
Abstract
Objectives
To introduce efficient stereological approaches for estimating the volume of a normal or enlarged spleen from MDCT.
Methods
All study participants underwent an abdominal MDCT. The first group included 20 consecutive patients with splenomegaly and the second group consisted of 20 subjects with a normal spleen. Splenic volume estimations were performed using the stereological point counting method. Stereological assessments were optimized using the systematic slice sampling procedure. Planimetric measurements based on manual tracing of splenic boundaries on each slice were taken as reference values.
Results
Stereological analysis using five to eight systematically sampled slices provided enlarged splenic volume estimations with a mean precision of 4.9 ± 1.0 % in a mean time of 2.3 ± 0.4 min. A similar measurement duration and error was observed for normal splenic volume assessment using four to seven systematically selected slices. These stereological approaches slightly but insignificantly overestimated the volume of a normal and enlarged spleen compared to planimetry (P > 0.05) with a mean difference of −1.3 ± 4.3 % and −2.7 ± 5.2 %, respectively. The two methods were highly correlated (r ≥ 0.96). The variability of repeated stereological estimations was below 3.8 %.
Conclusions
The proposed stereological approaches enable the rapid, reproducible, and accurate splenic volume estimation from MDCT data in patients with or without splenomegaly.
Key Points
• New efficient stereological approaches are proposed for spleen volumetry from MDCT
• These volumetric approaches are applicable in patients with or without splenomegaly
• Stereological splenic volume estimations from MDCT are rapid, reproducible, and accurate
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The presence of splenomegaly, which is an enlargement of the spleen, is associated with several conditions including infectious, haematological, congestive, inflammatory, storage, and malignant diseases [1]. The quantitative assessment of the splenic size is often required for the treatment and follow-up of patients with these disorders. Physical examination using palpation is subjective, dependent upon the degree of enlargement [1], and it might lead to unreliable results [2]. The size of the spleen is currently evaluated in vivo using radiological modalities. Computed tomography (CT) and ultrasound (US) are currently considered the main modalities for routine splenic imaging in clinical practice [1, 3]. Previous studies have reported a reasonable to good correlation between sonographic splenic volume assessments and the true volume of resected spleens [4, 5]. However, volumetry using two-dimensional US is often restricted by the incomplete depiction of the entire spleen due to overlying structures [6], whereas three-dimensional US occasionally underestimates the volume of large spleens exceeding 500 cm3 [7]. Sonographic analysis is also dependent upon the operator’s experience and performance. CT provides detailed and reliable information about the spleen and surrounding structures and it is more reproducible than US [1]. The good agreement between CT-based splenic volume measurements before splenectomy with the true organ volume determined by water displacement has indicated the high accuracy of this modality [8].
The modern design stereology enables the direct organ volume estimation on cross-sectional images through the simple process of point counting [9]. The method gives volume assessments with a known precision without the requirement for image segmentation. The stereology has been successfully combined with CT data for estimating the lung [10], bladder [11], liver [12], and heart volume [13]. Moreover, it has been employed to quantify severe head injuries [14] and intra-abdominal haemorrhage [15] from CT. To the best of our knowledge, there is no reported experience regarding the stereological splenic volume estimation using conventional or multidetector computed tomography (MDCT). Advanced volumetric methods relied on the selection either of points [16] or of randomly marked voxels [17] have been solely applied on magnetic resonance images to determine normal splenic size.
The objective of the current study was to introduce efficient stereological approaches for estimating the volume of a normal or enlarged spleen from MDCT images.
