
Abstract
Purpose
Methotrexate (MTX)/6-Mercaptopurine (6MP)-based maintenance therapy is crucial to cure childhood acute lymphoblastic leukemia (ALL). Cytotoxicity is mediated by incorporation of thioguanine nucleotides (TGN) into DNA (DNA-TG) with higher levels in leucocytes being associated with reduced relapse risk. To further understand the dynamics of DNA-TG formation, we measured DNA-TG levels in leucocyte subsets during maintenance therapy and in the months following its discontinuation.
Methods
DNA-TG levels were measured in leucocytes (DNA-TGTotal), polymorph nucleated granulocytes (neutrophils, eosinophils, basophils [DNA-TGPMN]) and mononucleated cells (lymphocytes, monocytes [DNA-TGMNC]) in 1013 samples from 52 patients on ALL maintenance therapy (951 samples during therapy and 62 samples after therapy discontinuation, respectively).
Results
Median DNA-TGTotal, DNA-TGPMN and DNA-TGMNC during maintenance therapy were 539, 563 and 384 fmol/µg DNA, respectively. DNA-TGPMN displayed more pronounced fluctuation than DNA-TGMNC (range 0–3084 [interquartile range IQR 271–881] versus 30–1411 [IQR 270–509] fmol/µg DNA). DNA-TGTotal was more strongly correlated with DNA-TGPMN (rS = 0.95, p < 0.0001) than DNA-TGMNC (rS = 0.73, p < 0.0001). DNA-TGPMN correlated less with DNA-TGMNC (rS = 0.64, p < 0.0001) and to a much lesser extent with absolute neutrophil count (rS = 0.35, p < 0.0001). Following discontinuation of therapy, DNA-TGPMN was rapidly eliminated, and not measurable beyond day 22 after discontinuation, whereas DNA-TGMNC was slowly eliminated, and five patients demonstrated a measurable DNA-TGMNC more than 365 days after therapy discontinuation.
Conclusion
Fluctuations in DNA-TGTotal are predominantly caused by corresponding fluctuations in DNA-TGPMN, thus DNA-TGTotal measures recent TGN incorporation in these short-lived cells. Measurement of DNA-TGTotal at 2–4 weeks intervals provides a reliable profile of DNA-TG levels.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Survival rate of childhood acute lymphoblastic leukemia (ALL) has improved tremendously over the last decades and now surpasses 90% in children receiving the best contemporary therapy [1, 2]. Methotrexate (MTX) and 6-Mercaptopurine (6MP)-based maintenance therapy constitutes a key element of ALL therapy [3]. To adjust for the substantial inter-individual variability in MTX and 6MP pharmacokinetics, maintenance therapy doses are guided by degree of myelosuppression, i.e. by white blood cell count (WBC) or absolute neutrophil count (ANC), which have been associated with relapse rates [4,5,6,7,8,9]. WBC is, however, confounded by substantial natural variation with gender, age, circadian fluctuations and ethnicity, and is therefore a weak surrogate parameter for MTX/6MP treatment intensity [10,11,12]. Insufficient treatment intensity during maintenance therapy has alongside shortening of maintenance therapy been related to a poorer ALL outcome, thus emphasizing the importance of effective maintenance therapy and warranting identification of a better indicator of MTX/6MP treatment efficacy [3, 13,14,15,16]. Thioguanine nucleotides (TGN) are the primary mediators of 6MP cytotoxicity and compete with guanine for incorporation into DNA (DNA-TG) [17]. Incorporated TGN undergo random methylation, which favors mismatch between TGN and thymidine. This results in repetitive but futile attempts of mismatch repair, which ultimately leads to cell death catalyzed by the mismatch repair system [18,19,20]. Both methylated 6MP metabolites and MTX inhibit purine de novo synthesis, and concomitant administration of MTX therefore enhances DNA-TG formation, due to decreased guanine availability [17, 21,22,23,24].
Higher leucocyte DNA-TG levels during maintenance therapy have been shown to be associated with decreased relapse rates [15]. This argues for a potential advantage of adjusting maintenance therapy according to DNA-TG level, thus aiming to reduce risk of relapse through increased DNA-TG. To further understand the dynamics of DNA-TG incorporation, we studied DNA-TG levels in leucocytes and leucocyte subsets during maintenance therapy and in the months following its discontinuation.
