
Abstract
This study aims to estimate the reliable prevalence of fibromyalgia using meta-analysis method. Available databanks were searched using appropriate keywords. According to the heterogeneity between the results (indicated by Cochrane and I square indices), random- or fixed-effects model was applied to combine the point prevalences. Meta-regression models were used to assess the suspected factors in the heterogeneity. In 65 selected papers, 81 evidences regarding prevalence of fibromyalgia among 3,609,810 subjects from general population and specific groups were investigated. The total prevalences (95% confidence intervals) of fibromyalgia among general population, women, men, patients referring to rheumatology and internal departments, patients with Irritable bowel syndrome (IBS), hemodialysis patients and those with type 2 diabetes mellitus were estimated as of 1.78% (1.65, 1.92), 3.98% (2.80, 5.20), 0.01% (−0.04, 0.06), 15.2% (13.6, 16.90), 12.9% (12.70, 13.10), 6.30% (4.60, 7.90) and 14.80% (11.10, 18.40), respectively. In addition, prevalence of fibromyalgia in specified groups varied from 3.90% in hemodialysis patients to 80% in patients suffering from Behcet syndrome. This meta-analysis showed that prevalence of fibromyalgia in general population was significantly lower than that in populations with some diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fibromyalgia (FM) syndrome is one of the most common musculoskeletal disorders with unknown cause involving adults especially women aged 20–55 [1]. The primary diagnosis is based on chronic generalized pain with tenderness during exam, fatigue, sleep disorder, headache and mood/cognitive problems [1, 2]. The American College of Rheumatology (ACR) has defined the fibromyalgia as generalized pains for at least three months with 11/18 tender points during physical examination [3, 4]. Although combining these two criteria can detect 81–88% of cases, other complaints such as fatigue, sleep disorder, morning stiffness, paresthesia and psychosis are also common during the disease [3].
According to ACR criteria, different studies reported the prevalence of fibromyalgia between 0.2 to 5% [5]. Other studies indicate the prevalence among men and women as of 0.2–3.9% and 0.7–13%, respectively [6]. The heterogeneity in different countries can be due to different factors such as different methodologies and even real differences between countries [7]. This syndrome has been observed in most countries with various climates among different ethnic groups [8]. Prevalence of FM among women is 8–9 folds greater than that among men and is increased with age so that 7.4% of women aged 70–79 years are suffered from this problem [1]. According to the available evidences, the pain and disability is as high as that in rheumatoid arthritis which affects the personal activity and recreations leading to occupational problems [1, 9].
According to the results of primary searches, different studies have been carried out with regard to the prevalence of FM. Combining the results of these primary studies provides reliable evidences for policymaking [10,11,12]. This study aims to estimate the total prevalence of fibromyalgia in the world using meta-analysis method.
Methods
Search strategy
During 1–25 December 2016, two independent researchers searched PubMed, Web of Sciences, Ovid, Ebsco, Scopus and Cochrane library databanks and Google scholar search engine using the following Keywords to find relevant evidences written in English from each time to 30 November 2015. A sample of search strategy in PubMed is follow: ((((((((((((((((((((fibromyalgia) OR fibromyalgia-fibromyositis syndrome) OR fibromyalgia-fibromyositis syndromes) OR syndrome, fibromyalgia-fibromyositis) OR syndromes, fibromyalgia-fibromyositis) OR fibromyositis-fibromyalgia syndrome) OR fibromyositis fibromyalgia syndrome) OR fibromyositis-fibromyalgia syndromes) OR syndrome, fibromyositis-fibromyalgia) OR syndromes, fibromyositis-fibromyalgia) OR fibromyalgia, secondary) OR fibromyalgia, secondary) OR secondary fibromyalgia) OR secondary fibromyalgia) OR fibromyalgia, primary) OR fibromyalgia, primary) OR primary fibromyalgia) OR primary fibromyalgia) AND prevalence) OR epidemiology) OR frequency.
Any disagreement was managed by a third researcher. They also investigated the references of the identified papers to increase the search sensitivity.
Inclusion/exclusion criteria
All English-written articles with enough quality scores reporting the prevalence of fibromyalgia as well as sample size of the study were included in the meta-analysis. On the other hand, studies did not report the above-mentioned information, those with low-quality score, articles had not been written in English and abstracts represented in congresses without full text, were excluded from the meta-analysis.
