
Abstract
The FLAMSA reduced intensity (RIC) concept, also known as “sequential therapy”, is a conceptual platform for the treatment of leukemia separated in several parts: induction therapy, a sequence of antileukemic and immunosuppressive conditioning for allogeneic stem cell transplantation, and immune restitution supported by donor lymphocyte transfusions. The antileukemic part consists of fludarabine, cytosine arabinoside, and amsacrine (FLAMSA); non-cross reactive agents like fludarabine and amsacrine have been successfully used in cases of refractoriness and relapse. Immunosuppressive conditioning and transplantation follow after only 3 days of rest. This way, the toxicity of allogeneic transplantation could be reduced and the anti-leukemia effects by using allogeneic immune cells could be optimized. This review summarizes available data on efficacy and toxicity of this approach. Further, possible strategies for improvements are discussed in order to provide better chances for elderly and frail patients and patients with advanced and high-risk disease. Among others, several new agents are available that target molecular changes of leukemia for induction of remission and allow for bridging the time after transplantation until adoptive immunotherapy becomes safe and effective.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Originally, total body irradiation (TBI) and rescue with marrow transplantation were used for the treatment of hematopoietic malignancies including leukemia [1]. Although irradiation was effective in suppressing leukemia, it rarely could eradicate the disease. The combination of TBI with cyclophosphamide (CY) and other chemotherapy with allogeneic transplantation was effective in some patients with advanced and otherwise refractory disease. Mostly, allogeneic hematopoietic cells were essential for the cure of leukemia [2], allogeneic transplantation has always been a form of adoptive immunotherapy, but GVHD is the major obstacle of allogeneic transplantation [3]. Depletion of T cells from the graft has been the most effective way of prevention in animal experiments [4] and in human patients [5, 6]. However, rejection of the graft, delayed immune recovery, and an increased incidence of relapse have been the drawbacks of “ex vivo” T cell depletion [7]. Treatment of the recipient with anti-thymocyte globulin (ATG) and monoclonal T cell antibodies prior to transplantation could prevent rejection and GVHD by depletion of grafted T cells “in vivo” by persistent antibodies in the patient.
However, relapses were not prevented; leukemia and residual hematopoietic cells of the host survived despite “myeloablative” conditioning. Obviously, T cells were necessary for the elimination of residual lymphocytes of the host and leukemia cells [8, 9]. In animal experiments with dogs, mixed chimerism was produced by transplantation of T cell-depleted marrow [10]. In these, the transfusion of lymphocytes from the marrow donor could convert mixed into complete chimerism. Importantly, the transfusion of lymphocytes had to be delayed for 2 months after transplantation in order to prevent GVHD.
Donor lymphocyte transfusions induced sustained remissions in patients with relapse of chronic myelogenous leukemia (CML) after transplantation [11]. Beneficial effects were also observed in patients with recurrent acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), myeloproliferative neoplasms (MPN), and multiple myeloma (MMY) as well as in some patients with acute lymphoblastic leukemia (ALL) [12,13,14]. The beneficial effect of donor lymphocytes gave a chance for reducing the intensity of conditioning, but the role of donor lymphocytes and conditioning remains to be defined for various diseases and stages of disease. Non-myeloablative conditioning and conditioning with reduced intensity have already allowed the inclusion of elderly and frail patients [15, 16].
The aim of the FLAMSA-RIC regimen in patients with advanced or genetically high-risk acute myeloid leukemia (AML) and preleukemic myelodysplastic syndrome (MDS) was the sequential application of a short and intensive chemotherapy followed by reduced intensity conditioning without waiting for a remission to be confirmed. Conditioning treatment with FLAMSA-RIC has primarily been restricted to elderly patients (over 60 years of age) and patients with high-risk AML. Most patients had intensive induction chemotherapy with and without remission and incomplete recovery of blood counts. As a rule, patients with high-risk MDS did not have prior intensive chemotherapy, but they were treated with azacytidine, decitabine, or low-dose cytosine arabinoside (ARA-C). The majority had refractory or relapsed disease [17].
Antileukemic conditioning
The FLAMSA-RIC concept was designed for patients with advanced acute myeloid leukemia (AML) and preleukemic myelodysplastic syndrome (MDS); the disease stage was either primary refractory, in relapse or with high risk of early relapse. The first part of the treatment consists of intermediate doses of cytosine arabinoside (Ara-C 2 g/m2) preceded by fludarabine (30 mg/kg) and followed by amsacrine (100 mg/m2) on each of 4 successive days followed by 3 days of rest prior to the second part of treatment with 4 Gy TBI on day − 4, antithymocyte globuline (ATG) on days − 3, − 2, and − 1 and cyclophosphamide (CY) on days − 3 and − 2 prior to transplantation [17]. The first part is directed to proliferating leukemia cells, whereas TBI is toxic to stem cells and kills quiescent and slowly proliferating leukemia stem cells besides normal stem cells (cf. below). This protocol is highly effective and well tolerated. The addition of fludarabine (FLU) prior to Ara-C enhances the production of Ara-CTP [18]. Amsacrine was applied instead of anthracyclines, because it belongs to another class of DNA intercalating drugs and inhibitors of topoisomerase II, it is not cross resistant with anthracyclines [19] and less cardiotoxic [20]. In countries where amsacrin is not available, mitoxantrone (10 mg/m2 × 3 days) and idarubicin (10 mg/m2 × 3 days) have been used with some success. FLAMSA has also been used in patients with recurrent AML after allogeneic transplantation for remission induction followed by blood stem cells from the original donor. These patients did not receive immunosuppressive conditioning, if significant chimerism persisted. The leukemia treatment block has been changed by some centers and clofarabine has been substituted for fludarabine. Clofarabine is very effective in acute leukemia, but is associated with considerable toxicity. The dose of ARA-C should be reduced, if clofarabine is substituted for fludarabine (M. Mohty personal comm.) [21].
Immunosuppressive conditioning
This part of the conditioning was reduced intensity consisting of 4 Gy TBI, ATG and CY. TBI has a strong myelosuppressive effect; its immunosuppressive effect is moderate. Cyclophosphamide (CY) is strongly immunosuppressive, but it fails to eliminate myeloid stem cells. The combination of TBI with cyclophosphamide is sufficiently immunosuppressive and allows prompt engraftment and permanent chimerism [22]. Prevention of GVHD is best achieved by depletion of T cells from the graft. Treatment of the patient with ATG is superior to ex vivo T cell depletion because the immune suppression of the host prevents rejection; ex vivo treatment of the graft only prevents GVHD. ATG given to the host prior to transplantation suppresses the host’s immune reaction against the graft and the graft-versus-host reaction by “in vivo” T cell depletion. In patients given sufficiently large doses of ATG (30 mg/kg × 4 days), T cell antibodies were found in the peripheral blood up to 4 weeks after the last dose [23]. Antibody levels fell suddenly around 30 days post treatment, most likely because antibodies against ATG are formed that eliminate residual activity. CY and ATG doses were adjusted to the donor source, HLA-identical sibling transplant: ATG 10 mg/kg × 3 days, CY 40 mg/kg × 2 days, HLA-matched unrelated transplants: ATG 20 mg/kg × 3 days, CY 60 mg/kg for 2 days.
