
Abstract
Purpose
To gain a better understanding of the impact of dose and other prognostic factors on safety and efficacy of docetaxel in second-line non-small-cell lung cancer patients.
Methods
A model-based meta‐analysis (MBMA) of a published docetaxel monotherapy data in 6085 second‐line non-small-cell lung cancer patients from 46 trials was conducted.
Results
The logit of grade 3/4 neutropenia incidence was a linear function of dose, with a 5 % increase in the odds of neutropenia per mg/m2 increase in dose [odds ratio (OR) 1.05, 95 % confidence interval (CI) 1.04–1.06], and a Japanese study effect (OR 17.1, 95 % CI 6.05–48.4). The logit of overall response rate (ORR) was a linear function of cumulative dose (0.4 % increase in the odds of response per mg/m2 increase; OR 1.004, 95 % CI 1.001–1.008) and median population age (OR 1.08 per year, 95 % CI 1.02–1.15). A Japanese study effect was identified for overall survival (OS) in addition to prognostic factors identified by a previous meta-analysis.
Conclusions
This current MBMA identified docetaxel dose–response relationships for both neutropenia and ORR, an effect of age on ORR, and Japanese study effects on both neutropenia and OS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lung cancer is currently the leading cause of cancer deaths worldwide. Non-small-cell lung cancer (NSCLC) accounts for the majority of lung cancer cases [1]. Though improvements in the first-line treatment of patients with advanced NSCLC have resulted in longer survival time and reduced disease-related symptoms, nearly all patients experience disease progression. Docetaxel, in addition to pemetrexed and erlotinib, is approved for use in the second-line setting [2] and is used as a comparator in second-line NSCLC studies. Meta-analysis of docetaxel in second-line NSCLC allows us to leverage these data for trial design and study result interpretation [3].
The primary mechanism of action for docetaxel involves stabilization of microtubules and ultimately disruption of cell division. The indiscriminate action of docetaxel on both proliferating cancer and normal cells, including those of the bone marrow, leads to a dose-limiting toxicity of neutropenia [4]. Cross- and within-study evaluations suggest dose- and/or exposure-related efficacy and tolerability for docetaxel. The risk of progression was found to decrease with first-course docetaxel exposure in NSCLC [5], and breast cancer patients receiving higher doses of docetaxel were reported to achieve more favorable tumor response [6]. Additional reports suggest dose may impact the mechanism of action for docetaxel; continued low-dose administration of taxanes may also result in an anti-angiogenic effect [7]. Both empirical and semi-mechanistic pharmacokinetic/pharmacodynamic (PK/PD) models suggest a decrease in neutrophil count over a range of increasing docetaxel exposure [8, 9].
Meta-analysis is a formal analytical method that can be used to integrate data from various studies to systematically assess the results of a body of research [10]. Traditional meta-analysis methods have been used to compare efficacy and safety outcomes in second-line treatment of patients with advanced NSCLC with docetaxel alone or in combination. Shen et al. [11] analyzed nine randomized controlled clinical trials (RCTs) comparing cisplatin plus vinorelbine or cisplatin plus docetaxel, showing the docetaxel combination to have improved tumor response rate, two-year survival, and safety (lower leucopenia, anemia, and vomiting) over the vinorelbine combination. Di et al. [12] analyzed six RCTs to compare efficacy and safety of pemetrexed versus docetaxel, identifying little difference in terms of efficacy, but lower rates of grade 3/4 febrile neutropenia, neutropenia, leukocytes, diarrhea, and alopecia, and higher rates of thrombocytopenia for pemetrexed. Li et al. [13] included 14 RCTs in a meta-analysis to compare the effects of combining targeted therapies with pemetrexed or docetaxel as a second-line treatment for advanced NSCLC patients. While, overall, combined therapy did not improve overall survival (OS), a subanalysis revealed a significant increase in OS in patients with non-squamous NSCLC who received combination therapy. Des Guetz et al. [14] and Qi et al. [15] both used meta-analysis of summary-level data to compare single-agent versus doublet chemotherapy. Though Qi et al. focused on docetaxel-containing therapy rather than all third-generation agents in the elderly as Des Guetz et al., both researchers concluded that doublets significantly improved overall response rate (ORR), but not OS.
Meta-analyses by Di Maio et al. [16–19] have used individual patient data (IPD) to identify prognostic factors in second-line treatment of advanced NSCLC and evaluate other aspects of therapy. A meta-analysis of individual data from 1197 patients in nine RCTs identified prognostic factors that could be used to categorize patients based on survival probability [18]. These prognostic factors included gender, performance status (PS), histology, stage, previous use of platinum, and response to first-line therapy. The prognostic score was subsequently validated using an external dataset using individual patient data from a non-inferiority phase III trial comparing vinflunine and docetaxel [19]. With the added support of the external validation of the prognostic score, this analysis could be considered a reference source for factors influencing survival in second-line treatment of advanced NSCLC.