Materials and methods
Study participants
Study patients were aged 1–18 years at ALL diagnosis and included from May 2016 to November 2018. Patients were treated according to the Nordic Society of Pediatric Hematology and Oncology (NOPHO) ALL2008 protocol at the Department of Pediatrics and Adolescent Medicine, Rigshospitalet, University of Copenhagen, Denmark. Risk grouping and therapy details of the NOPHO ALL2008 protocol have been published previously elsewhere [1, 25, 26]. Eligible patients were those who had started maintenance therapy in first remission and had at least one DNA-TG measurement available in leucocytes and subsets during maintenance therapy.
The study was approved by the Ethical Committee of the Capital Region of Denmark (H-2.2010-002), and written informed consent was secured from all participants or their legal guardians.
Maintenance therapy, NOPHO ALL2008 protocol
Maintenance therapy is divided into two therapy phases: Maintenance-I and maintenance-II. The fundament of both phases of maintenance therapy is daily oral 6MP and weekly oral MTX irrespective of risk group stratification, and dose adjustments during maintenance therapy is targeted to achieve a WBC target of 1.5–3.0 × 109/L. Patients with standard risk (SR), intermediate risk (IR) and high risk (HR) ALL start maintenance-I in week 20, 22 and 36 following diagnosis, respectively. For patients with SR and IR ALL maintenance-I contains alternating pulses every fourth week with either vincristine (2.0 mg/m2 once; total five times for SR, and four times for IR patients) and dexamethasone (6 mg/m2 for 5 days) or high-dose MTX (5.0 g/m2/24 h iv, five times). Patients were further randomized as part of a NOPHO ALL2008 phase 3 study to receive intramuscular pegylated-asparaginase administrations either every second (total of ten administrations) or sixth week (total of three administrations) until week 33. Results of this study have been published in detail elsewhere [27, 28]. Patients with HR ALL receive three high-dose intravenous MTX administrations at 24-week intervals during maintenance-I.
Moreover, patients receive intrathecal MTX during maintenance-I, which for patients with IR ALL is supplemented with prednisolone and cytarabine in case of central nervous system leukemia at diagnosis (triple intrathecal therapy [TIT]), and patients with HR ALL receive alternating TIT and intrathecal MTX during maintenance-I.
After maintenance-I, patients with SR ALL continue directly to maintenance-II, which is the last phase of therapy in the NOPHO ALL2008 protocol. Patients with SR ALL enter maintenance-II in week 58 following diagnosis, whereas patients with IR and HR ALL receive 6 weeks of delayed intensification before entering maintenance-II in week 66 and 105, respectively. Patients with IR and HR ALL continue to receive intrathecal chemotherapy in addition to oral 6MP and oral MTX during maintenance-II until discontinuation of antileukemic therapy 2.5 years after diagnosis.
DNA-TG quantification
Blood samples for metabolite measurements were only drawn, when blood samples were otherwise indicated to evaluate ALL therapy. On the same day, patients had complete blood counts evaluated, including WBC, ANC, absolute lymphocyte count (ALC), monocytes, eosinophils, basophils, and thrombocytes.
DNA-TG level was quantified as a total in circulating leucocytes (DNA-TGTotal), and furthermore in polymorph nucleated granulocytes, i.e. neutrophils, eosinophils and basophils (DNA-TGPMN) and in mononucleated cells, i.e. lymphocytes and monocytes (DNA-TGMNC). The gradient medium, Lymphoprep™ (Abbott) 1.077 ± 0.001 g/mL was used for separation into polymorph nucleated granulocytes and mononucleated cells.
For the quantification of DNA-TG, the same method was applied to determine DNA-TGTotal, DNA-TGPMN and DNA-TGMNC; 1 − 2 μg DNA was purified, de-purinized and subsequently ethenoderivatized using chloroacetaldehyde. Following normalization with the respective isotope internal standards, the ratios of thioguanine and guanine were calculated. Ratios were quantified with ultra-performance liquid chromatography tandem mass spectrometry and reported as fmol TGN/μg DNA. With 1 μg DNA per sample, the limit of detection was 4.2 fmol/μg DNA and the limit of quantification 14.1 fmol/μg DNA, with intraday and interday relative standard deviations of less than 11%, and an analytical linearity up to a minimum of 10,000 fmol/μg [29].
