
Abstract
This study aimed to compare the effectiveness of a 6-week combined exercise program with and without connective tissue massage (CTM) on pain, fatigue, sleep problem, health status, and quality of life in patients with fibromyalgia syndrome (FMS). Patients were randomly allocated into Exercise (n = 20) and Exercise + CTM (n = 20) groups. The exercise program with and without CTM was carried out 2 days a week for 6 weeks. Pain, fatigue, sleep problem with Visual Analog Scales, health status with Fibromyalgia Impact Questionnaire (FIQ), and quality of life with Short Form-36 were evaluated. After the program, pain, fatigue and sleep problem reduced, health status (except of the scores of FIQ-1 and FIQ-10), physical functioning, role limitations due to physical health, bodily pain, role limitations due to emotional health, vitality, and general health perceptions parameters related to quality of life improved in the Exercise group, (P < 0.05). In the Exercise + CTM group, pain, fatigue and sleep problem decreased, health status and quality of life improved (P < 0.05). Pain, fatigue, sleep problem, and role limitations due to physical health improved in the Exercise + CTM group in comparison to the Exercise group (P < 0.05). The study suggested that exercises with and without CTM might be effective for decreasing pain, fatigue and sleep problem whereas increasing health status and quality of life in patients with FMS. However, exercises with CTM might be superior in improving pain, fatigue, sleep problem, and role limitations due to physical health compared to exercise alone.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fibromyalgia syndrome (FMS) is associated with chronic widespread pain and at least eleven positive tender points out of 18 according to the 1990 criteria of the American College of Rheumatology (ACR) [1]. It is often associated with such symptoms as reduced physical strength, fatigue, sleep disorders, gastrointestinal disorders, and psychiatric disorders such as depression [2]. Pain and other symptoms are associated with fibromyalgia interferes with daily function, work, and social activities, resulting a decrease in quality of life [3]. FMS is a common disorder which occurs more often in women than in men, with an estimated prevalence of 0.5–5.8% in the general population [4, 5].
Although it is a syndrome of unknown etiology, several studies on autonomic nervous system, neurotransmitters, hypothalamic–pituitary–adrenal axis hormones, central sensitization, and peripheral tissues in FMS revealed various abnormalities [6, 7]. Especially, parasympathetic activity and vascularization decrease, muscle tension, stress, pain and complain of sleep disorder increase in these patients. Because there is not any known cause, or cure, and therefore treatment focuses on the control or relief of symptoms [8]. Although medication mainly focuses on pain reduction, physical therapy approaches aim to improve pain, fatigue, muscle weakness, deconditioning, sleep disturbances, and overall health [9].
Several physical therapy applications are available for patients with FMS. These applications include educational programs, cognitive behavioral therapy, balneotherapy, acupuncture, electrophysical agents, manual therapy, and exercises [9,10,11,12,13,14,15]. Especially, exercise has favorable effects on physical fitness, aerobic performance, pain management, and quality of life of patients with FMS [15]. Most clinical trials have focused on aerobic exercises [16]. Few studies have shown strengthening and stretching exercises as safe and effective for FMS [17, 18]. Recent studies also focused on the effects of combined exercise interventions for the management of patients with FMS [19, 20]; nevertheless, there are inadequate studies related to these exercise interventions.
Connective tissue massage (CTM), one of the varied manual therapy techniques for FMS, also generates local mechanical effects on mast cells in the connective tissue by short and long tractions and thus creates vasodilation by reducing the sympathetic activity. Subsequently, parasympathetic effect increases; and the improvement in the circulation promotes healing process [21, 22]. In literature, it was applied only CTM in treatment of FMS in a study of Brattberg [23]. In a study of Citak-Karakaya et al. [13], researchers investigated the effects of CTM with combined ultrasound therapy in patients with FMS. In a study of Ekici et al. [14], authors compared the effectiveness of manual lymph drainage therapy and CTM in patients with FMS; whereas, in another study of Ekici et al. [24] they compared the effects of Pilates exercises and CTM in FMS. However, there are few randomized controlled trials (RCT) that examine its effectiveness on FMS [13, 14, 23, 24].