Since individual studies suggest a relationship between docetaxel dose and both efficacy and tolerability, there is a rationale to consider a possible dose effect in addition to other potentially important covariates on endpoints of interest. While the aforementioned meta-analyses identified important trends and prognostics for docetaxel safety and efficacy, they did not explicitly consider dose or estimate a dose effect. The model-based meta-analysis (MBMA) is well-suited for this application as explicit provisions for dose are incorporated in the analysis [3]. MBMA for dose–response analysis in oncology trials has rarely been reported, potentially due to significant heterogeneity across trials. A previous study by Lu et al. [20] used MBMA to correlate paclitaxel exposure with efficacy and tolerability endpoints; this report uses similar methods to analyze summary-level data for docetaxel monotherapy in second-line NSCLC.
Materials and methods
Literature search
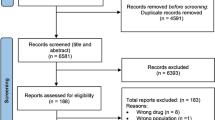
The data were extracted from a docetaxel monotherapy Clinical Trial Database developed by Quantitative Solutions Inc. The database development was done systematically, based on relevant identification, screening, and assessment steps described in the Cochrane Handbook for Systematic Reviews of Interventions [21] and reporting items in the PRISMA statement [22]; a flow diagram is provided in Supplementary Figure 1. The literature search was conducted on August 6, 2013, on the online PubMed database (http://www.ncbi.nlm.nih.gov/pubmed/), using the following search terms: docetaxel AND ((second‐line) OR (refractory) OR (relapsed) OR (salvage) OR (previously treated)) AND non‐small cell lung cancer AND (English[language]) NOT (review[publication type]). Of these, 52 were non‐duplicated clinical trials with relevant efficacy and safety information including docetaxel monotherapy treatment arms. Six studies were removed due to low quality or unmet inclusion criteria. The final database included 46 trials and 57 trial arms, with summary-level data for 6085 patients. Study, patient, and treatment information, and efficacy and safety results were extracted from each publication’s tables, figures, and text. OS curves were digitized using Engauge Digitizer, version 4.1©.
MBMA of docetaxel in NSCLC
Exploratory analysis of endpoints
Exploratory graphical analysis identified potential relationships between dose or covariates and efficacy and safety endpoints, and identified potential outliers and data errors. Efficacy endpoints included ORR and OS. Neutropenia was the safety endpoint. Each endpoint (excluding those based on Kaplan–Meier representations) was plotted against nominal and actual docetaxel dose (mg/m2), docetaxel dose intensity (mg/m2/week), and cumulative dose (mg/m2). Covariate–response relationships were examined for median age, gender, treatment cycle length, regimen length, median weeks of treatment, median weeks of follow‐up, performance status (PS), tumor stage, histology, prior treatment line (first line or second line), prior treatment type (taxane, platin, etc.), and response to first‐line treatment. Kaplan–Meier OS curves were assessed visually by different doses, regimens, or dose intensities.
Neutropenia and ORR
Neutropenia and ORR were modeled using logistic regression to describe the probability (Pr) of neutropenia (% of subjects with grade 3 or 4 neutropenia) or response (% of subjects with overall response). The impact of docetaxel exposure and covariates of interest on the probability of each endpoint was modeled using the inverse logit function:
In Eq. 1, the number of patients with an event in treatment arm j of trial i (Nevent,ij) is described by a binomial distribution that is a function of the sample size (Nij) and the probability of an event (Pr(event)ij). The probability of an event was modeled as an inverse logit of the intercept for the ith study and a linear combination of docetaxel exposure and/or covariates (f(θ ki)). The variance of the residuals was modeled as a function of the variance of the estimated probability. Random effects (inter‐trial variability) were evaluated on the intercept of any relationship with docetaxel exposure where possible. If fewer than 20 % of arms were missing a covariate value, the values in missing arms were imputed first based on the most similar study with a non-missing value or as the median across the remaining studies in the database if no similar study could be identified. For the neutropenia and ORR analyses, data were complete for the relevant covariate effects. For the OS curve analysis, some imputations were required. For the Japanese studies, any missing covariates (one instance each for Takeda [23] and Maruyama [24]) were imputed from the remaining Japanese studies.
The neutropenia and ORR models were developed by identifying a base model describing each endpoint as a function of docetaxel exposure and/or regimen, then identifying covariates that significantly improved the overall fit as assessed by Akaike Information Criterion (AIC). Metrics of docetaxel exposure included actual and nominal dose, cumulative dose, and dose intensity (in mg/m2/week). Covariates were selected based on significant (p < 0.05) univariate relationships with inter‐trial variability. Simulated dose response curves with 95 % PIs were compared to observed data. The 95 % PI of each plot was obtained by simulating 1000 trials with both inter‐ trial variability and model parameter uncertainty.
Nonlinear mixed-effects model in Splus® Professional version 8.2 (TIBCO Software Inc. Seattle, Washington) was used for model development. Exploratory plots, model evaluation, and diagnostic plots were also created using Splus®.