For the analysis, DNA-TG values in the range 1–29 fmol/µg DNA were set to 30 fmol/µg DNA, i.e. approximately twice the lowest quantifiable level, as this was the lowest standard in the applied DNA-TG analysis. A DNA-TG of 100 fmol/μg DNA corresponds approximately to a median ratio of incorporation of 1:30,000 nucleobases.
Outcomes
The objectives of this study were to (1) identify the primary determinator of DNA-TGTotal among DNA-TGPMN and DNA-TGMNC, (2) describe fluctuations in DNA-TGTotal and in subsets during maintenance therapy, (3) investigate the quality of separation into DNA-TGPMN and DNA-TGMNC, and (4) describe DNA-TG elimination after cessation of therapy as a surrogate parameter for the dynamics of DNA-TG incorporation.
Statistical analysis
Spearman correlations between DNA-TG measurements and blood counts were estimated with p-values based on cluster-robust standard errors to account for multiple measurements per patient. Patient levels of DNA-TG were calculated as medians of each patient’s DNA-TG measurements, and the distributions of these were compared between independent groups with Mann–Whitney test. Patient coefficients of variation were calculated for each patient as the ratio of the standard deviation to the mean and were compared between DNA-TG subgroups with Wilcoxon signed-rank test.
To evaluate the quality of our separation into polymorph nucleated granulocytes and mononucleated cells, we calculated DNA-TGTotal from DNA-TGPMN, DNA-TGMNC and the blood counts, when all measurements were available from the same day for the same patient as:
These were compared with the measured DNA-TGTotal with Wilcoxon signed-rank test.
Statistical analyses were performed using R version 4.0.0.
Results
A total of 52 patients were included (patient characteristics are summarized in Table 1), and a total of 1013 samples were available for analysis. Of the 1013 samples, 951 samples were taken during maintenance-I and maintenance-II (median 15.5 per patient, range 2–50), and 62 samples were taken after discontinuation of therapy.
All samples taken during maintenance therapy did not include all blood counts (as shown in Online Resource 1) and/or DNA-TG measurements (Table 2); hence, a total of 939 DNA-TGTotal, 947 DNA-TGPMN, and 937 DNA-TGMNC measurements taken during maintenance therapy were available. Neutrophils and lymphocytes constituted by far the largest proportion of polymorph nucleated granulocytes and mononucleated cells, respectively. Hence, DNA-TGPMN and DNA-TGMNC are regarded to predominantly reflect DNA-TG levels in neutrophils and in lymphocytes, respectively (Online Resource 1).
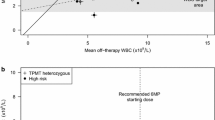
Median DNA-TGTotal, median DNA-TGPMN, and median DNA-TGMNC of all samples during maintenance therapy were 539, 563, and 384 fmol/µg DNA, respectively (Fig. 1a–c, Table 2).

a–c Level of thioguanine nucleotides incorporated into DNA (DNA-TG) during maintenance therapy. a DNA-TGTotal, DNA-TG level in leucocytes. b DNA-TGPMN, DNA-TG level in polymorph nucleated granulocytes (neutrophils, eosinophils, basophils). c DNA-TGMNC, DNA-TG level in mononucleated cells (lymphocytes, monocytes). All DNA-TG levels are reported in fmol/µg DNA
DNA-TGTotal was more strongly correlated with DNA-TGPMN (rs = 0.95) than DNA-TGMNC (rs = 0.73, both p < 0.0001) Fig. 2a, b), whereas DNA-TGPMN to a lesser extent was correlated with DNA-TGMNC (rs = 0.64). DNA-TGPMN was to a much lesser extent correlated with ANC (rs = 0.35, p < 0.0001, Fig. 2c). A comparable poor correlation was also observed between DNA-TGMNC and ALC (rs = − 0.22, p < 0.01, Fig. 2d).