Therefore, this prospective RCT aimed to compare the effectiveness of a 6-week combined exercise program with and without CTM on pain, fatigue, sleep problem, health status, and quality of life in patients with FMS. The following hypotheses were investigated: (1) combined exercises either with or without CTM would be effective for the treatment of FMS. (2) The combined exercise program in addition to CTM may change the outcomes.
Methods
Study design
In this prospective RCT, written informed consent forms were obtained from all participants; and they were informed about the study based on the Declaration of Helsinki. It was approved by the Ethics Committee of Ankara Yildirim Beyazit University, Faculty of Medicine, Clinical Researches Ankara, Turkey (Approval number: 105/2015). The study began in May 2015 and ended in January 2017.
Patients
The patients diagnosed with FMS by a rheumatologist according to the 1990 criteria of ACR for the syndrome [1] and referred to the Physiotherapy and Rehabilitation clinic were screened for eligibility. The study’s inclusion criteria were as follows: being women, having FMS, 18–65 years of age, and being volunteer. The exclusion criteria were as follows: have neurologic, infectious, endocrine, and other inflammatory rheumatic diseases, severe psychological disorders, any condition interfering with exercise (advanced cardiac respiratory or orthopedic problems), malignancy, being pregnant, and intervention including exercise program or physical therapy in the last 6 months.
Assessments
Physical characteristics (age, weight, height, body mass index (BMI), smoking, and any mechanism of injury), were collected. The participants’ physical activity was measured using the Turkish version of the International Physical Activity Questionnaire-7 (IPAQ-7) for baseline standardization [25]. Before and after the program, evaluations related to pain intensity, complaints of fatigue and nonrestorative sleep, health status, and quality of life were carried out. All patients were evaluated by the same physical therapist (BAK), who was blinded to the baseline results.
Pain, fatigue and sleep problem were assessed with the Visual Analog Scales (VASs). The reliability of this scale was determined by Clark et al. [26]. This scale involves a horizontal line, 10 cm long, such that “0” defines “no pain” and “10” defines “unbearable pain” for pain evaluation, “0” indicates “no fatigue” and the “10” indicates “intolerable fatigue” for fatigue evaluation, and “0” shows “refreshing sleep” and the “10” shows “non-refreshing sleep” for sleep evaluation. The patient is asked to mark the intensity of her pain, fatigue and sleep problem on the horizontal line.
Health status of the patients was evaluated using the Turkish version of the Fibromyalgia Impact Questionnaire (FIQ) [27]. The questionnaire has 10 subscales, ranging from 0 to 10, assessing ‘‘physical impairment’’, ‘‘days felt good’’, ‘‘work missed’’, ‘‘work impairment’’, ‘‘pain’’, ‘‘fatigue’’, ‘‘morning tiredness’’, ‘‘stiffness’’, ‘‘anxiety’’, and ‘‘depression’’. Total score of the FIQ ranges from 0 to 100, and higher scores indicate a greater impact of the disease on the patient [28].
The quality of life was assessed with the Turkish of the Short Form-36 (SF-36) [29]. The SF-36 consists of 36 questions: physical functioning (10 items), role limitations due to physical health (4 items), bodily pain (2 items), social functioning (2 items), vitality (4 items), role limitations due to emotional health (3 items), mental health (5 items), general health perceptions (5 items) and changes in health over time (1 item, not included in the final score). The SF-36 score ranges from 0 (the worst score) to 100 (the best score). Thus, higher scores indicate better health [29].
Randomization
After the comprehensive clinical assessments, patients were randomly assigned to Exercise group or Exercise + CTM group using a computer-generated randomized table of numbers, created by an individual not involved in the recruitment and treatment of patients. Individual, sequentially numbered index cards with a random assignment were prepared. The index cards were folded and placed in sealed, opaque envelopes to concealed allocation. The treating therapists opened the envelope and proceeded with treatment according to the group assignment. Patients in Exercise group were performed the exercise program, whereas patients in Exercise + CTM group were performed the exercise program with CTM applications.
