
Abstract
Objectives
Amyloid deposition is considered the initial pathology in Alzheimer’s disease (AD). Personalized management requires investigation of amyloid pathology and the risk factors for both amyloid pathology and cognitive decline in the Chinese population. We aimed to investigate amyloid positivity and deposition in AD patients, as well as factors related to amyloid pathology in Chinese cities.
Methods
This cross-sectional multicenter study was conducted in Shanghai and Zhengzhou, China. All participants were recruited from urban communities and memory clinics. Amyloid positivity and deposition were analyzed based on amyloid positron emission tomography (PET). We used partial least squares (PLS) models to investigate how related factors contributed to amyloid deposition and cognitive decline.
Results
In total, 1026 participants were included: 768 participants from the community-based cohort (COMC) and 258 participants from the clinic-based cohort (CLIC). The overall amyloid-positive rates in individuals with clinically diagnosed AD, mild cognitive impairment (MCI), and normal cognition (NC) were 85.8%, 44.5%, and 26.9%, respectively. The global amyloid deposition standardized uptake value ratios (SUVr) (reference: cerebellar crus) were 1.44 ± 0.24, 1.30 ± 0.22, and 1.24 ± 0.14, respectively. CLIC status, apolipoprotein E (ApoE) ε4, and older age were strongly associated with amyloid pathology by PLS modeling.
Conclusion
The overall amyloid-positive rates accompanying AD, MCI, and NC in the Chinese population were similar to those in published cohorts of other populations. ApoE ε4 and CLIC status were risk factors for amyloid pathology across the AD continuum. Education was a risk factor for amyloid pathology in MCI. Female sex and age were risk factors for amyloid pathology in NC.
Clinical relevance statement
This study provides new details about amyloid pathology in the Chinese population. Factors related to amyloid deposition and cognitive decline can help to assess patients’ AD risk.
Key Points
• We studied amyloid pathology and related risk factors in the Chinese population.
•·The overall amyloid-positive rates in individuals with clinically diagnosed AD, MCI, and NC were 85.8%, 44.5%, and 26.9%, respectively.
• These overall amyloid-positive rates were in close agreement with the corresponding prevalence for other populations.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Alzheimer’s disease (AD) is the most common type of dementia. The prevalence of dementia and AD in the population aged 60 years or older was estimated to be 6.0% and 3.9%, respectively, in a cross-sectional study in China with a large sample size [1, 2]. Moreover, the prevalence of mild cognitive impairment (MCI), a stage between AD and normal cognition (NC), was estimated to be 15.5% in China, consistent with the estimated prevalence of 10 to 30% from several other studies [1, 3, 4]. AD and MCI share similar risk factors, such as older age, parental history of dementia, fewer years of education, smoking, hyperlipidemia, diabetes, and heart disease [1, 5, 6].
The amyloid hypothesis, supported by several studies, suggests that the accumulation of β-amyloid (Aβ) is the initial event in AD, followed by downstream tau pathology, neurodegeneration, and cognitive decline [7, 8]. Regardless of its place in the sequence, amyloid accumulation is an important biomarker of AD; the rate of amyloid positivity is high, albeit variable among studies, for individuals with AD (77 to 91%) or MCI (40 to 75%) [9,10,11]. For the population of China, a multicenter study indicated that the rates of amyloid positivity in individuals with AD and MCI were 86.8% (833/960) and 9.7% (14/144), respectively [9]. In addition, the pattern of amyloid pathology and the factors related to this pathology are unclear in China. Therefore, a cross-sectional study of amyloid positivity and deposition with a large sample size is necessary to elucidate the pathology of AD.
This large-sample study enrolled individuals from urban communities and memory clinics in China who were clinically diagnosed with NC, MCI, or AD and underwent amyloid positron emission tomography (PET) scans using [18F]florbetapir. We evaluated the rates of amyloid positivity and amyloid deposition. Furthermore, factors related to amyloid pathology and cognitive impairment, such as age, sex, education duration, and apolipoprotein E (ApoE) genotypes, were investigated by multivariate analyses [12,13,14,15,16,17,18,19,20].
Materials and methods
Participants
The community-based cohort (COMC) participants were from The Chinese Preclinical Alzheimer’s Disease Study (C-PAS). C-PAS is an observational longitudinal study conducted in Shanghai, China, starting in April 2019, as described in detail in our previous studies [21]. The clinic-based cohort (CLIC) participants were recruited by clinicians in a memory clinic. All participants were between 50 and 80 years old and were recruited from October 2018 to February 2022. The exclusion criteria included the presence of neurological or psychiatric antecedents; significant alcohol or drug abuse; MR images that exhibited structural/vascular alterations beyond what is usual for a patient’s age; diseases involving the central nervous system; and severe diseases, such as cancers. Participants with any contraindications to magnetic resonance imaging (MRI) or PET were also excluded. Neuropsychological assessments, ApoE genotyping, MRI, and PET were performed. Written informed consent was obtained from the participants or their guardians. The study was approved by the Institutional Ethics Review Board of Huashan Hospital (ethical code number: HS-KY-2017–406). The flowchart of study inclusion is shown in Fig. 1.