CY exerts strong immunosuppression, but mucositis and cystitis are serious side effects, particularly in elderly patients. Possibly, CY could be reduced without a critical reduction of immune suppression [24]. In a previous study in patients with CML, reduction of the dose of TBI did not change day 100 non-relapse mortality, whereas the reduced CY dose decreased early mortality significantly [25].
In principle, TBI was applied as part of the immunosuppression, but it also induces prolonged hematopoietic aplasia. It has strong effects on stem cells, normal hematopoietic and leukemia stem cells [26], 99% of progenitor cells are eliminated at 4 Gy. In general, leukemia stem cells have a similar radiosensitivity as normal stem cells. However, the radio-sensitivity of leukemia may vary with the stage of the leukemia; in advanced stages, a greater resistance of apoptotic mechanisms can develop. The results of transplantation are best for patients transplanted in remission; the results are worst, if several lines of chemotherapy have failed. In primary refractory patients, the results are better, if they had less chemotherapy before transplantation [17, 27]. Allogeneic transplantation in refractory patients should therefore be scheduled as soon as one or two cycles of induction chemotherapy have failed.
The effect of TBI can be enhanced by prior chemotherapy with fludarabine and amsacrine, but it is not known whether the effect of other stem cell toxic agents as busulfan, treosulfan, melphalan, and BCNU are also enhanced. Substituting TBI with busulfan for 2 days has been well tolerated by elderly patients, but its anti-leukemia effect may be lower [28]. Treosulfan at a dose of 10 g/m2 was substituted for TBI with a similar outcome in elderly patients [29].
A prospective randomized study in Great Britain did not find better results with FLAMSA-busulfan than with other regimens including fludarabine-busulfan [30]. However, 155 patients were in remission and only nine patients in primary refractory disease, and treatment for remission induction and time until transplantation were not reported. In contrast, a retrospective analysis of the EBMT Acute Leukemia Working Party showed a lower relapse incidence and better relapse-free survival of FLAMSA TBI than treosulfan-fludarabine and FLAMSA Busulfan, but no major impact on overall survival [31]. A benefit of low dose of TBI was also described in patients with MDS conditioned with fludarabine and treosulfan [32]; the relapse incidence was lower with an additional dose of 2 Gy TBI without increased toxicity.
Adoptive immunotherapy with transfusions of lymphocytes of the donor
Transfusion of donor lymphocytes is an integral part of the FLAMSA-RIC concept and of allogeneic stem cell transplantation with any form of T cell depletion for prevention of GVHD. An important variable is the time after transplantation in order to avoid GVHD. In animal experiments, it had been shown that 2 months after transplantation of T cell-depleted marrow lymphocytes of the donor could be transfused without producing GVHD [8, 33]. These animals were mixed chimeras and became complete chimeras after donor lymphocyte transfusions. Immune responses were improved in transfused animals and donor immunity could be transferred. These animals could be given large amounts of lymphocytes without producing GVHD. However, GVHD did occur in animals that received donor lymphocytes following a T cell-depleting treatment [34].
In humans, donor lymphocyte transfusions were effective in the treatment of relapses of CML, AML, and myeloma as well as in some patients with ALL [11,12,13,14]. However, sustained remissions were observed mainly in patients with recurrent CML; the majority of patients with acute leukemia and myeloma disease relapsed again without further treatment. Long-term remissions were preferably seen in CML patients treated simultaneously with low-dose interferon-a (IFN-a) or IFN-a and GM-CSF [35]. Success was also due to the slow pace of the disease in CML, and GVHD could be avoided by starting with a low dose and escalating doses with repeated transfusions [36, 37]. In AML, relapse could be controlled with low-dose Ara-C, mobilized stem cells, and GM-CSF after transfusion, if the relapse occurred more than 6 months after transplantation [38]. GVHD was more frequent than in CML patients.
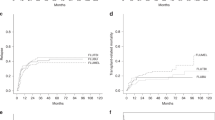
Prophylactic donor lymphocyte transfusions (DLI) were given to high-risk AML patients more than 120 days after transplantation. The requirements for prophylactic DLI were absence of GVHD, infections, and relapse; immunosuppressive therapy had to be suspended for at least 30 days [17]. A matched pair analysis of FLAMSA patients treated in Germany demonstrated superior survival of patients given DLI as compared to those not given DLI (Fig. 1) [39]. However, the control of early relapses is difficult by DLI from normal donors; they have been excluded by a landmark analysis in 180-day survivors. This analysis compared patients transplanted in remission and patients transplanted in active disease with their respective historical control. Remission patients had an excellent survival and relapse patients an improved survival as compared to historical controls. Of course, retrospective analyses can be biased by the improvement of treatment modalities not adjusted for.

FLAMSA regimen and its components. Flu: fludarabin 30 mg/m2, AraC: cytosine arabinoside 2000 mg/m2, AMSA: amsacrine 100 mg/m2; BUS2: busulfan 4 × 0.8 mg/kg × 4 per day × 2 days; TBI: total body irradiation 4 Gy; ATG: antithymocyte globulin 20 mg/kg or 10 mg/kg (in case of HLA-identical sibling donor) per day × 3; CY: cyclophosphamide 60 mg/kg (40 mg/kg for HLA-identical sibling donor); HCT hematopoietic cell transplantation, DLI: donor lymphocyte transfusions in escalating doses starting with 1 × 106/kg CD3+ T cells escalating to 5 × 106 and 107/kg or 108/kg
Acute GVHD was seen in about 50% of patients given large doses of DLI; in most patients, severe GVHD could be prevented by starting with a low dose of donor T cells (1 × 106–1 × 107/kg body weight (BW) for HLA-identical transplants) and increasing the dose every 4–6 weeks, if there is no GVHD. In HLA-mismatched and HLA-haploidentical transplants, the starting dose should be no more than 1 × 105/kg BW. This dose of T cells in the graft did not produce acute GVHD neither in DLA-mismatched dogs [40] nor in HLA-mismatched human patients [41] . However, GVHD can develop, if lymphocyte-depleting treatment is given prior to DLI and/or infection is occurring. Infections, particularly viral infection, induce interferon and expression HLA class II antigens in non-hematopoietic tissue. Prevention of infection by prevention of exposure and prophylactic treatment with antibiotics, antivirals, and antifungals is indicated. As a rule, acute GVHD can be controlled, if treated early and with adequate intensity [42].
Chronic GVHD can develop in some patients; a mild degree may be acceptable, because it is associated with a strong graft-versus-leukemia effect. More severe chronic GVHD is deleterious and should be treated with all available methods. Progressive involvement of the lungs and the gut has to be treated vigorously.