Overall survival
OS was modeled based on a reference survival curve extracted from a meta‐analysis of individual‐level survival data for second‐line NSCLC (“Di Maio meta‐analysis”) [18]. In the analysis of the NSCLC docetaxel database with Kaplan–Meier curves for OS, the hazard ratios reported by the Di Maio meta‐analysis established a “base model” to describe the variability due to the benchmarked prognostic factors which included sex, performance status, tumor stage, histology, platin first‐line treatment, and response to first‐line treatment. After applying the base model, the remaining covariates were explored to identify additional sources of variability in OS in the database.
Overall survival was described by the reference survival curve and the total hazard ratio (Eq. 2), where HR is a function of the prognostic factors and published hazard ratios from the Di Maio meta‐analysis, and S REF is a nonparametric reference survival curve, with one parameter estimated per time point.
The reference survival curve was evaluated by comparing the predictions from the model to the observed published survival curves from the Di Maio meta‐analysis.
Additional covariates were tested. OS for each trial (S i ) was described by Eq. 3, where HR is the hazard ratio for prognostic factors from Di Maio meta‐analysis, LRRtyp is the typical log relative risk, which represents the bias in the model, and η i is a random effect describing the remaining inter‐trial variability, cov i is an additional covariate not included in the prognostic factors, and θ describes the effect of each covariate on OS. Parameters were estimated by modeling conditional survival [Δ(t j )].
Covariates were screened for significant (p < 0.05) correlations with trial variability. Covariates included metrics of docetaxel exposure, regimen, and population characteristics excluded from the list of benchmark prognostic factors. Missing covariates were imputed from the remaining studies. For each study missing one or more values, the missing values were imputed based on studies conducted by the same researchers or at the same center where possible. When no relevant studies could be identified, the median of the remaining studies was applied. Covariates with missing values were imputed if values were missing for fewer than 20 % of study arms.
The reference curve was modeled using a nonlinear generalized least-squares model (gnls) in Splus®. The MBMA of Kaplan–Meier survival curves from the docetaxel database was completed using Splus® and NONMEM 7.2. Exploratory plots, model evaluation, and diagnostic plots were also created using Splus®.
Results
Literature database
The docetaxel database included unique phase I—III trials from 46 publications, encompassing 57 treatment arms and trial summary information for 6085 patients. Thirty of the 46 trials were randomized, though for many only a single docetaxel monotherapy arm was available. Thirty-seven arms included 4891 patients who received docetaxel once every three weeks (Q3W), 3 arms with 158 patients who received docetaxel once every 2 weeks (Q2W), and 17 arms with 1036 patients who received weekly docetaxel (QW), respectively. Nominal docetaxel doses (i.e., the first docetaxel dose) ranged from 20 to 100 mg/m2. Neutropenia, ORR, and OS data were reported for 51, 52, and 52 arms, respectively.
MBMA
Neutropenia model development
Exploratory graphical analyses evaluated potential relationships between the incidence of grade 3/4 neutropenia and docetaxel exposure metrics, regimen, and several covariates; the covariates screened included age, % males, cycle length, regimen length, treatment length, follow‐up length, performance status (PS 0, 1, or 2), tumor stage (stage III or stage IV), histology (adenocarcinoma, squamous, or other), number of prior therapies, type of prior therapy (taxane or platin), response to first‐line therapy, and study location (Japanese or non‐Japanese). Other covariates were included in the database, but were either deemed irrelevant or lacked data for more than 20 % of the treatment arms.
A base structural model was established describing the logit of neutropenia as a linear function of nominal dose. Structural models comparing cumulative dose, dose intensity, regimen alone, and dose plus regimen were also evaluated. The structural model with nominal dose alone was more predictive of neutropenia than regimen (based on Akaike Information Criterion). When the effect of regimen was included on top of dose, the regimen effect was neither significant nor well estimated.
An exploratory analysis suggested significant relationships with the proportion of male subjects, the proportion of subjects with partial response to first‐line treatment, and proportion of subjects with other response (non‐partial response or complete response) to first‐line treatment. Stepwise addition of each effect to the base model revealed that only the Japanese study effect was significant (p < 0.0001). Final model parameters are shown in Table 1; the model parameters for grade 3/4 neutropenia indicated a 5 % increase in the odds of neutropenia with each mg/m2 increase in dose [odds ratio (OR) 1.05, 95 % CI 1.04–1.06], and a Japanese study effect (OR 17.1, 95 % CI 6.05–48.4). Figure 1 suggests that the model adequately describes the data.