Materials and methods
MDCT examinations
The first group of study participants consisted of 20 consecutive patients (nine males, 11 females) with splenomegaly diagnosed by abdominal MDCT examinations. The scanning was performed for the evaluation of infections, hematological diseases, hepatic disorders, and abdominal masses. The mean age of these patients was 54.4 ± 9.4 years. The second group also involved 20 consecutive subjects (10 men, 10 women) with normal spleens as confirmed by MDCT data. These subjects did not exhibit any pathology that may influence the splenic size, and their mean age was 65.0 ± 13.1 years. They were referred for MDCT in order to evaluate primary or metastatic malignancies, abdominal pain, inflammatory diseases, bowel obstruction, and infections. Written informed consent was obtained by each participant prior to scanning.
The patients’ examinations were performed on a 16-MDCT unit (Somatom Sensation 16, Siemens Medical Solutions, Forcheim, Germany). Abdominal imaging was performed using 120 kV and 160 effective mAs. The MDCT data were acquired during a single breath-hold and covered the entire region of the abdomen including the spleen. Volumetric analysis was performed on contrast-enhanced axial images. The reconstructed slice thickness was 8 mm without any slice gap. Ninety milliliters of iodinated contrast material was administered intravenously with a flow rate of 2.7 ml/s. These MDCT images were transferred to a Windows personal computer for both planimetric and stereological volume estimations with the aid of the Analyze software version 3.1 (Biomedical Imaging Resource, Mayo Foundation, Rochester, MN, USA).
Planimetric volume estimations
The splenic boundaries of all patients with or without splenomegaly were manually delineated on a slice-by-slice basis. The contouring procedure was performed by a user with more than 8 years of experience in organ volume measurements using the conventional method of manual planimetry. The user had detailed knowledge of the cross-sectional anatomy of the abdomen. The software automatically calculated the area of the spleen encompassed by the manually defined contours on each MDCT slice. The sum of these calculated areas multiplied by the reconstructed slice thickness provided the total volume of the spleen.
Stereological volume estimations
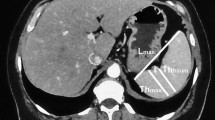
Stereological estimations were performed by overlaying the MDCT images with a systematic square grid of test points (Fig. 1a). The counting grid was placed and oriented at random on the first slice depicting the spleen of each patient. The grid orientation remained stable for all subsequent slices crossing the region of interest. The user selected all points hitting the spleen by simply moving the cursor over the region of interest and holding down the left mouse button. The button release automatically stopped the process and the number of selected points on each slice was recorded by the software. The total splenic volume (V) was automatically calculated by the software program using the following formula:

A systematic square grid of test points is randomly placed on an abdominal MDCT image for normal splenic volume estimation using either (a) the entire slice set depicting the spleen, or samples with every (b) second and (c) third slice containing the organ of interest. The distance d between the test points is equal to (a) 12.9 mm, (b) 9.1 mm, and (c) 7.5 mm
where T is the distance between two consecutive slices, d is the distance between the test points of the grid, P i is the number of counted points on a slice i, and m is the total number of slices imaging the spleen. The quantity d 2 in Eq. 1 denotes the area of each test point.
The precision of each stereological volume estimation was determined by its coefficient of error (CE). The CE was found by the following equation proposed by Cruz-Orive [18]:
where B is the mean splenic boundary length and A is mean area of the spleen. The fraction \( \left(B/\sqrt{A}\right) \), known as shape coefficient, was previously found to be 4.3 for a normal spleen [16]. The above value was inserted into Eq. 2 to find the CE of the stereological assessments of the normal splenic volume. The shape coefficient was also determined for the first nine patients with splenomegaly. The quantity A was found using the point counting process whereas B was determined by counting the number of intersections between splenic borders and a square grid of test lines [10]. Both grids with test points and test lines were randomly placed on the MDCT images. The mean shape coefficient was equal to 4.4. This value was adopted to find the CE associated with the volumetric estimations in patients with splenomegaly.