Flowchart of this study
Identical clinical diagnostic criteria were applied to the COMC and CLIC. The diagnosis was made by experienced neurologists on clinical grounds according to corresponding international criteria. The 2011 National Institute on Aging and Alzheimer’s Association (NIA-AA) diagnostic criteria for probable AD were used to define clinically diagnosed AD [22, 23]. Individuals without dementia were further assessed for the presence of MCI based on the method proposed by Jak and Bondi [24]. Specifically, a diagnosis of MCI was given if the participant met either of the following criteria: (1) at least one impaired cognitive domain, which means impaired scores (> 1 standard deviation (SD) below the age-corrected normative mean) on all neuropsychological tests in the same domain; (2) impaired scores (> 1 SD) in each of the three cognitive domains [25]. The participants in the NC group were all recruited from communities in Shanghai as in the study by Guo et al [26, 27]. Participants with NC were identified according to our previous study; specifically, those who did not meet the criteria for AD or MCI were identified as individuals with NC [28].
Neuropsychological assessments
All participants underwent comprehensive neuropsychological assessments in revised forms adapted for the Chinese population [29, 30]. Two global cognitive tests and six neuropsychological tests in three cognitive domains were administered. Specifically, the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment-Basic (MoCA-B) were used to assess global cognition. The long-delayed recall of the Auditory Verbal Learning Test (AVLT-LDR) and the recognition component of the AVLT were used to assess memory, the Animal Fluency Test (AFT, total score) and the 30-item Boston Naming Test (BNT, total score) were used to assess language, and the Shape Trail Test (STT) parts A and B (time to completion) were used to assess executive function [31, 32].
PET and MRI scans
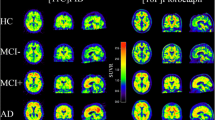
The COMC underwent [18F]florbetapir PET scans at Huashan Hospital and MRI scans at Shanghai Jiao Tong University Affiliated Sixth People’s Hospital. The automated radiosynthesis of [18F]florbetapir was performed as described in our previous report with the assistance of a local vendor [33]. The CLIC underwent [18F]florbetapir PET and MRI scans at the hospitals they visited. The methods of PET/CT and PET/MRI acquisition were similar to those used in our previous studies [34, 35]. The details are provided in Supplementary Table S1. For amyloid scans, 10 mCi (± 10%) [18F]florbetapir was injected, and a 20-min scan was performed 50 min after injection. After acquisition, the PET images were reconstructed by the filtered back-projection (FBP) algorithm (3.5 mm full width at half maximum [FWHM], Zoom 2.0) with corrections for decay, normalization, dead time, photon attenuation, scatter, and random coincidences [36]. The reconstructed brain PET image matrix size was 168 × 168 × 148, and the voxel size was 2.04 × 2.04 × 1.5 mm3. During the MRI scans, T1-weighted images were obtained with an MP-RAGE (magnetization-prepared rapid gradient echo) sequence on sagittal scans at different locations. The [18F]florbetapir PET images and T1 images of a given participant were taken within 1 month of each other.
Using the Amyvid read protocol [37] and the procedure applied in our previous study, the amyloid PET images were interpreted through visual inspection by 3 experienced raters (J.Z., F.H., and S.R.) by consensus [33]. Amyloid-positive participants, as classified by the readers, were considered to have AD (Aβ + AD) or MCI due to AD (Aβ + MCI) according to the 2018 NIA-AA research framework criteria [38].
Image processing
SPM12 (Wellcome Centre for Human Neuroimaging, https://www.fil.ion.ucl.ac.uk/spm) was used to process the [18F]florbetapir PET images. For analysis by region of interest (ROI), PET images were first coregistered to their respective T1-weighted images. All images were further converted to the normal Montreal Neurological Institute (MNI) stereotactic space by warping the images using transformation parameters. Finally, a Gaussian smoothing kernel with an 8-mm FWHM was used to smooth the images. The global cortex was defined as the sum of the following 7 ROIs: the frontal, lateral parietal, lateral temporal, medial temporal, and occipital lobes and the posterior cingulate and precuneus [39]. Then, the bilateral cerebellar crus was used as a reference area to calculate the global standardized uptake value ratios (SUVr) of [18F]florbetapir. The process for voxelwise analysis is detailed in the Supplementary material.
Statistical analysis
Fisher’s exact test was used to assess categorical demographic characteristics, and binary logistic regression was performed to analyze the rates of amyloid positivity in the different groups. For the continuous variables, analysis of covariance (ANCOVA) was used for comparisons among groups. Age, sex, education level, and ApoE ε4 allele carrier status were entered as covariates, and the significance threshold was set to p < 0.05. p values were corrected for multiple comparisons with the Benjamini and Hochberg (BH) method. We also performed a partial least squares (PLS) analysis with SIMCA P + 14.0 software (Umetrics AB) to evaluate the correlations of the risk factors with amyloid deposition, amyloid positivity, and cognition. In the PLS analysis, R2Y represents the goodness of fit, and Q2 indicates the predictive power of the model. Further details on the PLS analysis are provided in the Supplementary Information.