Interventions
During this program, general using drugs, which were recommended in our clinics, were not changed for standardization. In addition, it was not increased number of using drugs during the assessment and treatment sessions.
Combined exercise program
After the randomization, sessions began with postural education by placing patients in standing position to find a neutral balanced position of the spine curvatures [30]. The patients were asked to maintain neutral spine during the program.
The combined exercise program was carried out 2 days a week for 6 weeks by physical therapists (MEY, CSP). Each exercise program took 1 h. It was composed of 10-min warm-up exercises, 40-min aerobic and strengthening exercises, 10-min cool-down, stretching exercises including neck, trunk, upper and lower limb muscles. The program was selected from previous studies [19, 20].
The aerobic exercise consisted of 20-min walking on a treadmill. The target heart rate was initially adjusted to 65–70% of the maximal heart rate and to 75–80% of the maximal heart rate in the advanced program. Muscle strengthening exercises were then performed with elastic resistive bands for 20 min, where deep neck muscles, deltoid, latissimus dorsi, serratus anterior, scapular retractor muscles, pectoralis major, shoulder external rotator muscles, erector spinae, abdominalis, gluteus, and quadriceps muscles were strengthened. The patients began exercising with yellow or red Thera-Bands (Hygenic Corporation, Akron, OH, USA) with mild or medium tension. When they performed 15 repetitions without serious pain or fatigue, they progressed to the next color resistance band in the sequence of green and blue. They had 10 repetitions with a holding period of 10 s each.
CTM application
CTM was applied 2 days per week for a total of 12 sessions for 6 weeks by the same experienced physical therapist (STC). While patients were in a sitting position, starting from the lumbosacral region, the lower thoracic, scapular, interscapular, and cervical regions were included in the treatment, respectively. For creating traction between cutaneous tissues, the middle fingers of both hands were used during the application [31]. Each session lasted around 5–20 min.
Statistical analyses
For the pilot study, ten participants from each group were randomly recruited. G*Power package software program (G*Power, Version 3.0.10, Franz Faul, Universität Kiel, German) was used to determine the required sample size for the study. According to the pain measurement of the study, it was calculated that a sample consisting of 40 subjects (20 per group) was needed to obtain 80% power with d = 0.80 effect size, α = 0.05 type I error, and β = 0.20 type II error [32].
Data analysis was conducted using IBM SPSS Statistics 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.). The variables were investigated using visual (histograms, probability plots) and analytical methods (Shapiro-Wilks test) to determine whether or not they were normally distributed. Descriptive analyses were presented using mean and standard deviation (SD) for the normally distributed variables, and tables of frequencies, median, minimum and maximum values for the non-normally distributed and categorical variables. Normally distributed numeric variables related to age, BMI, non-normally distributed numeric variables related to IPAQ-7 score and categorical variables related to smoking were assessed with independent sample t test, Mann–Whitney U test and Chi square test, respectively. Wilcoxon test was used to compare the measurements of the pain, fatigue, sleep problem, health status, and quality of life scores between before and after the program. Pain, fatigue, sleep problem, health status, and quality of life scores between groups were analyzed by the Mann–Whitney U test. An overall P value of less than 0.05 was considered to be statistically significant.
Results
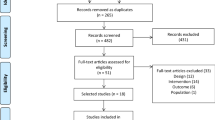
Fifty-six patients with FMS were assessed; however, forty patients completed the study. Details of included and excluded patients into the study are provided as a flowchart (Fig. 1). There were no adverse events reported with the program. There were no differences between the groups in terms of baseline physical characteristics (P > 0.05) (Table 1).