Observed data with neutropenia model fit. The figure shows the observed data and the 95 % prediction interval (PI) of the model including trial variability. Symbol colors vary by regimen, and line colors vary by model fit with and without Japanese study effect (red with Japanese study effect). Dashed vertical lines are 95 % PIs calculated for each observed incidence based on the normal approximation of the binomial distribution. Doses are “jittered” for visibility
ORR model development
Exploratory graphical analyses evaluated potential relationships between ORR and docetaxel exposure metrics, regimen, and covariates. The same set of screened covariates as explored for neutropenia (listed above) was again screened for ORR.
A base structural model described the logit of ORR as a linear function of actual cumulative dose, irrespective of the regimen. Relationships between trial variability and each covariate were evaluated, revealing median age as the only potential covariate. Age was added to the model, and the effect was significant (p = 0.0025), with ORR increasing with age. An interaction between the effects of cumulative dose and age was not significant. Final model parameters are shown in Table 2. The ORR model included a linear function of cumulative dose (0.4 % increase in the odds of response per mg/m2 increase in cumulative dose (OR 1.004, 95 % CI 1.001–1.008) and an effect of median population age (OR 1.08 per year, 95 % CI 1.02–1.15). Figure 2 suggests that the model adequately describes the data.

Observed data with ORR model fit as a function of cumulative dose. The figure shows the observed data and the 95 % prediction interval (PI) of the model including trial variability. Symbol colors vary by regimen. Dashed vertical lines are 95 % PIs calculated for each observed incidence based on the normal approximation of the binomial distribution. The model fit and PI are predicted at the population median age of 60 years
OS model development
Exploratory graphical analyses for OS evaluated the effect of docetaxel exposure and dosing regimen; no obvious relationships were evident. As described in detail elsewhere [25], a nonparametric reference survival curve was developed for the Di Maio analysis described previously in the Introduction [18].
Supplementary Figure 2 shows the estimated reference curve. The fit was also evaluated by using the model to predict each prognostic factor’s impact on OS as identified by the Di Maio meta‐analysis. Supplementary Figure 3 suggests that the model is a satisfactory representation of the Di Maio analysis.
The Di Maio reference model was next applied to the docetaxel NSCLC database to estimate the inter‐trial variability not explained by the benchmark prognostic factors. Although response to first‐line treatment was one of the prognostic factors in the Di Maio model, 18 of the 52 arms in the database lacked data for this factor; hence, the factor was excluded from the nonlinear mixed-effects (nlme) analysis. Table 3 shows the parameter estimates from the base and final models. To estimate inter‐trial variability, the benchmark prognostic factors were fixed at the values from the Di Maio model. In both the base and final models, the 95 % CI for the estimate of bias (θ1) includes zero, indicating no significant bias in the estimate of relative risk.
When correlations between trial variability and the remaining covariates (docetaxel exposure, Japanese study effect, treatment length, age, response to first‐line treatment, and regimen) were evaluated for the base model, only nominal dose intensity (p = 0.031) and a Japanese study effect (p = 0.0069) were significant. Figure 3 suggests that the significant relationship with nominal dose intensity was likely due to the three Japanese studies. Once the effect predicting improved OS for subjects in Japanese studies was added to the model, the relationship with dose intensity was not significant. With the inclusion of the Japanese study effect, the estimated trial variability decreased from 23.5 % in the base model to 20.7 % in the final model. Figure 4 suggests the survival curves are well described by the model.

Relationships between trial variability and dose intensity (a) or Japanese study effect (b) for overall survival (OS). The three Japanese studies are highlighted with orange symbols in (a)

A sample of survival curves by trial with trial-level (green) and population-level (red) predictions. Symbol size is proportional to square root of the number of subjects surviving at each time point
Discussion
This MBMA identified dose–response relationships for neutropenia and ORR, an age effect on ORR, and Japanese study effects on both neutropenia and OS. By integrating data from over 46 trials, with varying doses, dosing schedules, and population characteristics (e.g., age, study location), this MBMA provides a more complete picture than traditional summary-level meta-analyses by including the impact of trial-level covariate relationships on treatment effects and accounting for additional unexplained between-trials variability via random-effects models.
The analysis of grade 3/4 neutropenia suggested a significant relationship with docetaxel dose, in addition to a Japanese study effect on the baseline rate of neutropenia. Successive iterations of a semi-mechanistic myelosuppression model [9] have been applied to longitudinal neutrophil count data following docetaxel administration. A relatively recent iteration of the myelosuppression model [26] with sigmoid Emax drug effect and high Hill coefficient (~10) is well suited to capturing neutrophil count at nadir, suggesting that a combination of schedule and/or dose that minimizes time above the corresponding EC50 estimate (~1 μM) may reduce neutropenia incidence. Comparing docetaxel QW to Q3W in five RCTs inadequately powered to detect a difference, Di Maio et al. [17] identified significantly less grade 3/4 neutropenia and febrile neutropenia with QW docetaxel. Exploratory analysis of the current NSCLC database revealed a potential relationship with regimen; once dose was accounted for, no statistically significant effect of regimen was found. The Di Maio result is based on five RCTs comparing QW (33–40 mg/m2) and Q3W (66 and 75 mg/m2) regimens available at the time of analysis, and did not evaluate the effect of dose. A previous paclitaxel MBMA [20] also failed to identify regimen as a significant covariate for neutropenia in cancer patients once dose was included in the model, due to differences in dose intensity between QW and Q3W schedules. Although our docetaxel database includes a wider range of dose intensity than the paclitaxel database, and more overlap in the range of dose intensities for each schedule, the larger variability in neutropenia in Q3W trial arms is likely a greater impediment to detecting differences in neutropenia for Q3W over QW at a similar dose level. Additionally, it is of note that information on granocyte-colony-stimulating factor (GCSF) administration was not routinely reported for the studies included in our analyses; however, of the studies that did provide the information, most did not allow prophylactic use of GCSF prior to a neutropenic event. Thus, for most studies included in our analysis, GCSF administration would have little or no impact on the reported rates of neutropenia.