a–d Correlation plots of levels of thioguanine nucleotides incorporated into DNA (DNA-TG) during maintenance therapy. DNA-TGTotal, DNA-TG level in leucocytes; DNA-TGPMN, DNA-TG level in polymorph nucleated granulocytes (neutrophils, eosinophils, basophils); DNA-TGMNC, DNA-TG level in mononucleated cells (lymphocytes, monocytes). a DNA-TGTotal versus DNA-TGPMN. b DNA-TGTotal versus DNA-TGMNC. c DNA-TGPMN versus absolute neutrophil count (ANC). d DNA-TGMNC versus absolute lymphocyte count (ALC). All DNA-TG levels are reported in fmol/µg DNA
DNA-TGPMN fluctuated with a range of 0–3084 fmol/µg DNA during maintenance therapy, and DNA-TGMNC with a range of 30–1411 fmol/µg DNA. Median patient coefficients of variation (i.e. one coefficient of variation from each patient including all of their respective measurements) for DNA-TGTotal, DNA-TGPMN and DNA-TGMNC were 0.55 (interquartile range [IQR] 0.45–0.62), 0.67 (IQR 0.53–0.77) and 0.36 (IQR 0.29–0.44), respectively. The distribution of coefficients of variation for DNA-TGPMN differed significantly from the distribution for DNA-TGMNC (p < 0.0001).
The distributions of patient levels from all patients are summarized for the SR and IR groups and according to maintenance therapy phase in Table 3. The HR risk group was not reported here due to small patient numbers.
Including all patients, DNA-TGPMN was significantly higher in patients with SR ALL compared with patients with IR ALL during maintenance-I (median 494 versus 275 fmol/µg DNA, respectively, p = 0.03). Age did not differ between patients in the two risk groups (p = 0.98). There were no other significant differences in DNA-TG levels, when comparing patients with SR ALL with patients with IR ALL.
A subset of 18 patients had at least one DNA-TG measurement available from both maintenance-I and maintenance-II. Comparison of DNA-TG levels from these patients showed that DNA-TGTotal was significantly higher in maintenance-II compared with maintenance-I (p < 0.001). In this subset of patients, the median DNA-TGTotal was 335 fmol/µg DNA during maintenance-I, and 719 fmol/µg DNA during maintenance-II.
Confirming the quality of separation into polymorph nucleated granulocytes and mononucleated cells, we found that measured DNA-TGTotal was strongly correlated with the calculated DNA-TGTotal (rs = 0.96). The measured DNA-TGTotal was on average 7.7% higher than the calculated DNA-TGTotal (IQR 0.7–16.7%).
To describe DNA-TG elimination as a surrogate parameter for incorporation dynamics, a total of 62 samples from a median of 122 days after discontinuation of therapy (range 1–619, IQR 37–247) were available from 20 patients (11 males) with 1–7 DNA-TGTotal samples per patient (median 3). Of the total 62 samples, six samples from five patients demonstrated a measurable DNA-TGPMN after discontinuation of therapy (i.e. above 30 fmol/µg DNA). These samples were all taken between 1 and 22 days after discontinuation of therapy and the patients had subsequently a sample of 30 or below. Beyond day 22 after discontinuation of therapy, no patients demonstrated a measurable DNA-TGPMN. In comparison, DNA-TGMNC was very slowly eliminated. Six patients had a DNA-TGMNC sample available more than 365 days after discontinuation of therapy, of which five patients demonstrated a measurable DNA-TGMNC at this time point (range 35–110 fmol/µg DNA).
Discussion
Sufficient treatment intensity during maintenance therapy is crucial to ensure lasting remission of ALL. The persistent challenge has been to identify an optimal parameter to monitor for MTX/6MP treatment intensity. Historical strategies have been based on WBC or ANC, as sustained myelosuppression has been strongly associated with relapse rates [4, 7,8,9]. The inherent weakness of WBC to reflect MTX/6MP cytotoxicity (WBC fluctuates according to gender, ethnicity, age, infection and circadian rhythms [10,11,12]) is, however, a tremendous challenge to this strategy.