The flowchart diagram for the participants
Before the program, there were no differences between groups in terms of pain, fatigue and sleep problem, health status, and quality of life scores (Tables 2, 3). After the program, pain, fatigue and sleep problem decreased, health status (except of the scores of FIQ-1 and FIQ-10), the scores of physical functioning, role limitations due to physical health, bodily pain, role limitations due to emotional health, vitality, and general health perceptions scales related to quality of life improved in the Exercise group (P < 0.05), (Tables 2, 3). There was no difference for the scores of social functioning and mental health scales related to quality of life (Table 3). In the Exercise + CTM group, pain, fatigue and sleep problem decreased, health status (all items of the FIQ) and quality of life (subscale of the SF-36) improved (P < 0.05), (Tables 2, 3).
The intergroup comparison showed significant differences in some parameters in favor of the Exercise + CTM group (Table 3). Pain, fatigue and sleep problem, and role limitations due to physical health related to quality of life improved in the Exercise + CTM group in comparison to the Exercise group (P < 0.05), (Table 4). No significant differences were found for the other parameters between the groups (Table 4).
Discussion
The following findings were observed in the present study: Pain, fatigue and sleep problem decreased, health status except of physical impairment and depression, and quality of life (physical functioning, role limitations due to physical health, bodily pain, role limitations due to emotional health, vitality, and general health perceptions parameters) improved in only combined exercise program; the combined exercises with CTM reduced pain, fatigue and sleep problem, increased health status and quality of life in patients with FMS; Exercises with CTM were more effective in improving pain, fatigue and sleep problem, and role limitations due to physical health related to quality of life compared to exercise alone.
Exercise training is commonly recommended as a treatment for management of FMS symptoms [15,16,17,18,19]. Latorre et al. [33] demonstrated that physical training program in water and on land was effective in patients with FMS and thus yielded a decrease in pain and disease impact, and an increase in functional capacity. Rooks et al. [34] presented that progressive strength training and aerobic exercise may be safe, well tolerated, and effective at improving muscle strength, cardiovascular endurance and functional status in women with FMS without exacerbating symptoms. Ekici et al. [24] stated that Pilates exercises had a role in reducing pain, anxiety, and quality of life in FMS. Recently, combined exercises were also reported to be beneficial for FMS [19, 20]. Sañudo et al. [19] showed the effectiveness of supervised aerobic exercise and combined exercise program including supervised aerobic, muscle strengthening, and flexibility exercises for decreasing depression and increasing health status, quality of life and muscle strength in patients with FMS. However, combined exercising alone were proved to be a more effective form of program compared to aerobic exercise. Furthermore, exercise interventions alone have effect sizes similar to those of drugs; however, a significant barrier to their use is poor adherence [35]. For this reason, in our study it was performed supervised combined exercise for patients with FMS. Our study put forward that combined exercises might be effective for improving pain, fatigue, sleep problems, some parameters of health status and quality of life in these patients. These results should be taken into account for further studies to improve various symptoms of the patients with FMS.
In literature, different studies investigated the effects of CTM on management of FMS. Brattberg [23] emphasized that CTM resulted in pain relief, decreased depression, and increased quality of life in patients with FMS. Citak-Karakaya et al. [13] indicated that CTM combined with ultrasound therapy was helpful in reducing pain, tiredness, and sleeping problems and increasing quality of life in patients with FMS. Ekici et al. [14] presented that only CTM applications improved pain, health status, and quality of life in patients with FMS. Our results obtained from exercises with CTM group were in line with these studies. Moreover, it was found in the current study that exercises with CTM might be more effective in improving pain, fatigue and sleep problem, and role limitations due to physical health related to quality of life compared to only exercises. The results may be related to producing general body relaxation, decreasing muscle spasm and increasing plasma β-endorphins and vascularization throughout the CTM applications [31]. Furthermore, some studies indicate that touch and massage have beneficial influences across multiple-stress systems; in particular, decreasing sympathetic nervous system activity, hypothalamic-pituitary adrenocortical activity and stress hormones [35, 36]. Consequently, combined treatment including exercises with CTM might be superior in treating FMS patients with severe pain, fatigue and sleep problem, and limitations due to physical health.