Selection of the studies
During the investigation of the primary identified studies by two independent researchers, first, duplicates were identified and excluded. Then, irrelevant articles were removed after investigating the titles, abstracts and full texts, respectively. In addition, the investigators reviewed the results of these studies to find and omit any repeated results. A third researcher was selected to manage probable disagreements between the above-mentioned study selection processes.
Quality assessment
The above selected studies were quality assessed according to the STROBE checklist including 22 methodological questions [13]. Minimum and maximum scores achieved by each study were zero and 44, respectively. These studies were classified into low quality (less than 15.5), moderate quality (15.5–29.5) and high quality (30–44). Low-quality studies were excluded from the meta-analysis.
Data extraction
Title, first author name, date and country in which the study was conducted, prevalence of fibromyalgia, sample size of the study according to gender, mean age and age range of the participants and diagnostic methods were extracted from each study. These information were entered into the excel spreadsheets.
Statistical analysis
Data analysis was performed using Stata software. Standard error of prevalence for each study was calculated according to binomial distribution formula. The heterogeneity between the results of primary studies was presented based on I-square and Cochrane (Q) indices. P value less than 0.1 was considered significant heterogeneity. According to suggestion of Higgins and et al. [14], the I-squared results were classified into low heterogeneity (less than 25%), moderate heterogeneity (25–75%) and high heterogeneity (more than 75%). According to the results of heterogeneity between the primary studies, random- or fixed-effect model was applied for combining the results. The effect of the suspected factors for heterogeneity was assessed using meta-regression models and subgroup analysis. Pooled and primary prevalences as well as 95% confidence intervals were illustrated by forest plots. Considering the prevalence as the main indicator in the current meta-analysis, no investigation was done for publication bias.
Results
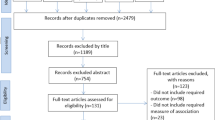
Out of 61,346 studies identified during the primary search, 1742 papers were remained after restricting the search strategy. Of them, 1040 duplicate papers were excluded. Review of titles and abstracts, 571 papers were identified irrelevant. Full text review revealed 49 irrelevant articles. Moreover, five new papers identified during the reference review. Finally, considering inclusion/exclusion criteria and quality assessment, 22 articles were omitted and 65 papers [1,2,3, 5, 7, 15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74] were identified eligible for meta-analysis (Fig. 1).

Literature search and review flowchart for selection of primary studies
Among 3,609,810 people investigated in the 65 included studies in the systematic review, 81 cases of evidence were identified the prevalence of fibromyalgia among general population and specific groups. According to the results of 44 cases of evidence (Table 1), prevalence of fibromyalgia among 3,500,756 people of general population was estimated as of 1.78% (95% confidence interval: 1.65–1.92). Subgroup analysis of Prevalence of fibromyalgia in the general population presented by World Health Organization (WHO) regions. In EURO region was reported in 24 studies varied from 0.29% in the study carried out by Sauer [64] in 2010 in Germany to 11.10% in the study conducted by Okumus [47] in Turkey (2012). The total prevalence of fibromyalgia in the EURO region was estimated as of 2.64% (95% confidence interval: 2.10–3.18) (Fig. 2).

Primary and pooled prevalences of fibromyalgia in general population and WHO regions
Prevalence of fibromyalgia in the general population of AMRO region was reported in 16 studies from 0.16% in Andary [17] study conducted in the USA (2004) to 6.36% in the study conducted by Vincent [69] in the USA (2013). The total prevalence of fibromyalgia in the AMRO general population was estimated as of 2.41% (95% confidence interval: 1.69–3.13) (Fig. 2).
According to the results of two studies reporting the fibromyalgia prevalence in the WPRO general population, this disease was observed in 1.50 and 1.70% of the population. Using fixed-effect model, the total prevalence was estimated as of 1.62% (95% confidence interval: 1.00–2.24).
Prevalence of fibromyalgia in EMRO general population was reported in two studies as of 8.30 and 0.69%. The pooled estimate of fibromyalgia prevalence in this region was 4.43% (−3.00 to 11.86) (Fig. 2). It is should be mentioned that list of countries by WHO regions presented in a supplemental file.