Results
Demographics and clinical assessments
A total of 2305 participants from communities and 557 from memory clinics were recruited. After the exclusion of 1628 participants without PET scans, 30 non-AD type dementia and 178 participants without ApoE genotype information, a total of 1026 participants were included; specifically, 768 participants from the COMC and 258 participants from the CLIC were included. A total of 246 individuals with AD, 274 individuals with MCI, and 506 individuals with NC were identified: 106 AD, 156 MCI, and 506 NC participants from the COMC as well as 140 AD and 118 MCI participants from the CLIC (Tables 1 and 2).
MCI participants (age: 65.69 ± 7.76 years) were older than NC participants (63.97 ± 8.18 years, p = 0.012). The AD group had a lower education level (8.87 ± 4.29) than the MCI (10.87 ± 3.59, p < 0.001) and NC (12.39 ± 3.30, p < 0.001) groups. The AD group had the highest proportion of ApoE ε4 carriers (122/246, 49.6%) by a significant margin, followed by the MCI (92/274, 33.6%) and NC (110/506, 21.7%, all p ≤ 0.001) groups. As expected, MMSE and MoCA-B scores were observed to be lowest in the AD group (15.96 ± 6.13, 11.51 ± 5.57) by a significant margin, followed by the MCI group (25.57 ± 3.57, 21.27 ± 4.53) and the NC group (28.07 ± 1.74, 25.50 ± 3.10; all p < 0.001). In addition, AVLT-N5/N7, AFT/BNT, and STT-A/B scores were observed to be lowest in the AD group by a significant margin, followed by the MCI group and the NC group (all p < 0.001). However, we did not observe differences in the sex ratio among these groups.
Amyloid-positive rate
Across the two cohorts, the AD group displayed the highest rate of amyloid positivity (211/246, 85.8%) by a statistically significant margin, followed by the MCI (122/274, 44.5%) and NC groups (136/506, 26.9%, all p < 0.001). In the MCI group, participants with a higher education level (> 9 years) had a higher rate of amyloid positivity than those with lower education levels (83/166, 50.0% vs. 39/108, 36.1%, p = 0.010). ApoE ε4 carriers displayed significantly higher amyloid positivity than noncarriers within the NC (40/110, 36.4% vs. 96/396, 24.2%, p = 0.014), MCI (55/92, 59.8% vs. 67/182, 36.8%, p = 0.002), and AD (114/122, 93.4% vs. 97/124, 78.2%, p = 0.002) groups. Participants from the CLIC displayed a higher rate of amyloid positivity than those from the COMC within the MCI (68/118, 57.6% vs. 54/156, 34.6%, p < 0.001) and AD groups (128/140, 91.4% vs. 83/106, 78.3%, p = 0.006). Amyloid positivity rates were not significantly different by sex or age in these three groups.
Quantification of amyloid deposition
According to the ROI-based analyses, the AD group displayed the highest global amyloid deposition by a significant margin, followed by the MCI and NC groups (global SUVr: 1.44 ± 0.24, 1.30 ± 0.22, and 1.24 ± 0.14, respectively, all p < 0.001). Individuals with clinically diagnosed AD and MCI from the COMC and CLIC had greater amyloid deposition than NC individuals (Supplementary Figure S1).
Additionally, in the clinically diagnosed groups, we observed greater amyloid deposition in females than in males in the NC group (SUVr: 1.25 ± 0.14 vs. 1.22 ± 0.14, p = 0.040. Fig. 2a). MCI individuals (SUVr: 1.32 ± 0.23 vs. 1.27 ± 0.20, p = 0.009) with a higher education level (> 9 years) displayed higher amyloid deposition than those with a lower education level (Fig. 2b). ApoE ε4 carriers had significantly higher amyloid deposition than noncarriers within the NC (SUVr: 1.27 ± 0.16 vs. 1.23 ± 0.13, p = 0.010), MCI (SUVr: 1.38 ± 0.25 vs. 1.26 ± 0.19, p < 0.001), and AD groups (SUVr: 1.48 ± 0.23 vs. 1.39 ± 0.23, p = 0.004) (Fig. 2c). Older participants (age > 65 years) had greater amyloid deposition than younger participants within the NC group (SUVr: 1.26 ± 0.16 vs. 1.22 ± 0.11, p < 0.001) (Fig. 2d). MCI (SUVr: 1.37 ± 0.25 vs. 1.25 ± 0.18, p < 0.001), Aβ + MCI (SUVr: 1.48 ± 0.27 vs. 1.37 ± 0.24, p = 0.028), and AD individuals (SUVr: 1.47 ± 0.23 vs. 1.39 ± 0.23, p = 0.012) from the CLIC displayed significantly greater amyloid deposition than those from the COMC (Figs. 2e and 4e). Significant differences were observed in most cortical areas after false discovery rate (FDR) correction at the voxel level (p < 0.05), as shown in Figure S3 by voxelwise analyses in the above groups with a significant global amyloid difference.