The Japanese study effect on neutropenia identified by the current analysis is consistent with the known higher risk of toxicity in Asian subjects leading to reduced doses in these subjects [27]. The NSCLC docetaxel database includes two studies in Taiwan [28, 29] and in China [30, 31], one study in Thailand [32], and three studies in Japan [23, 24, 33]. In addition to the expected increased toxicity risk in Asian subjects, our analysis suggests a larger increase in neutropenia in subjects in Japanese studies. The estimated odds ratio suggests a 17-fold increase in the baseline rate of neutropenia in Japanese studies. For the recommended dose of 60 mg/m2 dose of docetaxel in Japan, the expected increase in the rate of neutropenia in a Japanese study subject is about fourfold over a non-Japanese study subject. Due to insufficient data, we were unable to determine whether Japanese studies have a higher baseline rate of neutropenia, or if the increase in neutropenia for a given dose increase is larger in Japanese studies. A further consideration is that neither docetaxel exposure nor significant covariates affecting docetaxel exposure (i.e., α1-acid glycoprotein level, hepatic function, age, and body surface area as per a recent prospective population pharmacokinetic analysis [34]) were available to be included in the model; given the known relationship of hematological toxicities with docetaxel exposure, this is a possible limitation with our analysis. Also, given the limited data, inferences about the Japanese study effect at other doses or dosing frequencies may be more uncertain.
Our analysis also identified a relationship between ORR and actual cumulative dose and median population age, suggesting that ORR increases with age. In a mixed population of first-line and previously treated subjects (~42 % second line), Pallis et al. [35] found no significant difference in response rate or OS between patients of age <70 years versus patients of age ≥70 years. While our analysis evaluated the effect of a continuous age ranged from 56.5 to 74 years, the overall median age in our database was 60 years, including only one observation with median age >70 years. Only two of the Japanese studies in the database reported ORR [24, 33]; thus, no Japanese study effect was evaluated in our analysis of ORR.
For OS, our analysis was built upon a previous meta-analysis which identified prognostic factors for patients with advanced NSCLC eligible for second-line treatment [18]. Since a central component of our analysis was based on the hazard ratios estimated by Di Maio, its strength depends on the validity of their results. An external validation of the Di Maio prognostic score was completed with data from a non-inferiority phase III trial comparing vinflunine and docetaxel [19]. Application of the prognostic score allowed identification of patient subgroups with significant differences detected in survival between the prognostic categories, confirming the validity of the Di Maio prognostic model.
After applying prognostic hazard ratios from the Di Maio meta-analysis, our analysis identified a Japanese effect accounting for additional variability in OS in the docetaxel literature database. Effects of dose and regimen were not significant. The Di Maio meta-analysis included data from one Japanese study available at the time of their search [18]; hence, the effect of Japanese race was not evaluated in their study. Asian ethnicity has, however, been noted as a prognostic factor of OS in a separate model-based assessment of a single phase III study in NSCLC patients [36]; though docetaxel was not administered in this study, a model-based evaluation of first-line NSCLC patients receiving motesanib in combination with carboplatin/paclitaxel suggested Asian ethnicity, in addition to baseline tumor size, smoking history, and log (time to tumor regrowth) were significant prognostic factors of OS.
A similar model-based meta-analysis of the dose–response relationship between paclitaxel dosing regimen and ORR, OS, and neutropenia found that average dose (intensity) is predictive of ORR and OS, while neutropenia rates are predicted by administered dose [20]. Additionally, regimen effects were detected for both safety and efficacy for paclitaxel monotherapy in breast cancer patients. Since a limited number of covariates were evaluated, the authors caution that the lack of significant covariates other than dosing frequency may limit the interpretability of their results.