The cytotoxicity of maintenance therapy is based on formation of DNA-TG [17]. In the NOPHO ALL2008 maintenance therapy sub-study, it was shown that higher leucocyte DNA-TG levels during maintenance therapy were associated with decreased relapse rates [15]. The relapse hazard was reduced by 28% for every 100 fmol/µg DNA increase in DNA-TG, without signs of plateauing of the effect [15]. It was further demonstrated that DNA-TG levels were neither associated with MTX/6MP doses, nor associated with ANC or ALC during maintenance therapy [15]. MTX/6MP dose intensity and degree of myelosuppression can therefore not predict the DNA-TG level [15], which is consistent with the poor correlations we observed between DNA-TGPMN and ANC, as well as between DNA-TGMNC and ALC.
We observed that DNA-TGPMN was significantly higher during maintenance-I in patients with SR ALL compared with patients with IR ALL. Potential explanations could be that treatment prior to maintenance-I is notably more intensive for patients with IR ALL compared with patients with SR ALL. This could render the bone-marrow of IR patients with a different turnover, thus resulting in an altered pattern of DNA-TG incorporation. Further, the behavior of the treating physician might be influenced by the more intensive treatment for patients with IR ALL prior to maintenance-I, thus making their dosing strategy during maintenance-I less “aggressive” to obtain WBC target. Patients with IR ALL “catch up” during maintenance-II, where no significant difference was observed with regards to DNA-TG level.
DNA-TG level seems to represent an integrated measure of MTX/6MP cytotoxicity, and titration of MTX/6MP therapy according to DNA-TG level could therefore be a superior alternative to WBC/ANC aiming to reduce risk of relapse through increased DNA-TG. Thus, DNA-TG level holds the potential to serve as a dose adjustment parameter during maintenance therapy, and exploration of this potential in a therapeutic drug monitoring setting is currently investigated in the Thiopurine Enhanced ALL Maintenance therapy study (clinicaltrials.gov NCT02912676).
Present results highlighted the strong correlation between DNA-TGTotal and DNA-TGPMN, and for multicenter studies DNA-TGTotal can be used as a surrogate biomarker for the most recent build-up of DNA-TG in dividing cells due to the stability of DNA and additionally without the need to perform cell separation. Further, DNA-TGTotal and DNA-TGPMN displayed similar fluctuations during maintenance therapy, whereas DNA-TGMNC was much less variable. This was emphasized by the coefficients of variation, and further underlined by DNA-TGMNC displaying an IQR nearly half the size of the corresponding interval for DNA-TGTotal and DNA-TGPMN.
As lifespan for neutrophils is 0.5–1 day versus months to years for lymphocytes, the results of the present study are well explained. Due to the short lifespan of neutrophils (constituting the majority of the PMN fraction), the turnover of DNA-TG will be rapid, and thus prone to fluctuations, and due to the strong correlation between DNA-TGTotal and DNA-TGPMN, these wide fluctuations are also observed in DNA-TGTotal. The short neutrophil turnover results in a rapid TGN incorporation, which was also confirmed by the observed very rapid elimination of DNA-TGPMN after discontinuation of therapy.
Further, we hypothesized that elimination of DNA-TG after discontinuation of therapy was a surrogate parameter for the dynamics of DNA-TG incorporation. This is an approximation as lifespan of cells can change. However, elimination of DNA-TG was shown to be a two compartmental model, with a very rapid elimination in neutrophils and a far more prolonged elimination of DNA-TG in lymphocytes. Due to origin of the malignant clone, a clinical significance of both a higher DNA-TGMNC after completion of therapy as well as a prolonged elimination could be speculated. Data were however too limited to address this.
Conclusion
Fluctuations in DNA-TGTotal are predominantly caused by corresponding fluctuations in DNA-TGPMN. Measurements of DNA-TGTotal during maintenance therapy therefore primarily reflect recent TGN incorporation in the short-lived neutrophils. Due to this association and based on the observed elimination characteristics of DNA-TGPMN after discontinuation of therapy, measurement of DNA-TGTotal at 2–4 weeks intervals will provide a reliable profile of DNA-TG level during maintenance therapy.