Influence of different related factors on global amyloid deposition in the groups. Related factors included (a) sex, (b) education level, (c) ApoE genotype, (d) age, and (e) participant cohort and influenced global amyloid deposition in individuals with clinically diagnosed NC, MCI, and AD. *, **, and *** indicate statistical significance at p ≤ 0.05, p ≤ 0.01, and p ≤ 0.001, respectively
Factors related to amyloid deposition and cognition
A PLS model was established to analyze the associations of source, age, sex, education level, and ApoE genotype with qualitative and quantitative amyloid results and global cognition in all 1026 participants. Figure 3 displays the different weights of these factors for the qualitative and quantitative amyloid results as well as cognition. Among these factors, CLIC membership, the ApoE ε4 allele, and a higher level of education were significantly associated with positive amyloid deposition (Fig. 3a, R2Y = 0.164, Q2 = 0.154). CLIC, ApoE ε4 carriers, older age, and female sex were strongly associated with the severity of amyloid deposition (Fig. 3b, R2Y = 0.170, Q2 = 0.164). Furthermore, we found that CLIC, ApoE ε4 carriers, and lower education levels were associated with low scores on the MMSE (Fig. 3c, R2Y = 0.425, Q2 = 0.421) and MoCA-B (Fig. 3d, R2Y = 0.412, Q2 = 0.407).

Factors related to amyloid pathology and cognition based on the PLS model in clinically diagnosed participants. The latent variables from the partial least squares analysis of related factors and (A) qualitative Aβ results, (B) quantitative Aβ results, (C) global cognition according to MMSE scores, and (D) global cognition according to MoCA-B scores
In Aβ + individuals, these five related factors were significantly correlated with low MMSE scores (Supplementary Fig. 2A, R2Y = 0.423, Q2 = 0.414) and low MoCA-B scores (Supplementary Fig. 2B, R2Y = 0.408, Q2 = 0.399).
Discussion
This cross-sectional study examined a large sample of urban cities in China. In this study, we found that the rates of amyloid positivity according to [18F]florbetapir PET imaging were 26.9%, 44.5%, and 85.8% in individuals with clinically identified NC, MCI, and AD, respectively. Furthermore, we investigated the factors related to amyloid pathology and cognition.
The rates of amyloid positivity in different groups were similar to those reported in a previous meta-analysis, suggesting that the mean rates of amyloid positivity in the NC, MCI, and AD groups were 24%, 53%, and 88%, respectively, in multiethnic populations outside the Chinese population [10, 11]. This means that the proportion of Aβ-positive individuals in the Chinese population is in very good agreement with corresponding prevalence estimates for other populations. This was the first study to report the rates of amyloid positivity in individuals with NC in China; the rate (26.9%) was similar to that in other countries [11, 40]. Our research provides new details about AD pathology in Chinese populations. Overall, 14.2% of clinically diagnosed AD individuals displayed amyloid negativity, which is compatible with the findings of previous investigations [41,42,43]. A previous study of the 2005–2013 National Alzheimer’s Coordinating Center autopsy database discovered that ∼14% of subjects clinically diagnosed with mild to moderate probable AD have sparse neuritic plaques or none at all, which could lead to negative amyloid PET results [44]. In a previous Chinese study, the rate of amyloid positivity in MCI individuals was 9.7%, although no quantitative amyloid deposition data were provided [9]. The researchers explained that the low positivity rate may have been caused by the clinical criteria for MCI diagnosis developed by Winblad [9, 45]. Compared to the criteria we used, the criteria mentioned by Winblad et al were relatively general [46, 47], which may explain the low rate of amyloid positivity they found in MCI patients. In the present study, MCI patients from the COMC displayed significantly lower amyloid positivity and amyloid deposition than individuals from the CLIC. The former also had higher MMSE scores than the latter (26.72 ± 1.82 vs. 24.04 ± 4.61, p < 0.001, Supplementary Table S6). Therefore, it is also important to specify the rates of amyloid positivity in MCI individuals from the community (34.6%) and those from memory clinics (57.6%), which were also significantly different in this study. However, details regarding the factors associated with amyloid deposition and cognitive impairment remain unclear in the Chinese population.