Most covariates included in the docetaxel database and previously identified as prognostic factors of OS [18] were consistently reported in the literature. For neutropenia and ORR, only regimen length, median weeks of follow-up, and prior treatment type were excluded from our analyses due to lack of data. For OS, the percentage of subjects responding to first-line treatment was the only prognostic factor excluded from the analysis due to missing data. A sensitivity analysis in the subset of trial arms including these data revealed no statistically significant relationship. Though additional unknown or inadequately reported covariates likely contribute to trial heterogeneity, the covariates evaluated herein are generally reflective of covariates impacting the efficacy and safety of docetaxel.
Since dose is explicitly included in the docetaxel MBMA, we can further speculate regarding any clinical benefit that might result from modified dosing in second‐line NSCLC. The finding that neutropenia and ORR trend with nominal and cumulative dose, respectively, suggests that there may be opportunities for further navigating the putative therapeutic window for docetaxel. For example, these results suggest that starting patients at a reduced nominal dose may result in enhanced tolerability with a possibly greater fraction of patients who may achieve a given cumulative dose relative to a higher nominal dose (due to dose reductions and delays for the higher dose). For example, a recent study in NSCLC suggested a low-dose regimen of docetaxel of 25 mg/m2 QW was both well-tolerated and with a response rate that was similar to the standard 75-mg/m2 Q3W regimen [37].
This analysis leverages literature data to inform drug development for second‐line NSCLC. MBMA revealed dose–response relationships for neutropenia and ORR, and identified important population characteristics that influence response for the three endpoints examined. The most immediate application of these findings would be to support a trial design, benchmark single‐arm docetaxel combination studies, and normalize results for patient prognostic factors in support of accelerated approval of new therapies. A potential future application would be to leverage the MBMA to further explore alternate dosing for docetaxel in second‐line NSCLC which is better tolerated and possibly more effective than current standards of care.
References
Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA (2008) Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc 83(5):584–594. doi:10.4065/83.5.584
Stinchcombe TE, Socinski MA (2008) Considerations for second-line therapy of non-small cell lung cancer. Oncologist 13(Suppl 1):28–36. doi:10.1634/theoncologist.13-S1-28
Mandema JW, Gibbs M, Boyd RA, Wada DR, Pfister M (2011) Model-based meta-analysis for comparative efficacy and safety: application in drug development and beyond. Clin Pharmacol Ther 90(6):766–769. doi:10.1038/clpt.2011.242
Engels FK, Verweij J (2005) Docetaxel administration schedule: from fever to tears? A review of randomised studies. Eur J Cancer (Oxford, England: 1990) 41(8):1117–1126. doi:10.1016/j.ejca.2005.02.016
Bruno R, Hille D, Riva A, Vivier N, ten Bokkel Huinnink WW, van Oosterom AT, Kaye SB, Verweij J, Fossella FV, Valero V, Rigas JR, Seidman AD, Chevallier B, Fumoleau P, Burris HA, Ravdin PM, Sheiner LB (1998) Population pharmacokinetics/pharmacodynamics of docetaxel in phase II studies in patients with cancer. J Clin Oncol 16(1):187–196
Harvey V, Mouridsen H, Semiglazov V, Jakobsen E, Voznyi E, Robinson BA, Groult V, Murawsky M, Cold S (2006) Phase III trial comparing three doses of docetaxel for second-line treatment of advanced breast cancer. J Clin Oncol 24(31):4963–4970. doi:10.1200/jco.2005.05.0294
Kerbel RS, Kamen BA (2004) The anti-angiogenic basis of metronomic chemotherapy. Nat Rev Cancer 4(6):423–436. doi:10.1038/nrc1369
Clarke SJ, Rivory LP (1999) Clinical pharmacokinetics of docetaxel. Clin Pharmacokinet 36(2):99–114. doi:10.2165/00003088-199936020-00002
Friberg LE, Henningsson A, Maas H, Nguyen L, Karlsson MO (2002) Model of chemotherapy-induced myelosuppression with parameter consistency across drugs. J Clin Oncol 20(24):4713–4721
Haidich AB (2010) Meta-analysis in medical research. Hippokratia 14(Suppl 1):29–37