In 26 studies, prevalence of fibromyalgia was estimated based on ACR criteria as of 2.32% (95% confidence interval: 1.85–2.79). The total prevalences according to diagnostic methods of ACR, Fibromyalgia Impact Questionnaire (FIQ), international classification of disease (ICD 9/10), interview, London Fibromyalgia Epidemiology Study Screening Questionnaire (LFESSQ), physical examination and questionnaire self-made) are represented in Table 2 and Fig. 3.

Primary and pooled prevalences of fibromyalgia in general population according to diagnostic criteria
Prevalence of fibromyalgia in women was reported in nine studies varied from 20% in Vincent study [69] to 10.50% in Forseth study [34]. The total prevalence of fibromyalgia in women was estimated as of 3.98% (95% confidence interval: 2.80–5.20). Prevalence of fibromyalgia among men was reported in seven studies from zero in Lindell [45] and Assumpaco [18] studies to 4.80% in Vincent study [69]. The total prevalence of fibromyalgia in men was estimated as of 0.01 (0.04–0.06).
Using meta-regression models showed that publication date (β = −0.008, p = 0.884), diagnostic method (β = −0.002, p = 0.992) and WHO region (β = −0.197, p = 0.354) did not influence the heterogeneity between the results.
Prevalence of fibromyalgia in specific populations was reported in 37 studies including 109,054 subjects (Table 3). Prevalence of fibromyalgia among patients referring to the internal and rheumatology departments and clinics was reported by four primary studies varied from 14% in the study carried out by Branco [3] to 41% in the study conducted by Brill [21]. Combining the results of these studies, the total prevalence of fibromyalgia in patients visited in the internal and rheumatology departments was estimated as of 15.20% (95% confidence interval: 13.60–16.90). According to the results of three studies, prevalence of fibromyalgia among patients suffering from IBS was reported from 12.90% in Alexander study [28] to 31.60% in the Sperber study [65]. The total prevalence of fibromyalgia among IBS patients was estimated as of 12.90% (95% confidence interval: 12.70–13.10).
Prevalence of fibromyalgia among patients under hemodialysis was assessed in four studies reported from 3.90% in the study carried out by Claudio [29] to 12.20% in the study conducted by Samimagham [63]. The total prevalence of disease according to the results of these four studies was estimated as of 6.30% (95% confidence interval: 4.60–7.90). Patients with diabetes mellitus were investigated for fibromyalgia in three studies. The point prevalences varied from 9% in the study carried out by Patucchi [58] to 23.30% in the study performed by Wolak [71]. The total prevalence of fibromyalgia in these studies was estimated as of 14.80% (11.10–18.40).
Fibromyalgia was investigated in the other subpopulations such as HTLV-1-infected patients (one study), patients with vasovagal syncope (one study), full-term pregnant women (one study), Individuals exposed to the combination of physical injury and extreme stress (one study), multiple sclerosis (MS) patients (one study), cardiovascular patients (one study), subjects with chronic hepatitis B infection (one study), SLE (lupus erythematous) patients (one study), women in premenopausal and post menopausal phases referring to gynecology departments (two studies), patients with spondylitis ankylosans (one study), patients with Behcet syndrome (one study), patients with cervical radiculopathy (one study), patients with chronic disabling musculoskeletal disorders (one study), patients with idiopathic chronic urticaria (one study), patients with hereditary hemochromatosis (one study), patients with hypothalamic/hypophysis dysfunction(one study), patients with psoriasis (one study) and women with hyperprolactinemia (one study). The details of these studies are represented in Table 3. The prevalence of fibromyalgia among specific subgroups varied from 3.90% in patients undergoing hemodialysis in Claudio study [29] to 80% among patients with Behcet syndrome in the study carried out by Melikoglu [51].
Discussion
Results of our meta-analysis showed that 1.78% of the general population especially women are suffering from fibromyalgia. Although prevalence of fibromyalgia was higher in the EMRO region, the confidence intervals showed no significant difference between the WHO regions regarding the prevalence of fibromyalgia. It should be noted that most of the primary studies used ACR as the diagnostic method. Subgroup meta-analysis based on the subgroups showed prevalences of fibromyalgia as of 15.20% in patients referred to rheumatology clinic, 12.90% among IBS patients, 6.30% in hemodialysis patients and 14.80% in patients with type 2 diabetes mellitus. In addition, 80% of patients with Behcet syndrome developed fibromyalgia.