References
Toft N, Birgens H, Abrahamsson J, Griskevicius L, Hallbook H, Heyman M, Klausen TW, Jonsson OG, Palk K, Pruunsild K, Quist-Paulsen P, Vaitkeviciene G, Vettenranta K, Asberg A, Frandsen TL, Marquart HV, Madsen HO, Noren-Nystrom U, Schmiegelow K (2018) Results of NOPHO ALL2008 treatment for patients aged 1–45 years with acute lymphoblastic leukemia. Leukemia 32(3):606–615. https://doi.org/10.1038/leu.2017.265
Hunger SP, Mullighan CG (2015) Acute lymphoblastic leukemia in children. N Engl J Med 373(16):1541–1552. https://doi.org/10.1056/NEJMra1400972
Schmiegelow K, Nielsen SN, Frandsen TL, Nersting J (2014) Mercaptopurine/Methotrexate maintenance therapy of childhood acute lymphoblastic leukemia: clinical facts and fiction. J Pediatr Hematol Oncol 36(7):503–517. https://doi.org/10.1097/mph.0000000000000206
Schmiegelow K, Nersting J, Nielsen SN, Heyman M, Wesenberg F, Kristinsson J, Vettenranta K, Schroeder H, Weinshilboum R, Jensen KL, Grell K, Rosthoej S (2016) Maintenance therapy of childhood acute lymphoblastic leukemia revisited-Should drug doses be adjusted by white blood cell, neutrophil, or lymphocyte counts? Pediatr Blood Cancer 63(12):2104–2111. https://doi.org/10.1002/pbc.26139
Balis FM, Holcenberg JS, Poplack DG, Ge J, Sather HN, Murphy RF, Ames MM, Waskerwitz MJ, Tubergen DG, Zimm S, Gilchrist GS, Bleyer WA (1998) Pharmacokinetics and pharmacodynamics of oral methotrexate and mercaptopurine in children with lower risk acute lymphoblastic leukemia: a joint children’s cancer group and pediatric oncology branch study. Blood 92(10):3569–3577
Zimm S, Collins JM, Riccardi R, O’Neill D, Narang PK, Chabner B, Poplack DG (1983) Variable bioavailability of oral mercaptopurine. Is maintenance chemotherapy in acute lymphoblastic leukemia being optimally delivered. N Engl J Med 308(17):1005–1009. https://doi.org/10.1056/NEJM198304283081705
Lucas K, Gula MJ, Blatt J (1992) Relapse in acute lymphoblastic leukemia as a function of white blood cell and absolute neutrophil counts during maintenance chemotherapy. Pediatr Hematol Oncol 9(2):91–97
Hayder S, Bjork O, Nilsson B (1992) Relapse factors during maintenance therapy of acute lymphoblastic leukemia in children. Pediatr Hematol Oncol 9(1):21–27
Dolan G, Lilleyman JS, Richards SM (1989) Prognostic importance of myelosuppression during maintenance treatment of lymphoblastic leukaemia. Leukaemia in childhood working party of the medical research council. Arch Dis Childhood 64(9):1231–1234
Haus E, Smolensky MH (1999) Biologic rhythms in the immune system. Chronobiol Int 16(5):581–622
Nielsen SN, Grell K, Nersting J, Frandsen TL, Hjalgrim LL, Schmiegelow K (2016) Measures of 6-mercaptopurine and methotrexate maintenance therapy intensity in childhood acute lymphoblastic leukemia. Cancer Chemother Pharmacol 78(5):983–994. https://doi.org/10.1007/s00280-016-3151-2
Haddy TB, Rana SR, Castro O (1999) Benign ethnic neutropenia: what is a normal absolute neutrophil count? J Lab Clin Med 133(1):15–22. https://doi.org/10.1053/lc.1999.v133.a94931
Toyoda Y, Manabe A, Tsuchida M, Hanada R, Ikuta K, Okimoto Y, Ohara A, Ohkawa Y, Mori T, Ishimoto K, Sato T, Kaneko T, Maeda M, Koike K, Shitara T, Hoshi Y, Hosoya R, Tsunematsu Y, Bessho F, Nakazawa S, Saito T (2000) Six months of maintenance chemotherapy after intensified treatment for acute lymphoblastic leukemia of childhood. J Clin Oncol 18(7):1508–1516. https://doi.org/10.1200/jco.2000.18.7.1508
