K24 AR072133 grants. The corresponding author (Z.A.) received salary support from NIAMS R01-AR078917 and NIH NIAID R01 AI125080 during the course of this study and stipend support from Turkish Fulbright and TUBITAK 2219 Postdoctorate Research Scholarships during the previous year.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is T.M.L.
Conflict of interest
C.E.M. is a consultant for Amgen and Acuta Capital Partners. Z.A. has worked as a consultant for Calico Life Sciences Ltd. and is a member of the Scientific Editorial Board for European Radiology (section: musculoskeletal). T.M.L. is section editor for the musculoskeletal section of the Scientific Editorial Board for European Radiology. The authors affiliated with the Scientific Editorial Board for European Radiology did not participate in the selection nor review processes for this article. All remaining authors certify that there are no funding or commercial associations that might pose a conflict of interest related to the subject matter of this article.
Statistics and biometry
Co-authors Gabby B. Joseph and Charles E. McCulloch have kindly provided statistical advice for this manuscript.
Informed consent
Written informed consent was obtained from all subjects in this study.
Ethical approval
Institutional Review Board approval was obtained.
Study subjects or cohorts overlap
Preliminary results from this study have been presented as a poster presentation at OARSI 2023 World Congress.
Methodology
-
Retrospective
-
Cross sectional study/observational
-
Performed at one institution
Additional information
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Akkaya, Z., Giesler, P.J., Roach, K.E. et al. Ligamentum teres lesions are associated with compositional and structural hip cartilage degenerative change: region-specific cartilage degeneration. Eur Radiol (2024). https://doi.org/10.1007/s00330-024-11030-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00330-024-11030-w