In the study conducted by Perrot et al. in 2011, prevalence of fibromyalgia among 3081 French adults aged over 18 was reported as of 1.60%) [59]. Lindell et al. conducted a study among 147 Swedish people and reported the prevalence of fibromyalgia and chronic generalized pains as of 1.30 and 4.20%, respectively [45]. These two studies were carried out in the general population without difference in the prevalences.
According to a cross-sectional study conducted by Buskila et al. among 522 patients hospitalized in the internal department, fibromyalgia diagnosed by ACR criteria in 15% of patients 91% of which were women. They found that prevalence of fibromyalgia among women was associated with age [24]. It seems that patients referring to the internal and rheumatology departments and clinics need more investigation and consideration regarding this disorder.
According to the results of a case control study conducted by Cole et al. prevalence of fibromyalgia which was diagnosed by physical examination was significantly higher among people with IBS (12.90%) compared to those without (4.70%) [28]. Therefore, fibromyalgia should be taken into consideration in patients suffering from IBS.
Kucuksen et al. conducted a study among 118 patients with episodic migraine. According to the ACR criteria, prevalence of fibromyalgia was the same among migraine patients with and without aura [43]. There is no enough evidence for this lack of relationship, and further studies are required to investigate the precise association between episodic migraine and fibromyalgia.
During a cross-sectional study among 221 patients undergoing hemodialysis, Leblebici et al. showed similar distributions of age, gender and hemodialysis duration between subjects with and without fibromyalgia. However, significant differences were observed between these two groups regarding educational level, sleeping, fatigue and cognitive symptoms [44]. Therefore, it seems that fibromyalgia is more common among hemodialysis patients.
Mohammad et al. detected 106 (57%) patients suffering from fibromyalgia among 185 chronic hepatitis C patients with mean age 48.70 years [54]. Buskila et al. found that 15 (71%) of women with hyperprolactinemia as well as 2 (4.50%) of women with normal serum prolactin had fibromyalgia detected by ACR criteria [23]. These results indicate that fibromyalgia is more common among patients with chronic hepatitis C, hyperprolactinemia and other disorders shown in the results section.
Diagnostic criteria for fibromyalgia in the primary studies were ACR, LFESSQ and FIQ. ACR is a standard questionnaire which was applied more than the other criteria. According to these criteria, chronic generalized pain more than 3 months together with tenderness in eleven of eighteen points are in accordance with fibromyalgia. Disseminated pain including pain in right and left hemilaterals, upper and lower back, axial skeleton such as cervical, dorsal, thoracic and lumbar. Diagnosis of fibromyalgia will be ruled out by any concurrent disorder [1].
Another screening method for diagnosis of fibromyalgia is LFESSQ which is successfully applied for screening of fibromyalgia in both general and specific populations. This questionnaire includes pain and fatigue as diagnostic criteria [3]. In addition, FIQ was another diagnostic method including 10 questions and is applied as an effectiveness index for treatment [20].
The current meta-analysis is prone to some limitations such as great heterogeneity between the primary results. However, we combined the results using random effect model and subgroup analysis. On the other hand, in most of the primary studies, results were not presented based on gender. Using different diagnostic methods and language bias are other limitations for our study.
Combining various prevalences of fibromyalgia in general population and different subpopulations reported in primary studies was the main strength of this meta-analysis which can be a suitable opportunity for researchers and policymakers.
Conclusion
Our study showed that prevalence of fibromyalgia in general population is considerably lower than that among populations with specific disorders. It also more common among women. In contrast to the general population, it is important to investigate this disorder among people with specific diseases. In addition, future studies should apply more accurate diagnostic criteria and represent the exact sampling tools and characteristics of the study population.