The sequential treatment with DLI in the FLAMSA-RIC study has been designed for the prophylaxis of leukemia relapse in patients with high-risk AML and MDS after T cell depletion at transplantation; the use of DLI in patients with minimal residual disease after transplantation is discussed.
Current problems and future directions
Prophylactic and preemptive treatment with donor lymphocytes
Prophylactic treatment is indicated in patients with active disease and high-risk leukemia. Particular high risks are associated with primary refractory leukemia, early relapses of leukemia, and remissions without recovery of blood counts (CRi). Alternatively, post-transplant treatment with DLI may be preemptive in patients with minimal residual disease after transplantation. These patients have a particular high risk of relapse [43]. Cells with a mutated genotype for NPM1, CBFB-MYH11 (inv 16), and RUNX/RUNX1 can be detected by PCR with a sensitivity of 10−5 malignant cells [43]. An even better sensitivity can be reached by next-generation sequencing (NGS) [44]. Patients with MRD were treated with DLI or IL-2 depending on the availability of the DLI donor; DLI reduced relapse and improved survival in a multicenter study [45, 46]. These studies differ from others in several ways: the transplant consisted of G-CSF-mobilized bone marrow and blood cells, DLI were G-CSF-mobilized PBSC preceded in most cases by a cycle of intensive chemotherapy, GVHD prophylaxis was given after DLI for 2–4 weeks, and IL-2 was administered for stimulation of DLI. Most importantly, DLI were started whenever MRD was positive, as early as day 30 or 60 after transplantation.
The delay of DLI to day 120 after transplantation reflects the preconditions of absence of immunosuppressive treatment, absence of GVHD, and infections as well as the exclusion of early relapses. In addition, the effect of DLI from normal non-immunized donors on residual host hematopoietic cells is an ongoing effect over several months [8], in patients with CML clinical response took often 6–8 weeks after DLI and the median time until molecular response was 6 months and later responses were seen after more than 1 year [35, 47]. Therefore, it is conceivable that DLI from normal donors may not show immediate effects unless the donor is immune to an antigen presented by the leukemia or DLI are activated by host dendritic cells after transfusion.
Stimulation of the response
Most experience in stimulating a response has been gained from treating relapses after transplantation. In CML dendritic cells of leukemia origin present antigen directly [48], presentation can be stimulated by treatment with low-dose interferon-alpha (IFN-a) and GM-CSF [49]. In AML, direct antigen presentation and stimulation of T cells can be induced with GM-CSF [50, 51]; the role of IFN-a is disputed [52]. Clinical trials have shown divergent results; better results are expected from pegylated IFN-a. [52]. Patients with relapse of AML were treated with low-dose Ara-C, G-CSF-mobilized blood cells, and GM-CSF. Treatment of the patients with GM-CSF that started at week 2 and continued every month for 1 week has enabled leukemia-free survival in some patients. Patients with a late relapse had a better prognosis and some patients survived with sustained long-term remissions. Long-term survival of some patients has also been reported with the combination of azacytidine and DLI [53]. Early relapses are often associated with a FLT3-ITD. They rarely responded low-dose Ara-C; they could be treated with sorafenib or the first part of the FLAMSA regimen; in these, mobilized peripheral blood stem cell DLI and GM-CSF carried a high risk of acute GVHD.
There are several ways of immune escape of AML cells as summarized in recent reviews [54, 55]. Increased anti-inflammatory cytokines as IL-10 and TGF-ß, decreased inflammatory cytokines, and immunosuppressive enzymes as IDO and others are well known. Immune check point ligands and genes of the proliferative machinery (FLT3-ITD, KRAS) have gained interest with new inhibitory agents. In HLA-haploidentical transplantation, the genetic loss of heterozygosity of HLA class I in AML cells was an important finding [56]. Recently, variables for immune escape of AML cells were investigated in patients with relapse after allogeneic transplantation as compared to those after chemotherapy [57, 58]; the spectrum of gained and lost mutations at relapse as compared to those at diagnosis was similar in both groups [57]. Firstly, HLA class II antigens were downregulated in the majority of patients, a change that can be reversed with IFN-gamma.
Check point inhibitors have a great success in the treatment of lymphoma [59] and some solid tumors; they have been used for the treatment of leukemia relapse after allogeneic stem cell transplantation [60, 61]. The risk of GVHD has to be considered, and results are controversial. In patients with residual disease prior chemotherapy may be justified; this results in the depletion of lymphocytes prior to DLI [45] and damage associated activation giving a high risk of GVHD. These patients should be treated with prophylactic immune suppression for a short time [62]. However, immune suppression is a hindrance to recognize antigens on leukemia cells and it may result in the failure of GVL effects.
Bridging between transplantation and DLI
Obviously, donor lymphocytes transfused after more than 120 days cannot prevent early relapses, the time for recognition, and immune reaction may need another month so that 180 days as a landmark is a relevant time point for the evaluation of the effects. Therefore, bridging of the time until DLI is an important task.
Azacytidine has been given as post-transplant maintenance [63, 64] in combination with DLI in patients with recurrent AML/MDS [53, 65]. Complete responses were seen, and some responses were durable [63]. In combination with valproate, azacytidine can induce CD8-positive T cells against the tumor antigen MAGE [64]. Azacytidine was effective for the treatment of relapse after transplantation in a multicenter study and DLI did not improve the results of azacytidine [66]. However, there was no common schedule of DLI and most received DLI after failure of azacytidine. Favorable factors for response were late relapse—after more than 6 months—and low blast count in the marrow (< 20%) [66]. A multicenter study of azacytidine for mixed chimerism (RELAZA trial) demonstrated improved survival [63]. Recently, an oral preparation of azacytidine was tested as maintenance drug with good results, best results with 14 days of treatment rather than the usual 7-day schedule [67]. Another hypomethylation drug is decitabine that has been used in combination with DLI for the treatment of relapses after transplantation [68]. Long-term survival was achieved by second transplants.
In patients with FLT3 ITD, sorafenib was successful for remission induction pre- and post-transplant [69]; patients achieving molecular remissions have a chance of long-term survival [70]. Maintenance treatment with sorafenib post-transplant has improved relapse-free survival without significant added toxicity [71]. Midostaurin given with chemotherapy and after transplantation did have a positive effect [72]; more specific FLT3 inhibitors are quizartinib and gilteritinib [73]. Presently, it is not known whether these have the same immune effects as sorafenib [74].
Another interesting drug is the histone deacetylase inhibitor panobinostat as maintenance treatment [75] that was tested in 42 patients starting between 60 and 147 with a median of 95 days. There was no increase of GVHD, not even after DLI; panobinostat does not prevent the development of immunological tolerance; it has an immune-modulating effect as vorinostat, another deacetylase inhibitor [76], without weakening the graft-versus-leukemia effect. The major problem of these targeted therapies is hematological side effects so that treatment can only be started late after 1–2 months. Similarly, the bcl2 inhibitor venetoclax has excellent activity against leukemia, but the hematological side effects prohibit prophylactic treatment for bridging.