The distance between the test points of the grid was calculated using the following equation:
where V is an approximation of the mean splenic volume [10, 19]. The above equation secures that the volume of the organ of interest may be estimated with 150 point counts. This total number of counted points is usually sufficient for volumetry of structures with a wide variety of shapes [20]. By assuming a typical normal splenic volume of 200 cm3, the distance d was found to be 12.9 mm for a T equal to 8 mm. The corresponding d value for the group of patients with splenomegaly was 25.0 mm by considering an average volume of 750 cm3 for an enlarged spleen. The above distances between the test points of the grid were used for volume estimations using the total number of slices showing the spleen.
Systematic slice sampling procedure
The stereological method enables the assessment of any organ volume together with its CE by using only a sample of slices containing the organ of interest. Previous studies have indicated the efficiency of systematic slice sampling for volumetric analysis [11, 21]. The sampling procedure was made in order to define the optimal stereological approach for estimating the volume of a normal or enlarged spleen. This optimal approach should involve the minimum number of systematically sampled MDCT slices required to provide acceptable volume assessments with the minimum user intervention. Gundersen and Jensen [21] reported that a CE of 5 % is sufficient in stereological studies.
For the group of patients with splenomegaly, stereological volume estimations were obtained by using sampling intensities of 1/2, 1/3, 1/4, 1/5, and 1/6. The systematic slice sampling procedure may be illustrated in a randomly selected patient with splenomegaly. Let’s consider the entire slice set that depicts the enlarged spleen of patient no. 6 and consists of 19 contiguous MDCT slices numbered {1, 2,…, 18, 19}. The adoption of a sampling intensity of 1/3 implied that three samples having six to seven MDCT slices could be systematically drawn from the initial set of images. The first, second, and third samples consisted of the slices {1, 4, 7, 10, 13, 16, 19}, {2, 5, 8, 11, 14, 17}, and {3, 6, 9, 12, 15, 18}, respectively. One of these three samples was randomly chosen for volumetric measurements. The distance T between any two consecutive slices belonging to each sample generated from the 1/3 systematic sampling scheme was 3 × 8 mm or 24 mm. Therefore, the distance d between the test points was found to be 14.4 mm by inserting a T value of 24 mm and a V equal to 750 cm3 in Eq. 3. Regarding the patients with a normal splenic size, volume assessments were made using samples of MDCT slices arising from sampling intensities of 1/2 and 1/3. Based on Eq. 3, the distance d was 9.1 mm and 7.5 mm when the volume of a normal spleen was estimated with samples containing every second and third slice, respectively (Fig. 1b, c). The selection of the sampling intensities for both groups of patients was based on the requirement to use a sample size having at least three slices for splenic volume estimation. The above sample size coincides with the minimum number of slices needed to apply Eq. 2 and find the relevant CE. The distance between the test points of the grid and the number of MDCT slices used for estimating the volume of a normal or enlarged spleen are presented in Table 1.
Repeatability of stereological estimations
The volumetric analysis was performed one more time by using the optimal stereological approaches for estimating the splenic volume of all patients belonging to both groups. The measurements were made by the same user who performed the initial set of stereological estimations. The interval between the first and the second set of volumetric measurements was more than 1 month. The repeatability was expressed with the coefficient of variability (CV) value. Different CV values were calculated for splenic volume estimations in patients with or without splenomegaly.
Statistics
The time measurements and CE estimations were expressed as mean values ± 1 standard deviation. The Kolmogorov-Smirnov test was employed to check the normality of the volumetric data obtained by planimetry and the optimal stereological approaches. For both groups of participants, the statistical difference and correlation between stereological and planimetric volume estimations was determined. The Bland-Altman statistical test [22] was applied to find the agreement between the two volumetric methods. The mean percentage difference (M) between stereological and planimetric volume estimations was calculated for each group of patients. The 95 % limits of agreement were equal to M ± 1.96 standard deviation of the volume differences. A P-value below 0.05 was considered as statistically significant for all tests. Statistical analysis was made using the Graph Pad package version 4.00 (Graph Pad Software Inc., CA, USA).