The current study had some limitations. First of all, we evaluated the clinical results using self-reported measures, not objective measurements, which may have some influences on the final result. However, the effects of combined exercise with CTM on functional capacity parameters including muscle strength, power, flexibility, agility, balance, and aerobic endurance in patients with FMS should be investigated for further studies. Secondly, the results of a 6-week program were presented in this study. Long-term effects should be observed with follow-up studies. Thirdly, during this program, patients with FMS used their general drugs, because medication has been recommended generally in our clinics. However, the type and number of using drugs were not changed for the standardization. In further studies, the patients might be asked not to use their drugs during the study.
Conclusion
In this study, it was observed that combined exercises with and without CTM might be effective for reducing pain, fatigue and sleep problem while increasing the health status and quality of life in patients with FMS. In addition, exercises with CTM might be superior in improving pain, fatigue and sleep problem, and role limitations due to physical health related to quality of life compared to exercise alone. The CTM applications which have no any side effects and are economic may be applied safely by physical therapists and other experienced healthcare professionals in the CTM for patients with FMS in the clinics.
References
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL (1990) The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 33:160–172
Häuser W, Zimmer C, Felde E, Kollner V (2008) What are the key symptoms of fibromyalgia? Results of a survey of the German Fibromyalgia Association. Schmerz (Berlin, Germany) 22:176–183
Arnold LM, Crofford LJ, Mease PJ et al (2008) Patient perspectives on the impact of fibromyalgia. Patient Educ Couns 73:114–120
Branco JC, Bannwarth B, Failde I et al (2010) Prevalence of fibromyalgia: a survey in five European countries. Arthritis Rheum 39:448–453
Lawrence RC, Felson DT, Helmick CG et al (2008) Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum 58:26–35
Martinez-Lavin M, Hermosillo AG (2000) Autonomic nervous system dysfunction may explain the multisystem features of fibromyalgia. Arthritis Rheum 29:197–199
Le Goff P (2006) Is fibromyalgia a muscle disorder? Joint Bone Spine 73(3):239–242
Schaefer KM (2004) Caring for the patients with fibromyalgia: the rehabilitation nurse’s role. Rehabil Nurs 29:49–55
Offenbacher M, Stuck G (2000) Physical therapy in the treatment of fibromyalgia. Scand J Rheumatol 113(Suppl):78–85
Redondo JR, Justo CM, Moraleda FV et al (2004) Long-term efficacy of therapy in patients with fibromyalgia: a physical exercise-based program and a cognitive-behavioral approach. Arthritis Rheum 51:184–192
Karagulle MZ, Karagulle M (2004) Balneotherapy and spa therapy of rheumatic diseases in Turkey: a systematic review. Forsch Komplementarmed Klass Naturheilkd 11:33–41
Field T, Delage J, Hernandez-Reif M (2003) Movement and massage therapy reduce fibromyalgia pain. J Bodyw Mov Ther 7:49–52
Citak-Karakaya I, Akbayrak T, Demirturk F, Ekici G, Bakar Y (2006) Short and long-term results of connective tissue manipulation and combined ultrasound therapy in patients with fibromyalgia. J Manip Physiol Ther 29:524–528
Ekici G, Bakar Y, Akbayrak T, Yuksel I (2009) Comparison of manual lymph drainage therapy and connective tissue massage in women with fibromyalgia: a randomised controlled trial. J Manip Physiol Ther 32:127–133
Wilson B, Spencer H, Kortebein P (2012) Exercise recommendations in patients with newly diagnosed fibrmyalgia. PMR 4:252–255
Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL (2007) Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 4:CD003786