Shen G, Bian G, Yu H, Gao M, Kang D, Shen G, Hu S (2014) Comparison between cisplatin plus vinorelbine and cisplatin plus docetaxel in the treatment of advanced non-small-cell lung cancer: a meta-analysis of randomized controlled trials. Mol Clin Oncol 2(1):146–150. doi:10.3892/mco.2013.210
Di BS, Wei KP, Tian JH, Xiao XJ, Li Y, Zhang XH, Yu Q, Yang KH, Ge L, Huang WH, Zhang FW (2014) Effectiveness and safety of pemetrexed versus docetaxel as a treatment for advanced non-small cell lung cancer: a systematic review and meta-analysis. Asian Pac J Cancer Prev APJCP 15(8):3419–3424
Li X, Wang H, Lin W, Xu Q (2014) Efficacy of combining targeted therapy with pemetrexed or docetaxel as second-line treatment in patients with advanced non-small-cell lung cancer: a meta-analysis of 14 randomized controlled trials. Curr Med Res Opin. doi:10.1185/03007995.2014.909392
Des Guetz G, Uzzan B, Nicolas P, Valeyre D, Sebbane G, Morere JF (2012) Comparison of the efficacy and safety of single-agent and doublet chemotherapy in advanced non-small cell lung cancer in the elderly: a meta-analysis. Crit Rev Oncol/Hematol 84(3):340–349. doi:10.1016/j.critrevonc.2012.03.007
Qi WX, Shen Z, Yao Y (2012) Meta-analysis of docetaxel-based doublet versus docetaxel alone as second-line treatment for advanced non-small-cell lung cancer. Cancer Chemother Pharmacol 69(1):99–106. doi:10.1007/s00280-011-1678-9
Di Maio M, Chiodini P, Georgoulias V, Hatzidaki D, Takeda K, Wachters FM, Gebbia V, Smit EF, Morabito A, Gallo C, Perrone F, Gridelli C (2009) Meta-analysis of single-agent chemotherapy compared with combination chemotherapy as second-line treatment of advanced non-small-cell lung cancer. J Clin Oncol 27(11):1836–1843. doi:10.1200/JCO.2008.17.5844
Di Maio M, Perrone F, Chiodini P, Gallo C, Camps C, Schuette W, Quoix E, Tsai CM, Gridelli C (2007) Individual patient data meta-analysis of docetaxel administered once every 3 weeks compared with once every week second-line treatment of advanced non-small-cell lung cancer. J Clin Oncol 25(11):1377–1382. doi:10.1200/JCO.2006.09.8251
Maio M, Lama N, Morabito A, Smit EF, Georgoulias V, Takeda K, Quoix E, Hatzidaki D, Wachters FM, Gebbia V, Tsai CM, Camps C, Schuette W, Chiodini P, Piccirillo MC, Perrone F, Gallo C, Gridelli C (2010) Clinical assessment of patients with advanced non-small-cell lung cancer eligible for second-line chemotherapy a prognostic score from individual data of nine randomised trials. Eur J Cancer (Oxford, England: 1990) 46(4):735–743. doi:10.1016/j.ejca.2009.12.013
Di Maio M, Krzakowski M, Fougeray R, Kowalski DM, Gridelli C (2012) Prognostic score for second-line chemotherapy of advanced non-small-cell lung cancer: external validation in a phase III trial comparing vinflunine with docetaxel. Lung Cancer 77(1):116–120. doi:10.1016/j.lungcan.2012.01.013
Lu D, Joshi A, Li H, Zhang N, Ren MM, Gao Y, Wada R, Jin JY (2014) Model-based meta-analysis for quantifying Paclitaxel dose response in cancer patients. CPT Pharmacomet Syst Pharmacol. doi:10.1038/psp.2014.14
Sally Green JPH, Alderson P, Clarke M, Mulrow CD, Oxman AD (2009) Cochrane Handbook for Systematic Reviews of Interventions. In: Higgins JPT, Green s (eds) The cochrane collaborations. Wiley, New York
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. doi:10.1371/journal.pmed.1000097
Takeda K, Negoro S, Tamura T, Nishiwaki Y, Kudoh S, Yokota S, Matsui K, Semba H, Nakagawa K, Takada Y, Ando M, Shibata T, Saijo N (2009) Phase III trial of docetaxel plus gemcitabine versus docetaxel in second-line treatment for non-small-cell lung cancer: results of a Japan Clinical Oncology Group trial (JCOG0104). Ann Oncol 20(5):835–841. doi:10.1093/annonc/mdn705
Maruyama R, Nishiwaki Y, Tamura T, Yamamoto N, Tsuboi M, Nakagawa K, Shinkai T, Negoro S, Imamura F, Eguchi K, Takeda K, Inoue A, Tomii K, Harada M, Masuda N, Jiang H, Itoh Y, Ichinose Y, Saijo N, Fukuoka M (2008) Phase III study, V-15-32, of gefitinib versus docetaxel in previously treated Japanese patients with non-small-cell lung cancer. J Clin Oncol 26(26):4244–4252. doi:10.1200/JCO.2007.15.0185
Wada R (2013) Technical challenges in modeling Kaplan‐Meier survival curves. In: Paper presented at the American Conference on Pharmacometrics, Ft. Lauderdale, FL, May 2013
Quartino AL, Friberg LE, Karlsson MO (2012) A simultaneous analysis of the time-course of leukocytes and neutrophils following docetaxel administration using a semi-mechanistic myelosuppression model. Invest New Drugs 30(2):833–845. doi:10.1007/s10637-010-9603-3