References
Naji A, Arab P (2006) Prevalence of fibromyalgia syndrome in patients referring to Shariati hospital, Terhan. Tehran Univ Med J 64(10):60–66
Topbas M, Cakirbay H, Gulec H, Akgol E, Ak I, Can G (2005) The prevalence of fibromyalgia in women aged 20–64 in Turkey. Scand J Rheumatol 34(2):140–144
Branco JC, Bannwarth B, Failde I, Carbonell JA, Blotman F, Spaeth M et al (2010) Prevalence of fibromyalgia: a survey in five European countries. Semin Arthritis Rheum 39(6):448–453
Shakibi MR, Ata-pour J, Ramezani MA (2001) Prevalence of fibromyalgia in patients referring to Kerman rheumatology clinic from 1995 to 1998. J Kerman Univ Med Sci 8(4):220–225
Santos AMB, Burti JS, Lopes JB, Scazufca M, Marques AP, Pereira RMR (2010) Prevalence of fibromyalgia and chronic widespread pain in community-dwelling elderly subjects living in São Paulo, Brazil. Maturitas 67(3):251–255
Croft P, Rigby A, Boswell R, Schollum J, Silman A (1993) The prevalence of chronic widespread pain in the general population. J Rheumatol 20(4):710–713
Bannwarth B, Blotman F, Roué-Le Lay K, Caubère J-P, André E, Taïeb C (2009) Fibromyalgia syndrome in the general population of France: a prevalence study. Joint Bone Spine 76(2):184–187
White KP, Harth M, Speechley M, Ostbye T (1999) Testing an instrument to screen for fibromyalgia syndrome in general population studies: the London Fibromyalgia Epidemiology Study Screening Questionnaire. J Rheumatol 26(4):880–884
Pincus T, Castrejón I (2012) An evidence-based medical visit for patients with rheumatoid arthritis based on standard, quantitative scientific data from a patient MDHAQ and physician report. Bull NYU Hosp Jt Dis 70(2):73–94
Moosazadeh M, Lankarani KB, Afshari M (2016) Meta-analysis of the prevalence of Helicobacter pylori infection among children and adults of Iran. Int J Prev Med 7:48
Haghshenas MR, Mousavi T, Moosazadeh M, Afshari M (2016) Human papillomavirus and breast cancer in Iran: a meta-analysis. Iran J Basic Med Sci 19(3):231–237
Kelishadi R, Haghdoost AA, Moosazadeh M, Keikha M, Aliramezany M (2015) A systematic review and meta-analysis on screening lipid disorders in the pediatric age group. J Res Med Sci 20(12):1191–1199
Von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Prev Med 45(4):247–251
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558
Ablin JN, Oren A, Cohen S, Aloush V, Buskila D, Elkayam O et al (2012) Prevalence of fibromyalgia in the Israeli population: a population-based study to estimate the prevalence of fibromyalgia in the Israeli population using the London Fibromyalgia Epidemiology Study Screening Questionnaire (LFESSQ). Clin Exp Rheumatol 30(6 Suppl 74):39–43
Almodovar R, Carmona L, Zarco P, Collantes E, Gonzalez C, Mulero J et al (2010) Fibromyalgia in patients with ankylosing spondylitis: prevalence and utility of the measures of activity, function and radiological damage. Clin Exp Rheumatol 28(6 Suppl 63):S33–S39
Andary MT, Wieting JM, Baer D, Naftulin S, Hallgren RC (2004) The prevalence of fibromyalgia in collegiate athletes. J Clin Rheumatol Pract Rep Rheum Musculoskelet Dis 10(6):323–325
Assumpcao A, Cavalcante AB, Capela CE, Sauer JF, Chalot SD, Pereira CA et al (2009) Prevalence of fibromyalgia in a low socioeconomic status population. BMC Musculoskelet Disord 10:64
Barton A, Pal B, Whorwell PJ, Marshall D (1999) Increased prevalence of sicca complex and fibromyalgia in patients with irritable bowel syndrome. Am J Gastroenterol 94(7):1898–1901
Bennett R (2005) The Fibromyalgia Impact Questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 23(5):S154