We further investigated potential factors related to amyloid deposition and cognition. First, we found no sex differences in amyloid positivity and deposition or global cognition in either the MCI group or the AD group (Fig. 2, Fig. 4, Supplementary Table S2). However, females exhibited higher amyloid deposition than males within the NC group. These findings are similar to those of a previous study [48]. The increased level of AD neuropathology among women in the NC group could be associated with pregnancy and menopause [49,50,51], as blockade of follicle-stimulating hormone was found to improve cognition by clearing amyloid and tau deposits [52]. Education is an important source of cognitive reserve that prevents or delays AD. We also found significantly better global cognitive performance with higher education levels in the NC, MCI, and AD groups (Supplementary Table S3 and Figure S4). However, individuals with higher education levels displayed higher amyloid deposition and a higher amyloid-positive rate within the MCI group. To further investigate the association between education level and AD, we used partial correlation (SPSS, version 26.0) to study the relationship between years of education and global amyloid deposition. After controlling for the influence of sex, age, ApoE, and source, individuals with higher education levels tended to have more severe amyloid deposition in the MCI and AD groups (Supplementary Figure S4A and D). In addition, after controlling for the effects of sex, age, source, and ApoE genotype, years of education had a positive association with global cognitive performance (Supplementary Figure S4). In the MCI group, individuals with 10 years of education or more had more severe amyloid deposition but better global cognition performance than those with 9 or fewer years of education. These results indicated that higher education could help individuals “cope with” AD pathology and resist cognitive decline [53, 54]. In other words, individuals with higher education compensate more effectively for cognitive deficits. According to previous research, cognitive reserve can be influenced by the interaction of innate individual differences and lifetime exposures (early-life general cognitive ability, education, occupation, physical exercise, leisure activities, social engagement, etc.) [55]. Unfortunately, this research did not obtain enough information to evaluate lifetime exposures except for education. Amyloid deposition and the amyloid-positive rate in the MCI group could be affected by these unconsidered factors. The ApoE ε4 allele is the strongest risk factor for sporadic AD and acts as a trigger for Aβ accumulation, which could increase the rate of amyloid positivity and the severity of the Aβ burden [56]. The correlation between the ApoE genotype and Aβ can be explained by the hypothesis that ApoE lowers the rate of Aβ clearance [57, 58]. As found in our study, significant differences in the rates of amyloid positivity and amyloid deposition between ε4 carriers and ε4 noncarriers were observed in the NC, MCI, and AD groups. However, global cognition did not differ between carriers and noncarriers (Supplementary Table S4). We found that the ApoE ε4 allele is the key risk factor for amyloid positivity and amyloid deposition in the Chinese population. Age is another factor related to AD in the Chinese population, as previously reported [12]. In this study, older individuals tended to display more severe amyloid deposition. This finding is in line with a previous study showing that amyloid positivity and deposition increased with age [12]. In the AD group, younger individuals displayed significantly worse global cognition (MMSE scores: 14.88 ± 6.21 vs. 17.02 ± 5.89, p = 0.027; MoCA-B scores: 10.56 ± 5.60 vs. 12.44 ± 5.40, p = 0.027) (Supplementary Table S5). This could be due to the early onset of AD [59]. Individuals with early-onset AD exhibited an aggressive disease course and accelerated rates of cognitive decline [60]. Among MCI and AD patients in this study, a higher rate of amyloid positivity and greater amyloid deposition were observed in individuals from the CLIC than in those from the COMC. Additionally, worse cognition was observed in individuals from the CLIC than in those from the COMC within both the MCI and AD groups (Supplementary Table S6). The demographic characteristics of the COMC and CLIC groups were well balanced except for the proportion of ε4 carriers in the MCI group (Supplementary Table S7). Among individuals with MCI, the CLIC group contained a higher proportion of ε4 carriers than the COMC group (40.7% vs. 28.2%, p = 0.039). Within both the AD and MCI groups, the individuals in the CLIC displayed poorer global cognition performance and more severe amyloid deposition than the individuals in the COMC (Supplementary Table S7). Within the MCI group, individuals in the CLIC displayed poorer global cognition performance and more severe amyloid deposition than those in the COMC, which may be correlated with the larger proportion of ε4 carriers in the CLIC group. Existing literature indicates that individuals from the clinic have more Alzheimer’s pathology than individuals from the community [61]. As discussed in the literature, medical help seeking can be triggered or facilitated by multiple factors, including worry associated with a family history of dementia, low quality of life, poor physical health, and socioeconomic barriers (high cost/low access to health care). Help seeking might also be influenced by individuals’ knowledge, causal beliefs, and attitudes regarding memory function, aging, and dementia. In addition, Hu et al demonstrated that clinic-based patients had higher rates of dementia and AD than community-based patients within MCI populations, which could lead to poorer global cognition performance and more severe amyloid pathology [62]. Other risk factors leading to poorer cognitive performance and more severe amyloid deposition remain unidentified in this study.

Influence of different related factors on global amyloid deposition in the groups. Related factors included a sex, b education level, c ApoE genotype, d age, and e participant cohort; these factors influenced the amounts of global amyloid deposition in Aβ-positive (Aβ +) individuals with MCI due to AD (Aβ + MCI) and those with clinical AD (Aβ + AD). *, **, and *** indicate statistical significance at p ≤ 0.05, p ≤ 0.01, and p ≤ 0.001, respectively
We also constructed PLS models to investigate the contribution of related factors to amyloid deposition and cognitive decline in the overall cohort and in participants with AD pathology. First, CLIC membership and ApoE ε4 carrier status were strongly related to an increased rate of amyloid positivity and increased amyloid deposition. CLIC membership, ApoE ε4 carrier status, and low education levels were associated with global cognitive decline. A similar pattern was found in participants with AD pathology. Thus, the model elucidated the importance of the ApoE ε4 allele and CLIC membership as factors associated with amyloid deposition and cognitive decline in the Chinese population. These results have important clinical implications for the development of an early warning model for Aβ in the Chinese population.
This study had several limitations. First, we only included urban regions; rural regions were not included due to limited access to amyloid PET. Second, only 5 related factors were analyzed; other related factors, such as parental history of dementia, medical history, lifetime exposures and lifestyle variable, were not investigated. Third, according to a study conducted on other populations, there might be more than one typical pattern of amyloid pathology [63, 64]. In this cross-sectional baseline study, we did not explore other patterns of amyloid deposition through different models. Thus, future studies should incorporate more risk factors for AD and explore other patterns of amyloid deposition through longitudinal follow-up in the Chinese population.