Riehm H, Gadner H, Henze G, Kornhuber B, Lampert F, Niethammer D, Reiter A, Schellong G (1990) Results and significance of six randomized trials in four consecutive ALL-BFM studies. Haematol Blood Transfus 33:439–450. https://doi.org/10.1007/978-3-642-74643-7_81
Nielsen SN, Grell K, Nersting J, Abrahamsson J, Lund B, Kanerva J, Jonsson OG, Vaitkeviciene G, Pruunsild K, Hjalgrim LL, Schmiegelow K (2017) DNA-thioguanine nucleotide concentration and relapse-free survival during maintenance therapy of childhood acute lymphoblastic leukaemia (NOPHO ALL2008): a prospective substudy of a phase 3 trial. Lancet Oncol 18(4):515–524. https://doi.org/10.1016/s1470-2045(17)30154-7
Kato M, Ishimaru S, Seki M, Yoshida K, Shiraishi Y, Chiba K, Kakiuchi N, Sato Y, Ueno H, Tanaka H, Inukai T, Tomizawa D, Hasegawa D, Osumi T, Arakawa Y, Aoki T, Okuya M, Kaizu K, Kato K, Taneyama Y, Goto H, Taki T, Takagi M, Sanada M, Koh K, Takita J, Miyano S, Ogawa S, Ohara A, Tsuchida M, Manabe A (2017) Long-term outcome of 6-month maintenance chemotherapy for acute lymphoblastic leukemia in children. Leukemia 31(3):580–584. https://doi.org/10.1038/leu.2016.274
Karran P, Attard N (2008) Thiopurines in current medical practice: molecular mechanisms and contributions to therapy-related cancer. Nat Rev Cancer 8(1):24–36. https://doi.org/10.1038/nrc2292
Diouf B, Cheng Q, Krynetskaia NF, Yang W, Cheok M, Pei D, Fan Y, Cheng C, Krynetskiy EY, Geng H, Chen S, Thierfelder WE, Mullighan CG, Downing JR, Hsieh P, Pui CH, Relling MV, Evans WE (2011) Somatic deletions of genes regulating MSH2 protein stability cause DNA mismatch repair deficiency and drug resistance in human leukemia cells. Nat Med 17(10):1298–1303. https://doi.org/10.1038/nm.2430
Waters TR, Swann PF (1997) Cytotoxic mechanism of 6-thioguanine: hMutSalpha, the human mismatch binding heterodimer, binds to DNA containing S6-methylthioguanine. Biochemistry 36(9):2501–2506. https://doi.org/10.1021/bi9621573
Swann PF, Waters TR, Moulton DC, Xu YZ, Zheng Q, Edwards M, Mace R (1996) Role of postreplicative DNA mismatch repair in the cytotoxic action of thioguanine. Science 273(5278):1109–1111. https://doi.org/10.1126/science.273.5278.1109
Hedeland RL, Hvidt K, Nersting J, Rosthoj S, Dalhoff K, Lausen B, Schmiegelow K (2010) DNA incorporation of 6-thioguanine nucleotides during maintenance therapy of childhood acute lymphoblastic leukaemia and non-Hodgkin lymphoma. Cancer Chemother Pharmacol 66(3):485–491. https://doi.org/10.1007/s00280-009-1184-5
Ebbesen MS, Nersting J, Jacobsen JH, Frandsen TL, Vettenranta K, Abramsson J, Wesenberg F, Schmiegelow K (2013) Incorporation of 6-thioguanine nucleotides into DNA during maintenance therapy of childhood acute lymphoblastic leukemia-the influence of thiopurine methyltransferase genotypes. J Clin Pharmacol 53(6):670–674. https://doi.org/10.1002/jcph.81
Bokkerink JP, Damen FJ, Hulscher MW, Bakker MA, De Abreu RA (1990) Biochemical evidence for synergistic combination treatment with methotrexate and 6-mercaptopurine in acute lymphoblastic leukemia. Haematol Blood Transfus 33:110–117. https://doi.org/10.1007/978-3-642-74643-7_20
Schmiegelow K (2009) Advances in individual prediction of methotrexate toxicity: a review. Br J Haematol 146(5):489–503. https://doi.org/10.1111/j.1365-2141.2009.07765.x