Brill S, Ablin JN, Goor-Aryeh I, Hyat K, Slefer A, Buskila D (2012) Prevalence of fibromyalgia syndrome in patients referred to a tertiary pain clinic. J Investig Med Off Publ Am Fed Clin Res 60(4):685–688
Buskila D, Ablin JN, Ben-Zion I, Muntanu D, Shalev A, Sarzi-Puttini P et al (2009) A painful train of events: increased prevalence of fibromyalgia in survivors of a major train crash. Clin Exp Rheumatol 27(5 Suppl 56):S79–S85
Buskila D, Fefer P, Harman-Boehm I, Press J, Neumann L, Lunenfeld E et al (1993) Assessment of nonarticular tenderness and prevalence of fibromyalgia in hyperprolactinemic women. J Rheumatol 20(12):2112–2115
Buskila D, Neumann L, Odes LR, Schleifer E, Depsames R, Abu-Shakra M (2001) The prevalence of musculoskeletal pain and fibromyalgia in patients hospitalized on internal medicine wards. Semin Arthritis Rheum 30(6):411–417
Carranza-Lira S, Hernandez IB (2014) Prevalence of fibromyalgia in premenopausal and postmenopausal women and its relation to climacteric symptoms. Przeglad menopauzalny Menopause Rev 13(3):169–173
Clark P, Burgos-Vargas R, Medina-Palma C, Lavielle P, Marina FF (1998) Prevalence of fibromyalgia in children: a clinical study of Mexican children. J Rheumatol 25(10):2009–2014
Cobankara V, Unal UO, Kaya A, Bozkurt AI, Ozturk MA (2011) The prevalence of fibromyalgia among textile workers in the city of Denizli in Turkey. Int J Rheum Dis 14(4):390–394
Cole JA, Rothman KJ, Cabral HJ, Zhang Y, Farraye FA (2006) Migraine, fibromyalgia, and depression among people with IBS: a prevalence study. BMC Gastroenterol 6:26
Couto CI, Natour J, Carvalho AB (2008) Fibromyalgia: its prevalence and impact on the quality of life on a hemodialyzed population. Hemodial Int Int Symp Home Hemodial 12(1):66–72
Cruz BA, Catalan-Soares B, Proietti F (2006) Higher prevalence of fibromyalgia in patients infected with human T cell lymphotropic virus type I. J Rheumatol 33(11):2300–2303
Davatchi F, Tehrani Banihashemi A, Gholami J, Faezi ST, Forouzanfar MH, Salesi M et al (2009) The prevalence of musculoskeletal complaints in a rural area in Iran: a WHO-ILAR COPCORD study (stage 1, rural study) in Iran. Clin Rheumatol 28(11):1267–1274
Demir SE, Aytekin E, Karacan I, Aydin T, Kavadar GD (2014) The prevalence of fibromyalgia among patients with cervical radiculopathy due to cervical disc herniation: a pilot study. J Back Musculoskelet Rehabil 27(2):167–171
Durmaz Y, Alayli G, Canbaz S, Zahiroglu Y, Bilgici A, Ilhanli I et al (2013) Prevalence of juvenile fibromyalgia syndrome in an urban population of Turkish adolescents: impact on depressive symptoms, quality of life and school performance. Chin Med J 126(19):3705–3711
Forseth KO, Gran JT (1992) The prevalence of fibromyalgia among women aged 20–49 years in Arendal, Norway. Scand J Rheumatol 21(2):74–78
Goulding C, O’Connell P, Murray FE (2001) Prevalence of fibromyalgia, anxiety and depression in chronic hepatitis C virus infection: relationship to RT-PCR status and mode of acquisition. Eur J Gastroenterol Hepatol 13(5):507–511
Harbeck B, Sufke S, Harten P, Haas CS, Lehnert H, Monig H (2013) High prevalence of fibromyalgia-associated symptoms in patients with hypothalamic-pituitary disorders. Clin Exp Rheumatol 31(6 Suppl 79):S16–S21
Harvey CK (1993) Fibromyalgia. Part II. Prevalence in the podiatric patient population. J Am Podiatr Med Assoc 83(7):416–417
Haviland MG, Banta JE, Przekop P (2011) Fibromyalgia: prevalence, course, and co-morbidities in hospitalized patients in the United States, 1999–2007. Clin Exp Rheumatol 29(6 Suppl 69):S79–S87
Howard KJ, Mayer TG, Neblett R, Perez Y, Cohen H, Gatchel RJ (2010) Fibromyalgia syndrome in chronic disabling occupational musculoskeletal disorders: prevalence, risk factors, and posttreatment outcomes. J Occup Environ Med Am Coll Occup Environ Med 52(12):1186–1191