In conclusion, we described the rate of amyloid positivity and quantified amyloid deposition in city-dwelling individuals in China according to the AD spectrum. We found that individuals in the CLIC and those with the ApoE ε4 allele, as well as MCI individuals with more education, displayed a higher amyloid-positive rate. Sex, education level, ApoE ε4 carrier status, age, and CLIC membership were also associated with more severe amyloid deposition. Specifically, in a PLS model, CLIC, ApoE ε4 and older age were strongly associated with amyloid pathology in individuals. In summary, ApoE ε4 carrier status and CLIC membership were risk factors for amyloid pathology across the AD continuum. In MCI participants, a higher education level was also a risk factor. In the NC group, the risk factors for amyloid pathology included female sex and age.
Abbreviations
- AD:
-
Alzheimer’s disease
- AFT:
-
Animal fluency test
- ANCOVA:
-
Analysis of covariance
- ApoE :
-
Apolipoprotein E
- AVLT-LDR:
-
Long-delayed recall of the Auditory Verbal Learning Test
- Aβ:
-
β-Amyloid
- BH:
-
Benjamini and Hochberg
- BNT:
-
Boston Naming Test
- CLIC:
-
Clinic-based cohort
- COMC:
-
Community-based cohort
- CT:
-
Computed tomography
- FBP:
-
Filtered back-projection
- FDR:
-
False discovery rate
- FWHM:
-
Full width at half maximum
- MCI:
-
Mild cognitive impairment
- MMSE:
-
Mini-Mental State Examination
- MNI:
-
Montreal Neurological Institute
- MoCA-B:
-
Montreal Cognitive Assessment-Basic
- MP-RAGE:
-
Magnetization-prepared rapid gradient echo
- MRI:
-
Magnetic resonance imaging
- NC:
-
Normal cognition
- NIA-AA:
-
National Institute on Aging and Alzheimer’s Association
- PET:
-
Positron emission tomography
- PLS:
-
Partial least squares
- PVC:
-
Partial volume error correction
- ROI:
-
Region of interest
- SD:
-
Standard deviation
- STT:
-
Shape Trail Test
- SUVr:
-
Standardized uptake value ratio
References
Jia L, Du Y, Chu L et al (2020) Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health 5:e661–e671
Kern S, Zetterberg H, Kern J et al (2018) Prevalence of preclinical Alzheimer disease: comparison of current classification systems. Neurology 90:e1682–e1691
Ding D, Zhao Q, Guo Q et al (2015) Prevalence of mild cognitive impairment in an urban community in China: a cross-sectional analysis of the Shanghai Aging Study. Alzheimers Dement 11:300-309.e302
Jia J, Zhou A, Wei C et al (2014) The prevalence of mild cognitive impairment and its etiological subtypes in elderly Chinese. Alzheimers Dement 10:439–447
Silva MVF, Loures CMG, Alves LCV, de Souza LC, Borges KBG, Carvalho MDG (2019) Alzheimer’s disease: risk factors and potentially protective measures. J Biomed Sci 26:33
Day GS, Cruchaga C, Wingo T, Schindler SE, Coble D, Morris JC (2019) Association of acquired and heritable factors with intergenerational differences in age at symptomatic onset of Alzheimer disease between offspring and parents with dementia. JAMA Netw Open 2:e1913491
Jack CR Jr, Holtzman DM (2013) Biomarker modeling of Alzheimer’s disease. Neuron 80:1347–1358
Bateman RJ, Xiong C, Benzinger TLS et al (2012) Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N Engl J Med 367:795–804
Shi Z, Fu LP, Zhang N et al (2020) Amyloid PET in dementia syndromes: a Chinese multicenter study. J Nucl Med 61:1814–1819
Ossenkoppele R, Jansen WJ, Rabinovici GD et al (2015) Prevalence of amyloid PET positivity in dementia syndromes: a meta-analysis. JAMA 313:1939–1949
Jansen WJ, Ossenkoppele R, Knol DL et al (2015) Prevalence of cerebral amyloid pathology in persons without dementia: a meta-analysis. JAMA 313:1924–1938
Braak H, Braak E (1997) Frequency of stages of Alzheimer-related lesions in different age categories. Neurobiol Aging 18:351–357
Iadanza MG, Jackson MP, Hewitt EW, Ranson NA, Radford SE (2018) A new era for understanding amyloid structures and disease. Nat Rev Mol Cell Biol 19:755–773
Yasuno F, Kazui H, Morita N et al (2015) Low amyloid-beta deposition correlates with high education in cognitively normal older adults: a pilot study. Int J Geriatr Psychiatry 30:919–926
Rentz DM, Locascio JJ, Becker JA et al (2010) Cognition, reserve, and amyloid deposition in normal aging. Ann Neurol 67:353–364
Wada M, Noda Y, Shinagawa S et al (2018) Effect of education on Alzheimer’s disease-related neuroimaging biomarkers in healthy controls, and participants with mild cognitive impairment and Alzheimer’s disease: a cross-sectional study. J Alzheimers Dis 63:861–869
Rawlings AM, Sharrett AR, Mosley TH, Wong DF, Knopman DS, Gottesman RF (2019) Cognitive reserve in midlife is not associated with amyloid-beta deposition in late-life. J Alzheimers Dis 68:517–521