Results
Definition of the optimal stereological approach
The precision of the obtained stereological splenic volume estimations in patients with splenomegaly is presented in Fig. 2. The mean CE exceeded the target precision of 5 % when systematic sampling intensities of 1/4, 1/5, and 1/6 were adopted (Fig. 2). Volume assessments on the entire slice set depicting an enlarged spleen resulted in a mean CE of 2.8 ± 0.5 %. The corresponding CE with the use of a sample consisting of every second or third MDCT slice was 3.7 ± 0.9 % and 4.9 ± 1.0 %, respectively (Fig. 2). The mean time for volumetry using the total number of slices crossing an enlarged spleen or a sample of slices generated from a systematic sampling intensity of 1/2 was 3.3 ± 0.7 min and 2.6 ± 0.5 min, respectively. The respective duration was reduced to 2.3 ± 0.4 min when the analysis was made on a sample containing every third MDCT slice. Based on the above data, the application of stereology on a sample of slices arising from the 1/3 systematic sampling scheme was considered as the optimal approach. This approach could provide quick volume estimates with an acceptable level of precision. The CV value associated with repeated estimations of splenic volume in patients with splenomegaly using the optimal stereological approach was found to be 3.8 %.

Mean coefficient of error (±1 standard deviation) of stereological splenic volume estimations in patients with splenomegaly obtained by the entire slice set depicting the spleen and samples of MDCT slices generated from systematic sampling intensities of 1/2, 1/3, 1/4, 1/5, and 1/6
Stereological estimations of the normal splenic volume using the 1/3 systematic sampling scheme led to a high and unacceptable mean CE of more than 10 % (Fig. 3). The volumetry on the entire slice set showing the spleen or on samples of images generated from a systematic sampling intensity of 1/2 resulted in an acceptable precision below 5 % (Fig. 3). The mean time for stereological volume estimations using all slices imaging the normal spleen was 2.6 ± 0.6 min. The corresponding time using one half of the MDCT slices was reduced to 2.1 ± 0.4 min. The stereological approach that involved samples generated from a systematic sampling intensity of 1/2 was taken as the optimal one for estimating the normal splenic volume. Repeated volume estimations with the above optimal approach presented a variability of 3.3 %.

Mean coefficient of error (±1 standard deviation) of stereological normal splenic volume estimations obtained by the entire slice set depicting the spleen and samples of MDCT slices generated from systematic sampling intensities of 1/2 and 1/3
Comparison with planimetric estimations
For both groups of patients, the distribution of splenic volume estimations derived either by manual planimetry or by the optimal stereological approaches was found to be normal (P > 0.10). No significant difference was found between the two volumetric methods for estimating the volume of a normal (P = 0.11) or enlarged spleen (P = 0.06) according to a paired t-test. Planimetric and stereological volume estimations were strongly correlated (normal spleen, r = 0.99; enlarged spleen, r = 0.96), where r is the Pearson correlation coefficient. For the group of patients with a normal spleen, the Bland-Altman statistical test revealed that the optimal stereological approach resulted in slightly higher normal splenic volume assessments than those derived by planimetry with a mean difference of −1.3 ± 4.3 % (Fig. 4a). The 95 % limits of agreement were equal to −9.7 % and 7.1 % (Fig. 4a). Regarding the patients with splenomegaly, the mean difference between splenic volume estimations obtained by the two volumetric methods was −2.7 ± 5.2 % with confidence intervals of −12.9 % and 7.5 % (Fig. 4b).