Ifergane G, Buskila D, Simiseshvely N, Zeev K, Cohen H (2006) Prevalence of fibromyalgia syndrome in migraine patients. Cephalalgia Int J Headache 26(4):451–456
Jones GT, Atzeni F, Beasley M, Fluss E, Sarzi-Puttini P, Macfarlane GJ (2015) The prevalence of fibromyalgia in the general population: a comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol (Hoboken, NJ) 67(2):568–575
Kim C, Kim H, Kim J (2012) Prevalence of chronic widespread pain and fibromyalgia syndrome: a Korean hospital-based study. Rheumatol Int 32(11):3435–3442
Kucuksen S, Genc E, Yilmaz H, Salli A, Gezer IA, Karahan AY et al (2013) The prevalence of fibromyalgia and its relation with headache characteristics in episodic migraine. Clin Rheumatol 32(7):983–990
Leblebici B, Ozelsancak R, Yilmaz EE, Doruk P (2016) Fibromyalgia syndrome in Turkish hemodialysis patients. Hemodial Int Int Symp Home Hemodial 20(1):106–110
Lindell L, Bergman S, Petersson IF, Jacobsson LT, Herrstrom P (2000) Prevalence of fibromyalgia and chronic widespread pain. Scand J Prim Health Care 18(3):149–153
Lundberg G, Gerdle B (2002) Tender point scores and their relations to signs of mobility, symptoms, and disability in female home care personnel and the prevalence of fibromyalgia syndrome. J Rheumatol 29(3):603–613
Okumus M, Parpucu H, Kocaoglu S, Ceceli E, Duranay M, Borman P (2012) The frequency of fibromyalgia syndrome and the quality of life in patients with peritoneal dialysis. Open J Rheumatol Autoimmune Dis 2(4):88–93
Mäkelä M, Heliövaara M (1991) Prevalence of primary fibromyalgia in the Finnish population. BMJ Br Med J 303(6796):216–219
Marrie RA, Yu BN, Leung S, Elliott L, Warren S, Wolfson C et al (2012) The incidence and prevalence of fibromyalgia are higher in multiple sclerosis than the general population: a population-based study. Multiple Scler Relat Disord 1(4):162–167
Mas AJ, Carmona L, Valverde M, Ribas B (2008) Prevalence and impact of fibromyalgia on function and quality of life in individuals from the general population: results from a nationwide study in Spain. Clin Exp Rheumatol 26(4):519–526
Melikoglu M, Melikoglu MA (2013) The prevalence of fibromyalgia in patients with Behcet’s disease and its relation with disease activity. Rheumatol Int 33(5):1219–1222
Middleton GD, McFarlin JE, Lipsky PE (1994) The prevalence and clinical impact of fibromyalgia in systemic lupus erythematosus. Arthritis Rheum 37(8):1181–1188
Guermazi M, Ghroubi S, Sellami M, Elleuch M, Feki H, André E et al (2008) Fibromyalgia prevalence in TUNISIA. Tunis Med 86(9):806–811
Mohammad A, Carey JJ, Storan E, Scarry M, Coughlan RJ, Lee JM (2012) Prevalence of fibromyalgia among patients with chronic hepatitis C infection: relationship to viral characteristics and quality of life. J Clin Gastroenterol 46(5):407–412
Mohammad A, Carey JJ, Storan E, Scarry M, Coughlan RJ, Lee JM (2013) High prevalence of fibromyalgia in patients with HFE-related hereditary hemochromatosis. J Clin Gastroenterol 47(6):559–564
Nunes FR, Ferreira JM, Bahamondes L (2014) Prevalence of fibromyalgia and quality of life in women with and without endometriosis. Gynecol Endocrinol Off J Int Soc Gynecol Endocrinol 30(4):307–310
Ozsahin M, Gonen I, Ermis F, Oktay M, Besir FH, Kutlucan A et al (2013) The prevalence of fibromyalgia among patients with hepatitis B virus infection. Int J Clin Exp Med 6(9):804–808
Patucchi E, Fatati G, Puxeddu A, Coaccioli S (2003) Prevalence of fibromyalgia in diabetes mellitus and obesity. Recenti Prog Med 94(4):163–165
Perrot S, Vicaut E, Servant D, Ravaud P (2011) Prevalence of fibromyalgia in France: a multi-step study research combining national screening and clinical confirmation: the DEFI study (Determination of Epidemiology of FIbromyalgia). BMC Musculoskelet Disord 12:224