Lim YY, Kalinowski P, Pietrzak RH et al (2018) Association of beta-amyloid and apolipoprotein E epsilon4 with memory decline in preclinical Alzheimer disease. JAMA Neurol 75:488–494
Mattsson N, Zetterberg H, Hansson O et al (2009) CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA 302:385–393
Serrano-Pozo A, Qian J, Monsell SE, Betensky RA, Hyman BT (2015) APOEepsilon2 is associated with milder clinical and pathological Alzheimer disease. Ann Neurol 77:917–929
Cui L, Huang L, Pan FF et al (2023) Chinese preclinical Alzheimer’s disease study (C-PAS): design and challenge from PET acceptance. J Prev Alzheimers Dis 10:571–580
Edmonds EC, Delano-Wood L, Galasko DR, Salmon DP, Bondi MW (2015) Subtle cognitive decline and biomarker staging in preclinical Alzheimer’s disease. J Alzheimers Dis 47:231–242
McKhann GM, Knopman DS, Chertkow H et al (2011) The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7:263–269
Jak AJ, Bondi MW, Delano-Wood L et al (2009) Quantification of five neuropsychological approaches to defining mild cognitive impairment. Am J Geriatr Psychiatry 17:368–375
Pan FF, Huang L, Chen KL, Zhao QH, Guo QH (2020) A comparative study on the validations of three cognitive screening tests in identifying subtle cognitive decline. BMC Neurol 20:78
Huang Y, Pan FF, Huang L, Guo Q (2023) The value of clock drawing process assessment in screening for mild cognitive impairment and Alzheimer’s dementia. Assessment 30:364–374
Huang Y, Li Y, Xie F, Guo Q (2022) Associations of plasma phosphorylated tau181 and neurofilament light chain with brain amyloid burden and cognition in objectively defined subtle cognitive decline patients. CNS Neurosci Ther 28:2195–2205
Ren S, Li J, Huang L et al (2023) Brain functional alterations and association with cognition in people with preclinical subjective cognitive decline and objective subtle cognitive difficulties. Neuroscience 513:137–144
Ding D, Zhao Q, Guo Q et al (2016) Progression and predictors of mild cognitive impairment in Chinese elderly: a prospective follow-up in the Shanghai Aging Study. Alzheimers Dement 4:28–36
Guo Q, Zhao Q, Chen M, Ding D, Hong Z (2009) A comparison study of mild cognitive impairment with 3 memory tests among Chinese individuals. Alzheimer Dis Assoc Disord 23:253–259
Zhao Q, Guo Q, Hong Z (2013) Clustering and switching during a semantic verbal fluency test contribute to differential diagnosis of cognitive impairment. Neurosci Bull 29:75–82
Zhao Q, Guo Q, Liang X et al (2015) Auditory verbal learning test is superior to rey-osterrieth complex figure memory for predicting mild cognitive impairment to Alzheimer’s disease. Curr Alzheimer Res 12:520–526
Ren S, Pan Y, Li J et al (2023) The necessary of ternary amyloid classification for clinical practice: an alternative to the binary amyloid definition. View. https://doi.org/10.1002/viw.20220080
Su J, Huang Q, Ren S et al (2019) Altered brain glucose metabolism assessed by (18)F-FDG PET imaging is associated with the cognitive impairment of CADASIL. Neuroscience 417:35–44
Huang Q, Ren S, Jiang D et al (2019) Changes in brain glucose metabolism and connectivity in somatoform disorders: an 18F-FDG PET study. Eur Arch Psychiatry Clin Neurosci 270:881–891
Razifar P, Sandstrom M, Schnieder H et al (2005) Noise correlation in PET, CT, SPECT and PET/CT data evaluated using autocorrelation function: a phantom study on data, reconstructed using FBP and OSEM. BMC Med Imaging 5:5
Lilly E Full prescribing information. Available via https://pi.lilly.com/us/amyvid-uspi.pdf. Accessed 05/2023
Jack CR Jr, Bennett DA, Blennow K et al (2018) NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement 14:535–562
Wang J, Wang M, Ren S et al (2023) The effect of gender and APOE ɛ4 status on brain amyloid-β deposition in different age groups of mild cognitively impaired individuals: a PET-CT study. J Alzheimers Dis 94:763–775
Jansen WJ, Janssen O, Tijms BM et al (2022) Prevalence estimates of amyloid abnormality across the Alzheimer disease clinical spectrum. JAMA Neurol 79:228–243
Crary JF, Trojanowski JQ, Schneider JA et al (2014) Primary age-related tauopathy (PART): a common pathology associated with human aging. Acta Neuropathol 128:755–766
Serrano-Pozo A, Qian J, Monsell SE et al (2014) Mild to moderate Alzheimer dementia with insufficient neuropathological changes. Ann Neurol 75:597–601
Barkhof F, Polvikoski TM, van Straaten EC et al (2007) The significance of medial temporal lobe atrophy: a postmortem MRI study in the very old. Neurology 69:1521–1527
Beekly DL, Ramos EM, Lee WW et al (2007) The National Alzheimer’s Coordinating Center (NACC) database: the Uniform Data Set. Alzheimer Dis Assoc Disord 21:249–258