Frandsen TL, Heyman M, Abrahamsson J, Vettenranta K, Asberg A, Vaitkeviciene G, Pruunsild K, Toft N, Birgens H, Hallbook H, Quist-Paulsen P, Griskevicius L, Helt L, Hansen BV, Schmiegelow K (2014) Complying with the European Clinical Trials directive while surviving the administrative pressure - an alternative approach to toxicity registration in a cancer trial. Eur J Cancer 50(2):251–259. https://doi.org/10.1016/j.ejca.2013.09.027
Toft N, Birgens H, Abrahamsson J, Bernell P, Griskevicius L, Hallbook H, Heyman M, Holm MS, Hulegardh E, Klausen TW, Marquart HV, Jonsson OG, Nielsen OJ, Quist-Paulsen P, Taskinen M, Vaitkeviciene G, Vettenranta K, Asberg A, Schmiegelow K (2013) Risk group assignment differs for children and adults 1–45 yr with acute lymphoblastic leukemia treated by the NOPHO ALL-2008 protocol. Eur J Haematol 90(5):404–412. https://doi.org/10.1111/ejh.12097
Albertsen BK, Grell K, Abrahamsson J, Lund B, Vettenranta K, Jonsson OG, Frandsen TL, Wolthers BO, Heyman M, Schmiegelow K (2019) Intermittent versus continuous PEG-asparaginase to reduce asparaginase-associated toxicities: a NOPHO ALL2008 randomized study. J Clin Oncol 37(19):1638–1646. https://doi.org/10.1200/JCO.18.01877
Toksvang LN, De Pietri S, Nielsen SN, Nersting J, Albertsen BK, Wehner PS, Rosthoj S, Lahteenmaki PM, Nilsson D, Nystad TA, Grell K, Frandsen TL, Schmiegelow K (2017) Hepatic sinusoidal obstruction syndrome during maintenance therapy of childhood acute lymphoblastic leukemia is associated with continuous asparaginase therapy and mercaptopurine metabolites. Pediatric Blood Cancer 64:9. https://doi.org/10.1002/pbc.26519
Jacobsen JH, Schmiegelow K, Nersting J (2012) Liquid chromatography-tandem mass spectrometry quantification of 6-thioguanine in DNA using endogenous guanine as internal standard. J Chromatogr B Anal Technol Biomed Life Sci 881–882:115–118. https://doi.org/10.1016/j.jchromb.2011.11.032
Acknowledgements
We thank the dedicated staff at the laboratory of Pediatric Oncology, Bonkolab, Copenhagen for their valuable work. This work is part of Childhood Oncology Network Targeting Research, Organisation & Life expectancy (CONTROL) and supported by Danish Cancer Society (R-257-A14720) and the Danish Childhood Cancer Foundation (2019-5934).
Funding
Danish Cancer Society, Danish Childhood Cancer Foundation, Novo Nordisk Foundation, Swedish Childhood Cancer Foundation, Nordic Cancer Union, The Capital Region of Denmark, and Rigshospitalet, University of Copenhagen.
Author information
Authors and Affiliations
Contributions
RHL coordinated the study, compiled data, and drafted the manuscript. JN and MD performed DNA-TG analyses. KG supervised the study and performed the statistical analysis. LH and BAN supervised the study. KS initiated and supervised the study and had responsibility for the final submission for publication. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Kjeld Schmiegelow has received speaker and/or advisory board honoraria from Jazz Pharmaceuticals and Servier; speaker fee from Amgen and Medscape; Educational grant from Servier.
Ethics approval
The study was approved by the Ethical Committee of the Capital Region of Denmark (H-2.2010–002).
Informed consent
Written informed consent was obtained from all participants or legal guardians.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Larsen, R.H., Hjalgrim, L.L., Degn, M. et al. Dynamics of leucocyte DNA thioguanine nucleotide levels during maintenance therapy of childhood acute lymphoblastic leukemia. Cancer Chemother Pharmacol 88, 53–60 (2021). https://doi.org/10.1007/s00280-020-04219-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-020-04219-5