Bland-Altman scatter plots presenting the percentage differences between splenic volume estimations derived by the manual planimetry and the optimal stereological approach for patients having a (a) normal and (b) enlarged spleen. The solid line and dotted lines illustrate the mean percentage difference and the 95 % limits of agreement, respectively
Discussion
The assessment of splenic volume from CT data often relies on simple and easily performed linear measurements. The uni-dimensional indexes such as splenic width [23] and length [24] have been employed for organ volume prediction. However, volumetry based on these indexes is characterized by a limited accuracy [3]. The widely used splenic index [1, 25], defined as the product of length, width, and depth of the spleen, should only be considered as a surrogate of the real organ size [26]. Splenic volume has been previously estimated with the aid of the prolate ellipsoid formula [23, 27]. This assumption about the organ shape may result in a systematic overestimation of the splenic volume [23]. The volume of the spleen has also been assessed by incorporating the uni-dimensional indexes into different mathematical formulas [23, 28, 29]. There is no consensus about generally accepted equations for splenic volume assessment in adults or children with a normal or enlarged spleen.
The method of planimetry based on the manual contouring of organ borders on all CT images and then on the summation of the organ volumes enclosed by the contours has been extensively employed for splenic volume measurement [3, 8, 24, 28–31]. Planimetric CT measurements are accurate with a mean error of less than 3.7 % from the actual splenic volume [8]. The manual planimetry is often considered the reference method to examine the validity of different approaches used for splenic volume determination [24, 28, 29, 31]. However, manual segmentation on all cross-sectional images depicting the spleen is a time-consuming process. Automated segmentation methods have also been proposed in the literature for spleen volumetry from MDCT data [26, 32, 33]. The validity of the method of Harris et al. [32] was not tested in patients with splenomegaly, whereas that introduced by Hammon et al. [33] was solely applied in 15 lymphoma patients. The probabilistic atlas developed by Linguraru et al. [26] led to segmentation errors when the enlarged spleens were extended into the small intestines due to the similar intensity values of these tissues.
In the current study, the stereological point counting method was employed for estimating splenic volume in patients with or without splenomegaly from MDCT data. The method was initially based on the automatic placement of a systematic grid of test points on each image. The user intervention was limited to the selection of the grid points falling within the spleen. The user perception and knowledge of abdominal anatomy, as presented in MDCT images, is a prerequisite for reliable stereological volume estimations. However, the success of the method is not affected either by the user dexterity to trace the outline of the spleen on each image or by the application of any other advanced segmentation technique. Furthermore, stereological estimations are independent of any type of linear measurements and of any assumption about the shape of the spleen.
The stereological method was optimized through the systematic slice sampling procedure. This process revealed that the normal splenic volume may be estimated with a mean CE of 5 % using samples of slices generated by a sampling intensity of 1/2. The above samples consisted of only four to seven systematically sampled MDCT slices. A similar precision of 5 % was found for spleen volumetry in patients with splenomegaly when the 1/3 systematic sampling scheme was employed. The size of these samples varied from five to eight MDCT images. All volume estimations were obtained by counting about 150 points on the systematically sampled MDCT slices crossing a normal or enlarged spleen. These point counts per volume were secured by selecting the appropriate separation distance between the test points of the grid for each sampling intensity with the aid of Eq. 3. This process of point spacing choice is very simple, requiring only a guess of the average organ volume without the need for extensive volume measurements using different grid sizes in a pilot study [13, 34, 35].
For both groups of patients with or without splenomegaly, the splenic volume estimations derived by the optimal stereological approaches were highly correlated with the respective values obtained by the reference method of manual planimetry. The 95 % limits of agreement between the two methods, as calculated by the Bland-Altman analysis, were quite narrow and they were considered clinically acceptable. The variability of the repeated splenic volume estimations obtained by stereology was found to be relatively low. Moreover, the use of the optimal stereological approach provided a normal splenic volume assessment in a mean time of 2.1 min. The corresponding mean duration for volumetry in patients with enlarged spleens was only 2.3 min.
Our study faces some limitations. The presented splenic volume assessments were limited to a relatively small number of adults with or without splenomegaly. The applicability and reliability of the optimized stereological approaches should also be examined in paediatric patients undergoing an abdominal CT examination. The accuracy of the proposed volumetric approaches may also be checked in comparison with the volume of resected specimens. Moreover, the stereological analysis for each patient was performed by a single investigator. Further research is required to evaluate the interobserver variability associated with stereological splenic volume estimations on MDCT images.