Similarly, the CD33 antibody treatment either charged with the drug ozogamycin or as bispecific CD33 × CD3 T cell engager (BITE) has a limited role as bridging because of myelosuppression. The cytostatic-loaded antibody had severe side effects with veno-occlusive disease of the liver; it has been reintroduced for high antileukemic efficiency at a lower dose.
Remission induction
A major problem of the treatment of AML and preleukemic MDS is the high age and physical condition of the patients; many patients are not fit enough to stand several cycles of intensive chemotherapy without complications. Most regimens for remission induction are intensive chemotherapy with Ara-C and Daunomycin (7 + 3) [77] or FLAG-Ida [78]. They are associated with severe side effects like infections, diarrhea, and cardiac problems. Less intensive regimens can de designed for elderly and frail patients. Low-dose ARA-C was conventionally given with 20 mg/m2 twice per day for 10 days; toxicity was low as were remission rates [79]. Conventional regimens of low-dose ARA-C are not very effective, but treatment of elderly patients with 10 mg/m2 twice per day for 21 days produced the same survival as intensive chemotherapy with less side effects [80]. Gastrointestinal toxicity can limit the duration of treatment; otherwise, treatment over 4 weeks may even improve responses in patients with preleukemic MDS or smoldering leukemia and slow progression (personal obs.). Recently, combinations of low-dose ARA-C with cladribine in alternating cycles with decitabine have achieved objective responses in 58% of patients and a median overall survival of 13.8 months [81]. New regimens of low toxicity and good efficacy have been described; they include CPX351 and combinations of venetoclax with either Ara-C or azacytidine. CPX351 is a liposomal preparation of a fixed combination of Ara-C and daunorubicin that permits the slow release of the drugs with low toxicity and high efficiency [82]. CPX351 was compared to the conventional 7 + 3 regimen; it showed improved survival and gave the chance of long-term remissions following allogeneic transplantation [83]. Venetoclax is a bcl2 inhibitor that combines very well with low-dose Ara-C or azacytidine [84]. These less toxic induction therapies increase the chances of elderly and frail patients for transplantation. Sequential conditioning with FLAMSA may be sufficient to induce long-term remissions in patients treated with low intensity induction therapy.
Conclusions
The FLAMSA-RIC concept is a time sequential therapy that includes sequential anti-leukemia therapy with reduced intensity conditioning including in vivo T cell depletion and delayed transfusion of donor lymphocytes. The anti-leukemia part of conditioning is highly effective; the conditioning part consists of myelosuppressive 4 Gy TBI, BUS, or Treosulfan, and immunosuppressive ATG/CY. In countries where amsacrine is not available, idarubicin or mitoxantrone has been used instead. TBI appears superior anti-leukemic, BUS, and Treo less toxic in elderly patients. The use of melphalan and thiotepa has not yet been reported in this context. Toxicity of CY may be decreased by lower doses or protracted application (3 × 20/40 mg/kg). Immune therapy with donor lymphocytes is effective in patients treated with T cell depletion in vivo or ex vivo. ATG or alemtuzumab should be given in doses sufficient for in vivo T cell depletion. Donor lymphocytes rarely produce a GVL effect before 4–8 weeks unless the patient is lympho-depleted by prior therapy, or lymphocytes are stimulated by IFN-a and /or GM-CSF, intermittent infections or lymphocytes are from immune donors. The indication of DLI may be restricted to patients with minimal residual disease (MRD) or given to every patient with high-risk MDS/AML. Bridging the time interval between transplantation and DLI is most important, azacytidine and lenalidomide or panobinostat have been used with success, sorafenib for FLT3 mutated AML. The indication of allogeneic transplantation has been expanded to patients of 70 years and older. In patients, primary induction should be limited to one or two cycles of chemotherapy; in elderly patients, new less intensive regimens should be preferred like venetoclax-azacytidine [85] or CPX 351 [86].
References
Thomas ED, Lochte HL Jr, Cannon JH, Sahler OD, Ferrebee JW (1959) Supralethal whole body irradiation and isologous marrow transplantation in man. J Clin Invest 38:1709–1716
Mathe G, Amiel JL, Schwarzenberg L, Cattan A, Schneider M (1965) Adoptive immunotherapy of acute leukemia: experimental and clinical results. Cancer Res 25(9):1525–1531
Thomas E, Storb R, Clift RA, Fefer A, Johnson FL, Neiman PE et al (1975) Bone-marrow transplantation (first of two parts). N Engl J Med 292(16):832–843
Kolb HJ, Rieder I, Rodt H, Netzel B, Grosse Wilde H, Scholz S et al (1979) Antilymphocytic antibodies and marrow transplantation. VI. Graft- versus-host tolerance in DLA-incompatible dogs after in vitro treatment of bone marrow with absorbed antithymocyte globulin. Transplantation 27:242–245
Rodt H, Kolb HJ, Netzel B, Rieder I, Janka G, Belohradsky B et al (1979) GVHD suppression by incubation of bone marrow grafts with anti-T- cell globulin: effect in the canine model and application to clinical bone marrow transplantation. TransplantProc. 11:962–966
Waldmann H, Polliak A, Hale G, Or R, Cividalli G, Weiss L et al (1984) Elimination of graft-versus-host disease by in-vitro depletion of alloreactive lymphocytes with a monoclonal rat anti-human lymphocyte antibody (Campath 1). Lancet II:483–486
Goldman JM, Gale RP, Horowitz MM, Biggs JC, Champlin RE, Gluckman E et al (1988) Bone marrow transplantation for chronic myelogenous leukemia in chronic phase: increased risk of relapse associated with T-cell depletion. AnnInternMed. 108:806–814
Kolb HJ, Gunther W, Schumm M, Holler E, Wilmanns W, Thierfelder S (1997) Adoptive immunotherapy in canine chimeras. Transplantation. 63(3):430–436