Prescott E, Kjoller M, Jacobsen S, Bulow PM, Danneskiold-Samsoe B, Kamper-Jorgensen F (1993) Fibromyalgia in the adult Danish population: I. A prevalence study. Scand J Rheumatol 22(5):233–237
Rusu C, Gee ME, Lagace C, Parlor M (2015) Chronic fatigue syndrome and fibromyalgia in Canada: prevalence and associations with six health status indicators. Health Promot Chronic Dis Prevent Canada Res Policy Pract 35(1):3–11
Saa’d S, Many A, Jacob G, Ablin JN (2013) High prevalence of fibromyalgia symptoms among healthy full-term pregnant women. Rheumatol Int 33(6):1555–1560
Samimagham H, Haghighi A, Tayebi M, Jenabi A, Arabi M, Kianmehr N (2014) Prevalence of fibromyalgia in hemodialysis patients. Iran J Kidney Dis 8(3):236–239
Sauer K, Kemper C, Glaeske G (2011) Fibromyalgia syndrome: prevalence, pharmacological and non-pharmacological interventions in outpatient health care. An analysis of statutory health insurance data. Joint Bone Spine revue du rhumatisme 78(1):80–84
Sperber AD, Atzmon Y, Neumann L, Weisberg I, Shalit Y, Abu-Shakrah M et al (1999) Fibromyalgia in the irritable bowel syndrome: studies of prevalence and clinical implications. Am J Gastroenterol 94(12):3541–3546
Thune PO (2005) The prevalence of fibromyalgia among patients with psoriasis. Acta Dermato-venereologica 85(1):33–37
Toda K (2007) The prevalence of fibromyalgia in Japanese workers. Scand J Rheumatol 36(2):140–144
Vallejo M, Martínez-Martínez L-A, Grijalva-Quijada S, Olguín-Ruvalcaba H-M, Salas E, Hermosillo AG et al (2013) Prevalence of fibromyalgia in vasovagal syncope. JCR J Clin Rheumatol 19(3):111–114
Vincent A, Lahr BD, Wolfe F, Clauw DJ, Whipple MO, Oh TH et al (2013) Prevalence of fibromyalgia: a population-based study in Olmsted County, Minnesota, utilizing the Rochester Epidemiology Project. Arthritis Care Res 65(5):786–792
Walitt B, Nahin RL, Katz RS, Bergman MJ, Wolfe F (2015) The prevalence and characteristics of fibromyalgia in the 2012 National Health Interview Survey. PLoS One 10(9):e0138024
Wolak T, Weitzman S, Harman-Boehm I, Friger M, Sukenik S (2001) Prevalence of fibromyalgia in type 2 diabetes mellitus. Harefuah 140(11):1006–9, 120, 119
Wolfe F, Brahler E, Hinz A, Hauser W (2013) Fibromyalgia prevalence, somatic symptom reporting, and the dimensionality of polysymptomatic distress: results from a survey of the general population. Arthritis Care Res 65(5):777–785
Yanmaz MN, Mert M, Korkmaz M (2012) The prevalence of fibromyalgia syndrome in a group of patients with diabetes mellitus. Rheumatol Int 32(4):871–874
Yener M, Erturan I, Ceyhan AM, Inal EE, Kazanoglu OO (2013) The evaluation of prevalence of fibromyalgia in patients with chronic urticaria. Med Sci Monit Int Med J Exp Clin Res 19:757–761
Acknowledgements
This study has been registered in the Ethics Committee of Mazandaran University of Medical Sciences and supported by Research Deputy of this university (Project Number: 551). The authors would like to thank Research Deputy Coordinator of Mazandaran for kindly cooperation.
Author information
Authors and Affiliations
Contributions
FH and MM carried out the design, performed the literature searches of the study, screened titles, abstracted data, and performed data analysis. MA participated in provided of drafted the manuscript and helped to analysis the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Heidari, F., Afshari, M. & Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol Int 37, 1527–1539 (2017). https://doi.org/10.1007/s00296-017-3725-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3725-2