In conclusion, the current study proposes two different stereological approaches for estimating the volume of a normal or enlarged spleen from MDCT data. No significant difference was observed between the splenic volume estimations derived by these approaches and the reference method of manual planimetry. The excellent correlation and good agreement between the two methods clearly implies that the proposed stereological approaches may be considered effective alternative methods to the labour-intensive manual planimetry. The application of these approaches on a sample of systematically selected MDCT slices depicting the spleen enables the quick and reproducible organ volume estimation with a precision of about 5 %.
Abbreviations
- CT:
-
computed tomography
- US:
-
ultrasound
- MDCT:
-
multidetector computed tomography
- CE:
-
coefficient of error
- CV:
-
coefficient of variability
References
Pozo AL, Godfrey EM, Bowles KM (2009) Splenomegaly: investigation, diagnosis and management. Blood Rev 23:105–111
Arkles LB, Gill GD, Molan MP (1986) A palpable spleen is not necessarily enlarged or pathological. Med J Aust 145:15–17
Robertson E, Leander P, Ekberg O (2001) Radiology of the spleen. Eur Radiol 11:80–95
Ishibashi H, Higuchi N, Shimamura R, Hirata Y, Kudo J, Niho Y (1991) Sonographic assessment and grading of spleen size. J Clin Ultrasound 19:21–25
Rodrigues AJ, Rodrigues CJ, Germano MA, Rasera JI, Cerri GG (1995) Sonographic assessment of normal spleen volume. Clin Anat 8:252–255
De Odorico I, Spaulding KA, Pretorius DH, Lev-Toaf AS, Bailey TB, Nelson TR (1999) Normal splenic volumes estimated using three-dimensional ultrasonography. J Ultrasound Med 18:231–236
Hidaka H, Nakazawa T, Wang G et al (2010) Reliability and validity of splenic volume measurement by 3-D ultrasound. Hepatol Res 40:979–988
Breiman RS, Beck JW, Korobkin M et al (1982) Volume determinations using computed tomography. Am J Roentgenol 138:329–333
Roberts N, Puddephat MJ, McNulty V (2000) The benefit of stereology for quantitative radiology. Br J Radiol 73:679–697
Pache JC, Roberts N, Vock P, Zimmermann A, Cruz-Orive LM (1993) Vertical LM sectioning and parallel CT scanning designs for stereology: application to human lung. J Microsc 170:9–24
Mazonakis M, Damilakis J, Varveris H (1998) Bladder and rectum volume estimations using CT and stereology. Comp Med Imaging Graph 22:195–201
Emizreoglu M, Sahin B, Selcuk MB, Kaplan S (2005) The effects of section thickness on the estimation of liver volume by the Cavalieri principle using computed tomography images. Eur J Radiol 56:391–397
Mazonakis M, Pagonidis K, Schlosser T et al (2008) Stereological estimation of left-ventricular volumetric and functional parameters from multidetector-row computed tomography data. Eur Radiol 18:1338–1349
Eriksen N, Rostrup E, Andersen K et al (2010) Application of stereological estimates in patients with severe head injuries using CT and MR scanning images. Br J Radiol 83:307–317
Uzkeser M, Sahin H, Ozogul B, Cayir Y, Alper F, Emet M (2013) Defining the percentage of intra-abdominal hemorrhage in abdominal computerized tomography using stereology in patients with blunt liver injury and determining its relationship with outcomes. J Trauma Acute Care Surg 74:224–229
Betal D, Hughes ML, Whitehouse GH, Roberts N (2000) Postprandial decrease in splenic volume demonstrated by magnetic resonance imaging and stereology. Clin Anat 13:404–409
Mazonakis M, Damilakis J, Maris T, Prassopoulos P, Gourstosyiannis N (2000) Estimation of spleen volume using MR imaging and a random marking technique. Eur Radiol 10:1899–1903