Apperley JF, Jones L, Hale G, Waldmann H, Hows J, Rombos Y, Tsatalas C, Marcus RE, Goolden AW, Gordon-Smith EC (1986) Bone marrow transplantation for patients with chronic myeloid leukaemia: T-cell depletion with Campath-1 reduces the incidence of graft-versus-host disease but may increase the risk of leukaemic relapse. Bone Marrow Transplant 1(1):53–66
Kolb HJ, Beisser K, Mittermueller J, Clemm C, Schumm M, Ledderose G et al (1992) Adoptive immunotherapy in human and canine chimeras. In: Hiddemann W, Büchner T, Plunkett W, Keating M, Wörmann B, Andreeff M (eds) Acute Leukemias - Pharmakokinetics. Springer, Berlin, pp 595–600
Kolb HJ, Mittermuller J, Clemm C, Holler E, Ledderose G, Brehm G, Heim M, Wilmanns W (1990) Donor leukocyte transfusions for treatment of recurrent chronic myelogenous leukemia in marrow transplant patients. Blood. 76(12):2462–2465
Kolb HJ, Schattenberg A, Goldman JM, Hertenstein B, Jacobsen N, Arcese W, Ljungman P, Ferrant A, Verdonck L, Niederwieser D, van Rhee F, Mittermueller J, de Witte T, Holler E, Ansari H, European Group for Blood and Marrow Transplantation Working Party Chronic Leukemia (1995) Graft-versus-leukemia effect of donor lymphocyte transfusions in marrow grafted patients 397. Blood. 86(5):2041–2050
Collins RH, Shpilberg O, Drobyski WR, Porter DL, Giralt S, Champlin R et al (1997) Donor leukocyte infusions in 140 patients with relapsed malignancy after allogeneic bone marrow transplantation. J Clin Oncol 15:433–444
Shiobara S, Nakao S, Ueda M, Yamazaki H, Takahashi S, Asano S, Yabe H, Kato S, Imoto S, Maruta A, Yoshida T, Gondo H, Morishima Y, Kodera Y (2000) Donor leukocyte infusion for Japanese patients with relapsed leukemia after allogeneic bone marrow transplantation: lower incidence of acute graft-versus-host disease and improved outcome. Bone Marrow Transplant 26(7):769–774
McSweeney PA, Niederwieser D, Shizuru JA, Sandmaier BM, Molina AJ, Maloney DG et al (2001) Hematopoietic cell transplantation in older patients with hematologic malignancies: replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood. 97(11):3390–3400
Giralt S, Khouri I, Champlin R (1999) Non myeloablative "mini transplants". Cancer Treat Res 101:97–108
Schmid C, Schleuning M, Ledderose G, Tischer J, Kolb HJ (2005) Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J Clin Oncol 23(24):5675–5687
Gandhi V, Estey E, Keating MJ, Plunkett W (1993) Fludarabine potentiates metabolism of cytarabine in patients with acute myelogenous leukemia during therapy. J Clin Oncol 11(1):116–124
Legha SS, Keating MJ, Zander AR, McCredie KB, Bodey GP, Freireich EJ (1980) 4′-(9-Acridinylamino) methanesulfon-m-anisidide (AMSA): a new drug effective in the treatment of adult acute leukemia. Ann Intern Med 93(1):17–21
Arlin ZA, Feldman EJ, Mittelman A, Ahmed T, Puccio C, Chun HG, Cook P, Baskind P, Marboe C, Mehta R (1991) Amsacrine is safe and effective therapy for patients with myocardial dysfunction and acute leukemia. Cancer. 68(6):1198–1200
Mohty M, Malard F, Blaise D, Milpied N, Socie G, Huynh A et al (2017) Sequential regimen of clofarabine, cytosine arabinoside and reduced-intensity conditioned transplantation for primary refractory acute myeloid leukemia. Haematologica. 102(1):184–191
Santos GW, Tutschka P, Brookmeyer R et al (1983) Marrow transplantation for acute non-lymphocytic leukemia after treatment with busulfan and cyclophosphamide. N Engl J Med 309:1347–1353
Kolb HJ, Guenther W, Gyurkocza B, Hoetzl F, Simoes B, Falk C, Schleuning M, Ledderose G (2003) Tolerance and chimerism. Transplantation. 75(9 Suppl):26S–31S
Anderlini P, Wu J, Gersten I, Ewell M, Tolar J, Antin JH, Adams R, Arai S, Eames G, Horwitz ME, McCarty J, Nakamura R, Pulsipher MA, Rowley S, Leifer E, Carter SL, DiFronzo NL, Horowitz MM, Confer D, Deeg HJ, Eapen M (2015) Cyclophosphamide conditioning in patients with severe aplastic anaemia given unrelated marrow transplantation: a phase 1-2 dose de-escalation study. Lancet Haematol 2(9):e367–e375
Weisser M, Schleuning M, Ledderose G, Rolf B, Schnittger S, Schoch C, Schwerdtfeger R, Kolb HJ (2004) Reduced-intensity conditioning using TBI (8 Gy), fludarabine, cyclophosphamide and ATG in elderly CML patients provides excellent results especially when performed in the early course of the disease. Bone Marrow Transplant 34(12):1083–1088
Kimler BF, Park CH, Yakar D, Mies RM (1985) Radiation response of human normal and leukemic hemopoietic cells assayed by in vitro colony formation. Int J Radiat Oncol Biol Phys 11(4):809–816
Pfeiffer T, Schleuning M, Mayer J, Haude KH, Tischer J, Buchholz S, Bunjes D, Bug G, Holler E, Meyer RG, Greinix H, Scheid C, Christopeit M, Schnittger S, Braess J, Schlimok G, Spiekermann K, Ganser A, Kolb HJ, Schmid C (2013) Influence of molecular subgroups on outcome of acute myeloid leukemia with normal karyotype in 141 patients undergoing salvage allogeneic stem cell transplantation in primary induction failure or beyond first relapse. Haematologica. 98(4):518–525
Heinicke T, Labopin M, Schmid C, Polge E, Socie G, Blaise D et al (2018) Reduced relapse incidence with FLAMSA-RIC compared with busulfan/fludarabine for acute myelogenous leukemia patients in first or second complete remission: a study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant 24(11):2224–2232
Holtick U, Herling M, Pflug N, Chakupurakal G, Leitzke S, Wolf D, Hallek M, Scheid C, Chemnitz JM (2017) Similar outcome after allogeneic stem cell transplantation with a modified FLAMSA conditioning protocol substituting 4 Gy TBI with treosulfan in an elderly population with high-risk AML. Ann Hematol 96(3):479–487
Craddock C, Jackson AE, Malladi RK, Gilleece MH, Peniket A, Salim R, Tholouli E, Potter V, Crawley CR, Protheroe RE, Anne Parker A, Wilson K, Pavlu J, Nagra Siddique S, Hodgkinson A, Mason J, Wheatley K, Russell NH, Freeman SD (2019) The sequential FLAMSA-Bu conditioning regimen does not improve outcome in patients allografted for high risk acute myeloid and myelodysplasia irrespective of pre-transplant MRD status: results of the UK NCRI Figaro Trial. Blood. 134(Suppl 1)