Winblad B, Palmer K, Kivipelto M et al (2004) Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med 256:240–246
Wong CG, Thomas KR, Edmonds EC et al (2018) Neuropsychological criteria for mild cognitive impairment in the framingham heart study’s old-old. Dement Geriatr Cogn Disord 46:253–265
Bondi MW, Edmonds EC, Jak AJ et al (2014) Neuropsychological criteria for mild cognitive impairment improves diagnostic precision, biomarker associations, and progression rates. J Alzheimers Dis 42:275–289
Buckley RF, Mormino EC, Rabin JS et al (2019) Sex differences in the association of global amyloid and regional tau deposition measured by positron emission tomography in clinically normal older adults. JAMA Neurol 76:542–551
Ferretti MT, Iulita MF, Cavedo E et al (2018) Sex differences in Alzheimer disease - the gateway to precision medicine. Nat Rev Neurol 14:457–469
Russell JK, Jones CK, Newhouse PA (2019) The role of estrogen in brain and cognitive aging. Neurotherapeutics 16:649–665
Schupf N, Lee JH, Pang D et al (2018) Epidemiology of estrogen and dementia in women with Down syndrome. Free Radic Biol Med 114:62–68
Xiong J, Kang SS, Wang Z et al (2022) FSH blockade improves cognition in mice with Alzheimer’s disease. Nature 603:470–476
Zhu W, Li X, Li X et al (2021) The protective impact of education on brain structure and function in Alzheimer’s disease. BMC Neurol 21:423
Stern Y (2012) Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol 11:1006–1012
Stern Y, Arenaza-Urquijo EM, Bartres-Faz D et al (2020) Whitepaper: defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement 16:1305–1311
Serrano-Pozo A, Das S, Hyman BT (2021) APOE and Alzheimer’s disease: advances in genetics, pathophysiology, and therapeutic approaches. Lancet Neurol 20:68–80
Deane R, Sagare A, Hamm K et al (2008) apoE isoform-specific disruption of amyloid beta peptide clearance from mouse brain. J Clin Invest 118:4002–4013
Castellano JM, Kim J, Stewart FR et al (2011) Human apoE isoforms differentially regulate brain amyloid-beta peptide clearance. Sci Transl Med 3:89ra57
Bertram L, Tanzi RE (2008) Thirty years of Alzheimer’s disease genetics: the implications of systematic meta-analyses. Nat Rev Neurosci 9:768–778
Cho H, Seo SW, Kim JH et al (2013) Amyloid deposition in early onset versus late onset Alzheimer’s disease. J Alzheimers Dis 35:813–821
Perrotin A, La Joie R, de La Sayette V et al (2017) Subjective cognitive decline in cognitively normal elders from the community or from a memory clinic: differential affective and imaging correlates. Alzheimers Dement 13:550–560
Hu C, Yu D, Sun X, Zhang M, Wang L, Qin H (2017) The prevalence and progression of mild cognitive impairment among clinic and community populations: a systematic review and meta-analysis. Int Psychogeriatr 29:1595–1608
Collij LE, Salvadó G, Wottschel V et al (2022) Data‐driven evidence for three distinct patterns of amyloid‐β accumulation. Alzheimers Dement 17(S4):e055417
Collij LE, Salvadó G, Wottschel V et al (2022) Spatial-temporal patterns of β-amyloid accumulation: a subtype and stage inference model analysis. Neurology 98:e1692–e1703
Acknowledgements
The authors thank Jianfei Xiao, Xiangqing Xie, Yue Qian, and Zhiwei Pan for their generous assistance with this study.
Funding
This study has received funding by the National Key R&D Program of China (2016YFC1306305, 2018YFE0203600); STI2030-Major Projects (2022ZD0213800); the National Science Foundation of China (81801752, 81571345); the Shanghai Sailing Program (18YF1403200, 19YF1405300); the startup fund of Huashan Hospital, Fudan University (2017QD081); Shanghai Municipal Key Clinical Specialty (shslczdzk03402); Shanghai Municipal Science and Technology Major Project (No. 2018SHZDZX01); and Shanghai Rising-Star Program (21QA1405800) and ZJLab.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Guarantor
The scientific guarantor of this publication is Fang Xie.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Ethical approval
Institutional Review Board approval was obtained. This study has been approved by the Institutional Review Board of Huashan Hospital, Fudan University.
Study subjects or cohorts overlap
Some study subjects or cohorts have not been previously reported.
Methodology
• retrospective
• cross sectional study
• multicenter study
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
He, K., Li, B., Huang, L. et al. Positive rate and quantification of amyloid pathology with [18F]florbetapir in the urban Chinese population. Eur Radiol 34, 3331–3341 (2024). https://doi.org/10.1007/s00330-023-10366-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-023-10366-z