Cruz-Orive LM (1993) Systematic sampling in stereology. Bull Int Stat Inst 55:451–468
Mazonakis M, Pagonidis K, Damilakis J (2011) Right ventricular volumes and ejection fraction by MR imaging and stereology: comparison with standard image analysis method. Clin Anat 24:868–873
Robb RA (2000) Biomedical imaging, visualization, and analysis. Wiley-Liss, New York
Gundersen HJG, Jensen EB (1987) The efficiency of systematic sampling in stereology and its prediction. J Microsc 147:229–263
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Rezai P, Tochetto SM, Galizia MS, Yaghmai V (2011) Splenic volume model constructed from standardized one-dimensional MDCT measurements. Am J Roentgenol 196:367–372
Bezerra AS, D’Ippolito G, Faintuch S, Szejnfeld J, Ahmed M (2005) Determination of splenomegaly by CT: is there a place for a single measurement? Am J Roentgenol 184:1510–1513
Cools L, Osteaux M, Divano L, Jeanmart L (1983) Prediction of splenic volume by a simple CT measurement: a statistical study. J Comput Assist Tomogr 7:426–430
Linguraru MG, Sandberg JK, Jones EC, Summers RM (2013) Assessing splenomegaly: automated volumetric analysis of the spleen. Acad Radiol 20:675–684
Asghar A, Agrawal D, Yunus SM, Sharma PK, Zaidi SHH, Sinha A (2011) Standard splenic volume estimation in north Indian adult population using 3D reconstruction of abdominal CT scan images. Anat Res Int 2011:707325
Prassopulos P, Daskalogiannaki M, Raissaki M, Hatjidakis A, Gourtsoyiannis N (1997) Determination of normal splenic volume on computed tomography in relation to age, gender and body habitus. Eur Radiol 7:246–248
Schlesinger AE, Hildebolt CF, Siegel MJ, Pilgrim TK (1994) Splenic volume in children: simplified estimation at CT. Radiology 193:578–580
Lamb PM, Lund A, Kanagasabay RR, Martin A, Webb JAW, Reznek RH (2002) Spleen size: how well do linear ultrasound measurements correlate with three-dimensional CT volume assessments? Br J Radiol 75:573–577
Yetter EM, Acosta KB, Olson MC, Blundell K (2003) Estimating splenic volume: sonographic measurements correlate with helical CT determination. Am J Roentgenol 181:1615–1620
Harris A, Kamishima T, Hao HY et al (2010) Splenic volume measurements on computed tomography utilizing automatically contouring software and its relationship with age, gender and anthropometric parameters. Eur J Radiol 75:97–101
Hammon M, Dankerl P, Kramer M et al (2012) Automated detection and volumetric segmentation of the spleen in CT scans. Röfo 184:734–739
Cotter D, Miszkiel K, Al-Sarraj S et al (1999) The assessment of postmortem brain volume; a comparison of stereological and planimetric methodologies. Neuroradiology 41:493–496
Mazonakis M, Damilakis J, Mantatzis M et al (2004) Stereology versus planimetry to estimate the volume of malignant liver lesions on MR imaging. Magn Reson Imaging 22:1011–1016
Acknowledgments
The scientific guarantor of this publication is John Damilakis. The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. One of the authors has significant statistical expertise. Institutional review board approval was not required. Written informed consent was obtained from all subjects (patients) in this study. No study subjects or cohorts have been previously reported. Methodology: retrospective, experimental, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mazonakis, M., Stratakis, J. & Damilakis, J. Efficient stereological approaches for the volumetry of a normal or enlarged spleen from MDCT images. Eur Radiol 25, 1761–1767 (2015). https://doi.org/10.1007/s00330-014-3561-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-014-3561-7