Sheth V, Labopin M, Canaani J, Volin L, Brecht A, Ganser A, et al. (2018) Comparison of FLAMSA-based reduced intensity conditioning with treosulfan/fludarabine conditioning for patients with acute myeloid leukemia: an ALWP/EBMT analysis. Bone Marrow Transplant
Deeg HJ, Stevens EA, Salit RB, Ermoian RP, Fang M, Gyurkocza B, Sorror ML, Fatobene G, Baumgart J, Burroughs LM, Delaney C, Doney K, Egan DN, Flowers MED, Milano F, Radich JP, Scott BL, Sickle EJ, Wood BL, Yeung C, Storer BE (2018) Transplant conditioning with treosulfan/fludarabine with or without total body irradiation: a randomized phase II trial in patients with myelodysplastic syndrome and acute myeloid leukemia. Biol Blood Marrow Transplant 24(5):956–963
Drobyski WR, Keever CA, Roth MS, Koethe S, Hanson G, McFadden P, Gottschall JL, Ash RC, van Tuinen P, Horowitz MM (1993) Salvage immunotherapy using donor leukocyte infusions as treatment for relpased chronic myelogenous leukemia after bone marrow transplantation: efficacy and toxicity of a defined T-cell dose. Blood. 82:2310–2318
Johnson BD, Becker EE, LaBelle JL, Truitt RL (1999) Role of immunoregulatory donor T cells in suppression of graft-versus-host disease following donor leukocyte infusion therapy. JImmunol. 163(12):6479–6487
Kolb HJ, Rank A, Chen X (2004) In-vivo generation of leukaemia-derived dendritic cells. . p. 439–51
Mackinnon S, Papadopoulos EB, Carabasi MH, Reich L, Collins NH, Boulad F, Castro-Malaspina H, Childs BH, Gillio AP, Kernan NA (1995) Adoptive immunotherapy evaluating escalating doses of donor leukocytes for relapse of chronic myeloid leukemia after bone marrow transplantation: separation of graft-versus-leukemia responses from graft-versus-host disease. Blood. 86:1261–1268
Dazzi F, Szydlo RM, Craddock C, Cross NC, Kaeda J, Chase A et al (2000) Comparison of single-dose and escalating-dose regimens of donor lymphocyte infusion for relapse after allografting for chronic myeloid leukemia. Blood. 95(1):67–71
Schmid C, Schleuning M, Aschan J, Ringden O, Hahn J, Holler E et al (2004) Low-dose ARAC, donor cells, and GM-CSF for treatment of recurrent acute myeloid leukemia after allogeneic stem cell transplantation. Leukemia. 18(8):1430–1433
Jedlickova Z, Schmid C, Koenecke C, Hertenstein B, Baurmann H, Schwerdtfeger R, Tischer J, Kolb HJ, Schleuning M (2016) Long-term results of adjuvant donor lymphocyte transfusion in AML after allogeneic stem cell transplantation. Bone Marrow Transplant 51(5):663–667
Schumm M, Günther W, Kolb HJ, Rieber P, Büttner M, Voss C et al (1994) Prevention of graft-versus-host disease in DLA-haplotype mismatched dogs and hemopoietic engraftment of CD6-depleted marrow with and without cG-CSF treatment after transplantation. Tissue Antigens 43:170–178
Kernan NA, Collins NJ, Juliano L, Cartagena T, Dupont B, Oreilly RJ (1986) Clonable T-lymphocytes in T-depleted bone marrow transplants correlate with development of graft-versus-host disease. Blood 68:770
Marks DI, Lush R, Cavenagh J, Milligan DW, Schey S, Parker A, Clark FJ, Hunt L, Yin J, Fuller S, Vandenberghe E, Marsh J, Littlewood T, Smith GM, Culligan D, Hunter A, Chopra R, Davies A, Towlson K, Williams CD (2002) The toxicity and efficacy of donor lymphocyte infusions given after reduced-intensity conditioning allogeneic stem cell transplantation. Blood. 100(9):3108–3114
Ivey A, Hills RK, Simpson MA, Jovanovic JV, Gilkes A, Grech A, Patel Y, Bhudia N, Farah H, Mason J, Wall K, Akiki S, Griffiths M, Solomon E, McCaughan F, Linch DC, Gale RE, Vyas P, Freeman SD, Russell N, Burnett AK, Grimwade D, UK National Cancer Research Institute AML Working Group (2016) Assessment of minimal residual disease in standard-risk AML. N Engl J Med 374(5):422–433
Jongen-Lavrencic M, Grob T, Hanekamp D, Kavelaars FG, Al Hinai A, Zeilemaker A et al (2018) Molecular minimal residual disease in acute myeloid leukemia. N Engl J Med 378(13):1189–1199
Yan CH, Liu DH, Liu KY, Xu LP, Liu YR, Chen H, Han W, Wang Y, Qin YZ, Huang XJ (2012) Risk stratification-directed donor lymphocyte infusion could reduce relapse of standard-risk acute leukemia patients after allogeneic hematopoietic stem cell transplantation. Blood. 119(14):3256–3262
Yan CH, Liu QF, Wu DP, Zhang X, Xu LP, Zhang XH et al (2017) Prophylactic donor lymphocyte infusion (DLI) followed by minimal residual disease and graft-versus-host disease-guided multiple DLIs could improve outcomes after allogeneic hematopoietic stem cell transplantation in patients with refractory/relapsed acute leukemia. Biol Blood Marrow Transplant 23(8):1311–1319
Dazzi F, Raanani P, van Rhee F, Olavarria E, Szydlo RM, Apperley JF, et al. (1997) RT-PCR for bcr-abl transcripts in CML patients receiving DLI as treatment for relapse after BMT: differing pattern of molecular response. Bone Marrow Transplant. 19(Suppl 1):S32-S
Chen X, Regn S, Kolb HJ, Roskrow M (1999) The generation of leukemic dendritic cells from patients with chronic myeloid leukemia (CML) using the combination of interferon-à and GM-CSF. Blood. 94(10 Suppl 1):529a-a
Chen X, Regn S, Raffegerst S, Kolb HJ, Roskrow M (2000) Interferon alpha in combination with GM-CSF induces the differentiation of leukaemic antigen-presenting cells that have the capacity to stimulate a specific anti-leukaemic cytotoxic T-cell response from patients with chronic myeloid leukaemia. Br J Haematol 111(2):596–607
Woiciechowsky A, Regn S, Kolb HJ, Roskrow M (2001) Leukemic dendritic cells generated in the presence of FLT3 ligand have the capacity to stimulate an autologous leukaemia-specific cytotoxic T cell response from patients with acute myeloid leukaemia. Leukemia. 15:246–255
Schmetzer HM, Kremser A, Loibl J, Kroell T, Kolb HJ (2007) Quantification of ex vivo generated dendritic cells (DC) and leukemia-derived DC contributes to estimate the quality of DC, to detect optimal DC-generating methods or to optimize DC-mediated T-cell-activation-procedures ex vivo or in vivo 9. Leukemia. 21(6):1338–1341