Lorena SB, Lima Mdo C, Ranzolin A, Duarte ÂL (2015) Effects of muscle stretching exercises in the treatment of fibromyalgia: a systematic review. Rev Bras Reumatol 55(2):167–173
Busch AJ, Webber SC, Richards RS (2013) Resistance exercise training for fibromyalgia. Cochrane Database Syst Rev 12:CD010884
Sañudo B, Galiano D, Carrasco L, Blagojevic M, de Hoyo M, Saxton J (2010) Aerobic exercise versus combined exercise therapy in women with fibromyalgia syndrome: a randomized controlled trial. Arch Phys Med Rehabil 91(12):1838–1843
Sarıfakıoğlu B, Güzelant AY, Güzel EC, Güzel S, Kızıler AR (2014) Effects of 12-week combined exercise therapy on oxidative stress in female fibromyalgia patients. Rheumatol Int 34(10):1361–1367
Holey LA, Dixon J, Selfe J (2011) An exploratory termographic investigation of the effects of connective tissue massage on autonomic function. J Manip Physiol Ther 34:457–462
Holey EA (2000) Connective tissue massage: a bridge between complementary and orthodox approaches. J Bodyw Mov Ther 4:72–80
Brattberg G (1999) Connective tissue massage in the treatment of fibromyalgia. Eur J Pain 3:235–245
Ekici G, Unal E, Akbayrak T, Vardar-Yagli N, Yakut Y, Karabulut E (2017) Effects of active/passive interventions on pain, anxiety, and quality of life in women with fibromyalgia: randomized controlled pilot trial. Women Health 57(1):88–107
Saglam M, Arikan H, Savci S et al (2010) International physical activity questionnaire: reliability and validity of the Turkish version. Percept Mot Skills 111(1):278–284
Clark P, Lavielle P, Martínez H (2003) Learning from pain scales: patient perspective. J Rheumatol 30:1584–1588
Sarmer S, Ergin S, Yavuzer G (2000) The validity and reliability of the Turkish version of the Fibromyalgia Impact Questionnaire. Rheumatol Int 20:9–12
Burckhardt C, Clark S, Bennet R (1991) The fibromyalgia impact questionnaire. Development and validation. J Rheumatol 18:728–733
Kocyigit H, Aydemir O, Fisek G, Olmez N, Memis A (1999) Reliability and validity of the Turkish version of short-form-36 (SF-36). Turk J Drugs Ther 12:102–106
O’Sullivan PB (2004) Clinical instability of the lumbar spine: its pathological basis, diagnosis and conservative management. Churchill Livingstone, Singapore
Holey LA, Dixon J (2014) Connective tissue manipulation: a review of theory and clinical evidence. J Bodyw Mov Ther 18(1):112–118
Faul F, Erdfelder E, Lang AG, Buchner A (2007) G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39(2):175–191
Latorre PÁ, Santos MA, Heredia-Jiménez JM (2013) Effect of a 24-week physical training programme (in water and on land) on pain, functional capacity, body composition and quality of life in women with fibromyalgia. Clin Exp Rheumatol 31(6 Suppl 79):S72–S80
Rooks DS, Silverman CB, Kantrowitz FG (2002) The effects of progressive strength training and aerobic exercise on muscle strength and cardiovascular fitness in women with fibromyalgia: a pilot study. Arthritis Rheum 47(1):22–28
Lindgren L, Rundgren S, Winsö O et al (2010) Physiological responses to touch massage in healthy volunteers. Auton Neurosci 158(1):105–110
Holt-Lunstad J, Birmingham WA, Light KC (2008) Influence of a “warm touch” support enhancement intervention among married couples on ambulatory blood pressure, oxytocin, alpha amylase, and cortisol. Psychosom Med 70(9):976–985
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study did not receive any specific Grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
Authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Toprak Celenay, S., Anaforoglu Kulunkoglu, B., Yasa, M.E. et al. A comparison of the effects of exercises plus connective tissue massage to exercises alone in women with fibromyalgia syndrome: a randomized controlled trial. Rheumatol Int 37, 1799–1806 (2017). https://doi.org/10.1007/s00296-017-3805-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3805-3