Perng RP, Shih JF, Chen YM, Chou KC, Lee YC, Tsai CM (2000) A phase II study of single-agent docetaxel chemotherapy for non-small cell lung cancer. Jpn J Clin Oncol 30(10):429–434
Chen JP, Lo Y, Yu CJ, Hsu C, Shih JY, Yang CH (2008) Predictors of toxicity of weekly docetaxel in chemotherapy-treated non-small cell lung cancers. Lung Cancer 60(1):92–97. doi:10.1016/j.lungcan.2007.09.004
Tsao TC, Chen CH, Chang JW, Lee CH (2006) Weekly short infusion of taxotere at a 4 week cycle in Chinese patients with advanced NSCLC who have failed or relapsed after the frontline platinum-based non-taxane chemotherapy–a Phase II trial. Jpn J Clin Oncol 36(2):80–84. doi:10.1093/jjco/hyi230
Li R, Sun L, Wang J, Qian J, Wang Z, Jiao X (2012) Pemetrexed versus docetaxel in second line non-small-cell lung cancer: results and subsets analyses of a multi-center, randomized, exploratory trial in Chinese patients. Pulm Pharmacol Ther 25(5):364–370. doi:10.1016/j.pupt.2012.06.008
Sun Y, Wu YL, Zhou CC, Zhang L, Zhang L, Liu XY, Yu SY, Jiang GL, Li K, Qin SK, Ma SL, Han L, Quinlivan M, Orlando M, Zhang XQ (2013) Second-line pemetrexed versus docetaxel in Chinese patients with locally advanced or metastatic non-small cell lung cancer: a randomized, open-label study. Lung Cancer 79(2):143–150. doi:10.1016/j.lungcan.2012.10.015
Sirisinha T, Sirilertrakul S, Jirajarus M, Ratanatharathorn V (2005) Doxetaxel in previously treated non-small cell lung cancer patients: clinical efficacy and quality of life. Southeast Asian J Trop Med Public Health 36(1):246–253
Segawa Y, Kiura K, Hotta K, Takigawa N, Tabata M, Matsuo K, Yoshioka H, Hayashi H, Kawai H, Aoe K, Maeda T, Ueoka H, Tanimoto M (2010) A randomized phase II study of a combination of docetaxel and S-1 versus docetaxel monotherapy in patients with non-small cell lung cancer previously treated with platinum-based chemotherapy: results of Okayama Lung Cancer Study Group (OLCSG) Trial 0503. J Thorac Oncol 5(9):1430–1434. doi:10.1097/JTO.0b013e3181e3248e
Kenmotsu H, Tanigawara Y (2015) Pharmacokinetics, dynamics and toxicity of docetaxel: Why the Japanese dose differs from the Western dose. Cancer Sci 106(5):497–504. doi:10.1111/cas.12647
Pallis AG, Karampeazis A, Vamvakas L, Vardakis N, Kotsakis A, Bozionelou V, Kalykaki A, Hatzidaki D, Mavroudis D, Georgoulias V (2011) Efficacy and treatment tolerance in older patients with NSCLC: a meta-analysis of five phase III randomized trials conducted by the Hellenic Oncology Research Group. Ann Oncol 22(11):2448–2455. doi:10.1093/annonc/mdq772
Claret L, Bruno R, Lu JF, Sun YN, Hsu CP (2014) Exploratory modeling and simulation to support development of motesanib in Asian patients with non-small cell lung cancer based on MONET1 study results. Clin Pharmacol Ther 95(4):446–451. doi:10.1038/clpt.2014.11
Ardizzoia A, Acquati M, Fagnani D, Giordano M, Visini M, Scanni A, Quattrone A, Fusco O, Vergani C, Casartelli C, Tagliabue P, Malugani F, Group P (2004) Second line therapy with weekly low-dose docetaxel for pretreated non-small-cell lung carcinoma patients: a multicenter Italian phase II study. Lung 182(1):1–8. doi:10.1007/s00408-003-1039-5
Acknowledgments
We wish to acknowledge Angelica Quartino, Ph.D., for helpful discussion regarding analysis of longitudinal neutrophil count data following docetaxel administration.
Author contributions
MS, MG, EC, and JJ wrote the manuscript. MS, MG, NZ, and RW analyzed the data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The study was funded by F. Hoffmann-La Roche Ltd., Basel, Switzerland, and Genentech, Inc., a member of the Roche Group, South San Francisco, CA, USA. MS, EC, and JJ are Genentech employees and own Roche stock. MG, NZ, and RW are Quantitative Solutions employees.
Electronic supplementary material
Below is the link to the electronic supplementary material.
280_2015_2957_MOESM3_ESM.pdf
Survival curves observed (from Di Maio [18]) and predicted by the Di Maio reference model. The black solid lines connect the observed points. The colored (dashed or solid) lines are predictions from the reference model (PDF 103 kb)
Rights and permissions
About this article

Cite this article
Stroh, M., Green, M., Cha, E. et al. Meta-analysis of published efficacy and safety data for docetaxel in second-line treatment of patients with advanced non-small-cell lung cancer. Cancer Chemother Pharmacol 77, 485–494 (2016). https://doi.org/10.1007/s00280-015-2957-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-015-2957-7