Anguille S, Lion E, Willemen Y, Van Tendeloo VF, Berneman ZN, Smits EL (2011) Interferon-alpha in acute myeloid leukemia: an old drug revisited. Leukemia. 25(5):739–748
Schroeder T, Czibere A, Platzbecker U, Bug G, Uharek L, Luft T, Giagounidis A, Zohren F, Bruns I, Wolschke C, Rieger K, Fenk R, Germing U, Haas R, Kröger N, Kobbe G (2013) Azacitidine and donor lymphocyte infusions as first salvage therapy for relapse of AML or MDS after allogeneic stem cell transplantation. Leukemia. 27(6):1229–1235
Zeiser R, Beelen DW, Bethge W, Bornhauser M, Bug G, Burchert A et al (2019) Biology-driven approaches to prevent and treat relapse of myeloid Neoplasia after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant 25(4):e128–ee40
Zeiser R, Vago L (2019) Mechanisms of immune escape after allogeneic hematopoietic cell transplantation. Blood. 133(12):1290–1297
Vago L, Perna SK, Zanussi M, Mazzi B, Barlassina C, Stanghellini MT et al (2009) Loss of mismatched HLA in leukemia after stem-cell transplantation. N Engl J Med 361(5):478–488
Christopher MJ, Petti AA, Rettig MP, Miller CA, Chendamarai E, Duncavage EJ, et al. (2018) Immune escape of relapsed aml cells after allogeneic transplantation. N Engl J Med
Toffalori C, Zito L, Gambacorta V, Riba M, Oliveira G, Bucci G, Barcella M, Spinelli O, Greco R, Crucitti L, Cieri N, Noviello M, Manfredi F, Montaldo E, Ostuni R, Naldini MM, Gentner B, Waterhouse M, Zeiser R, Finke J, Hanoun M, Beelen DW, Gojo I, Luznik L, Onozawa M, Teshima T, Devillier R, Blaise D, Halkes CJM, Griffioen M, Carrabba MG, Bernardi M, Peccatori J, Barlassina C, Stupka E, Lazarevic D, Tonon G, Rambaldi A, Cittaro D, Bonini C, Fleischhauer K, Ciceri F, Vago L (2019) Immune signature drives leukemia escape and relapse after hematopoietic cell transplantation. Nat Med 25(4):603–611
Spinner MA, Advani RH, Connors JM, Azzi J, Diefenbach C (2018) New treatment algorithms in Hodgkin lymphoma: too much or too little? Am Soc Clin Oncol Educ Book 38:626–636
Zhou J, Bashey A, Zhong R, Corringham S, Messer K, Pu M, Ma W, Chut T, Soiffer R, Mitrovich RC, Lowy I, Ball ED (2011) CTLA-4 blockade following relapse of malignancy after allogeneic stem cell transplantation is associated with T cell activation but not with increased levels of T regulatory cells. Biol Blood Marrow Transplant 17(5):682–692
Davids MS, Kim HT, Bachireddy P, Costello C, Liguori R, Savell A, Lukez AP, Avigan D, Chen YB, McSweeney P, LeBoeuf N, Rooney MS, Bowden M, Zhou CW, Granter SR, Hornick JL, Rodig SJ, Hirakawa M, Severgnini M, Hodi FS, Wu CJ, Ho VT, Cutler C, Koreth J, Alyea EP, Antin JH, Armand P, Streicher H, Ball ED, Ritz J, Bashey A, Soiffer RJ, Leukemia and Lymphoma Society Blood Cancer Research Partnership (2016) Ipilimumab for patients with relapse after allogeneic transplantation. N Engl J Med 375(2):143–153
Chang YJ, Wang Y, Liu YR, Xu LP, Zhang XH, Chen H, Chen YH, Wang FR, Han W, Sun YQ, Yan CH, Tang FF, Mo XD, Liu KY, Huang XJ (2017) Haploidentical allograft is superior to matched sibling donor allograft in eradicating pre-transplantation minimal residual disease of AML patients as determined by multiparameter flow cytometry: a retrospective and prospective analysis. J Hematol Oncol 10(1):134
Platzbecker U, Wermke M, Radke J, Oelschlaegel U, Seltmann F, Kiani A, Klut IM, Knoth H, Röllig C, Schetelig J, Mohr B, Graehlert X, Ehninger G, Bornhäuser M, Thiede C (2012) Azacitidine for treatment of imminent relapse in MDS or AML patients after allogeneic HSCT: results of the RELAZA trial. Leukemia. 26(3):381–389
Goodyear O, Agathanggelou A, Novitzky-Basso I, Siddique S, McSkeane T, Ryan G, Vyas P, Cavenagh J, Stankovic T, Moss P, Craddock C (2010) Induction of a CD8+ T-cell response to the MAGE cancer testis antigen by combined treatment with azacitidine and sodium valproate in patients with acute myeloid leukemia and myelodysplasia. Blood. 116(11):1908–1918
de Lima M, Giralt S, Thall PF, de Padua SL, Jones RB, Komanduri K et al (2010) Maintenance therapy with low-dose azacitidine after allogeneic hematopoietic stem cell transplantation for recurrent acute myelogenous leukemia or myelodysplastic syndrome: a dose and schedule finding study. Cancer. 116(23):5420–5431
Craddock C, Labopin M, Robin M, Finke J, Chevallier P, Yakoub-Agha I, Bourhis JH, Sengelov H, Blaise D, Luft T, Hallek M, Kroger N, Nagler A, Mohty M (2016) Clinical activity of azacitidine in patients who relapse after allogeneic stem cell transplantation for acute myeloid leukemia. Haematologica. 101(7):879–883
de Lima M, Oran B, Champlin RE, Papadopoulos EB, Giralt SA, Scott BL, William BM, Hetzer J, Laille E, Hubbell B, Skikne BS, Craddock C (2018) CC-486 maintenance after stem cell transplantation in patients with acute myeloid leukemia or myelodysplastic syndromes. Biol Blood Marrow Transplant 24(10):2017–2024
Sommer S, Cruijsen M, Claus R, Bertz H, Wasch R, Marks R et al (2018) Decitabine in combination with donor lymphocyte infusions can induce remissions in relapsed myeloid malignancies with higher leukemic burden after allogeneic hematopoietic cell transplantation. Leuk Res 72:20–26
Metzelder S, Wang Y, Wollmer E, Wanzel M, Teichler S, Chaturvedi A, et al. (2009) Compassionate-use of sorafenib in Flt3-ITD positive acute myeloid leukemia: sustained regression prior and post allogenic stem cell transplantation 1. Blood
Metzelder SK, Schroeder T, Lubbert M, Ditschkowski M, Gotze K, Scholl S et al (2017) Long-term survival of sorafenib-treated FLT3-ITD-positive acute myeloid leukaemia patients relapsing after allogeneic stem cell transplantation. Eur J Cancer 86:233–239
Brunner AM, Li S, Fathi AT, Wadleigh M, Ho VT, Collier K, Connolly C, Ballen KK, Cutler CS, Dey BR, el-Jawahri A, Nikiforow S, McAfee SL, Koreth J, Deangelo DJ, Alyea EP, Antin JH, Spitzer TR, Stone RM, Soiffer RJ, Chen YB (2016) Haematopoietic cell transplantation with and without sorafenib maintenance for patients with FLT3-ITD acute myeloid leukaemia in first complete remission. Br J Haematol 175(3):496–504
Stone RM, Mandrekar SJ, Sanford BL, Laumann K, Geyer S, Bloomfield CD, Thiede C, Prior TW, Döhner K, Marcucci G, Lo-Coco F, Klisovic RB, Wei A, Sierra J, Sanz MA, Brandwein JM, de Witte T, Niederwieser D, Appelbaum FR, Medeiros BC, Tallman MS, Krauter J, Schlenk RF, Ganser A, Serve H, Ehninger G, Amadori S, Larson RA, Döhner H (2017) Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med 377(5):454–464
Stone RM (2018) What FLT3 inhibitor holds the greatest promise? Best Pract Res Clin Haematol 31(4):401–404
Mathew NR, Baumgartner F, Braun L, O'Sullivan D, Thomas S, Waterhouse M, Müller TA, Hanke K, Taromi S, Apostolova P, Illert AL, Melchinger W, Duquesne S, Schmitt-Graeff A, Osswald L, Yan KL, Weber A, Tugues S, Spath S, Pfeifer D, Follo M, Claus R, Lübbert M, Rummelt C, Bertz H, Wäsch R, Haag J, Schmidts A, Schultheiss M, Bettinger D, Thimme R, Ullrich E, Tanriver Y, Vuong GL, Arnold R, Hemmati P, Wolf D, Ditschkowski M, Jilg C, Wilhelm K, Leiber C, Gerull S, Halter J, Lengerke C, Pabst T, Schroeder T, Kobbe G, Rösler W, Doostkam S, Meckel S, Stabla K, Metzelder SK, Halbach S, Brummer T, Hu Z, Dengjel J, Hackanson B, Schmid C, Holtick U, Scheid C, Spyridonidis A, Stölzel F, Ordemann R, Müller LP, Sicre-de-Fontbrune F, Ihorst G, Kuball J, Ehlert JE, Feger D, Wagner EM, Cahn JY, Schnell J, Kuchenbauer F, Bunjes D, Chakraverty R, Richardson S, Gill S, Kröger N, Ayuk F, Vago L, Ciceri F, Müller AM, Kondo T, Teshima T, Klaeger S, Kuster B, Kim D(DH), Weisdorf D, van der Velden W, Dörfel D, Bethge W, Hilgendorf I, Hochhaus A, Andrieux G, Börries M, Busch H, Magenau J, Reddy P, Labopin M, Antin JH, Henden AS, Hill GR, Kennedy GA, Bar M, Sarma A, McLornan D, Mufti G, Oran B, Rezvani K, Shah O, Negrin RS, Nagler A, Prinz M, Burchert A, Neubauer A, Beelen D, Mackensen A, von Bubnoff N, Herr W, Becher B, Socié G, Caligiuri MA, Ruggiero E, Bonini C, Häcker G, Duyster J, Finke J, Pearce E, Blazar BR, Zeiser R (2018) Sorafenib promotes graft-versus-leukemia activity in mice and humans through IL-15 production in FLT3-ITD-mutant leukemia cells. Nat Med 24(3):282–291
Bug G, Burchert A, Wagner EM, Kroger N, Berg T, Guller S et al (2017) Phase I/II study of the deacetylase inhibitor panobinostat after allogeneic stem cell transplantation in patients with high-risk MDS or AML (PANOBEST trial). Leukemia. 31(11):2523–2525
Choi SW, Braun T, Chang L, Ferrara JL, Pawarode A, Magenau JM et al (2014) Vorinostat plus tacrolimus and mycophenolate to prevent graft-versus-host disease after related-donor reduced-intensity conditioning allogeneic haemopoietic stem-cell transplantation: a phase 1/2 trial. Lancet Oncol 15(1):87–95
Buchner T, Schlenk RF, Schaich M, Dohner K, Krahl R, Krauter J et al (2012) Acute myeloid leukemia (AML): different treatment strategies versus a common standard arm--combined prospective analysis by the German AML intergroup. J Clin Oncol 30(29):3604–3610
Estey EH (2018) Acute myeloid leukemia: 2019 update on risk-stratification and management. Am J Hematol 93(10):1267–1291
Burnett AK, Milligan D, Prentice AG, Goldstone AH, McMullin MF, Hills RK et al (2007) A comparison of low-dose cytarabine and hydroxyurea with or without all-trans retinoic acid for acute myeloid leukemia and high-risk myelodysplastic syndrome in patients not considered fit for intensive treatment. Cancer. 109(6):1114–1124
Tilly H, Castaigne S, Bordessoule D, Casassus P, Le Prise PY, Tertian G et al (1990) Low-dose cytarabine versus intensive chemotherapy in the treatment of acute nonlymphocytic leukemia in the elderly. J Clin Oncol 8(2):272–279
Kadia TM, Cortes J, Ravandi F, Jabbour E, Konopleva M, Benton CB, Burger J, Sasaki K, Borthakur G, DiNardo CD, Pemmaraju N, Daver N, Ferrajoli A, Wang X, Patel K, Jorgensen JL, Wang S, O'Brien S, Pierce S, Tuttle C, Estrov Z, Verstovsek S, Garcia-Manero G, Kantarjian H (2018) Cladribine and low-dose cytarabine alternating with decitabine as front-line therapy for elderly patients with acute myeloid leukaemia: a phase 2 single-arm trial. Lancet Haematol 5(9):e411–ee21
Bose P, Vachhani P, Cortes JE (2017) Treatment of relapsed/refractory acute myeloid leukemia. Curr Treat Options in Oncol 18(3):17
Lancet JE, Uy GL, Cortes JE, Newell LF, Lin TL, Ritchie EK, Stuart RK, Strickland SA, Hogge D, Solomon SR, Stone RM, Bixby DL, Kolitz JE, Schiller GJ, Wieduwilt MJ, Ryan DH, Hoering A, Banerjee K, Chiarella M, Louie AC, Medeiros BC (2018) CPX-351 (cytarabine and daunorubicin) liposome for injection versus conventional cytarabine plus daunorubicin in older patients with newly diagnosed secondary acute myeloid leukemia. J Clin Oncol 36(26):2684–2692
DiNardo CD, Pratz K, Pullarkat V, Jonas BA, Arellano M, Becker PS et al (2019) Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 133(1):7–17
DiNardo CD, Rausch CR, Benton C, Kadia T, Jain N, Pemmaraju N et al (2018) Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am J Hematol 93(3):401–407
Wei AH, Tiong IS (2017) Midostaurin, enasidenib, CPX-351, gemtuzumab ozogamicin, and venetoclax bring new hope to AML. Blood. 130(23):2469–2474
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Kolb Consulting UG has consulting contracts with Novartis, Therakos and Eurocept without impact on the presented review.
Research involving human participants
All procedures performed in studies involving human patients were in accordance with the standards of the institutional review boards and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all participants for the treatment as well as the scientific use of the data.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kolb, HJ., Schmid, C. The FLAMSA concept—past and future. Ann Hematol 99, 1979–1988 (2020). https://doi.org/10.1007/s00277-020-04131-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-020-04131-1