
Abstract
Postpartum anemia has been associated with postpartum morbidities, such as depression and poor cognition. However, it is unclear whether postpartum anemia is associated with reduced health-related quality of life. We performed a prospective study to examine the relations between postpartum Hb levels with postpartum health-related quality of life (HRQoL). We collected data from 60 women intending vaginal delivery and assessed HRQoL and maternal fatigue on admission and on the first postpartum day using the RAND 36-Item Short-Form Health Survey (SF-36) and the Multidimensional Fatigue Inventory (MFI), respectively. Maternal Hb levels were measured on admission and on the first postpartum day. We also assessed patients for postpartum depression using the Edinburgh Postpartum Depression Scale (EPDS). We performed unadjusted and multivariate linear regression (adjusting for maternal age, parity, mode of delivery, and race) to assess the associations between postdelivery Hb with each subscale of the SF-36 and MFI. The mean predelivery and postpartum Hb levels were 12.3 (1.2) and 10.8 (1.4) g/dl, respectively. In our unadjusted and adjusted regression analyses, we observed no statistically significant associations between postpartum Hb levels with any SF-36 or MFI subscale (P > 0.05). Based on the EPDS, only one patient was depressed; her postpartum Hb was 11.2 g/dl. Our findings suggest that postpartum Hb levels may not influence HRQoL or fatigue. However, our findings may only apply to women without predelivery anemia, severe blood loss or moderate-to-severe anemia after delivery. Future studies are needed to determine whether postpartum Hb influences HRQoL among women with moderate or severe postpartum anemia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Health-related quality of life (HRQoL) is recognized as an important outcome in clinical and comparative effectiveness studies and in research studies evaluating quality of medical care [1, 2]. Measurements of HRQoL provide important insight into patients’ experiences of medical care and are useful supplements to more traditional physiological or biological indices of health status and recovery after surgery or childbirth [1]. Furthermore, improving HRQoL and well-being is one of four initiatives and foundation measures proposed for Healthy People 2020, a US federal plan for building a healthier nation [3]. These goals directly apply to postpartum women who may experience debilitating disorders of HRQoL, such as depression, fatigue, and pain [4–7]. Identifying determinants of poor maternal health status after delivery, therefore, provides an opportunity to intervene at multiple points on the causal pathway, with the goal of optimizing mothers’ HRQoL.
Postpartum anemia is an underappreciated maternal morbidity with a high prevalence. At 24–48 h after delivery, postpartum anemia (defined as a hemoglobin (Hb) <11 g/dL) can affect 50 % women [8]. Because postpartum anemia has been linked to a number of important postpartum morbidities, including depression, reduced cognition, and fatigue [9–11], the potential detrimental influence of postpartum anemia on maternal and newborn health has important clinical and public health relevance. However, few studies have examined the relations between postpartum Hb levels with different measures of maternal health status, such as impaired physical functioning or fatigue [12]. If studies were to confirm these associations, then a postpartum Hb could be considered as a biomarker for maternal HRQoL or fatigue. Furthermore, women with postpartum anemia could receive early treatment to limit the presence and severity of impaired HRQoL and fatigue.
Therefore, the aim of this prospective exploratory study was to examine whether an association exists between postpartum Hb levels with maternal HRQoL. In our secondary analyses, we assessed the extent of the associations between postpartum Hb levels and maternal fatigue.
Methods
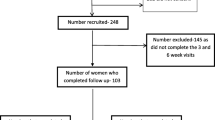
This prospective observational study was approved by the Stanford University Institutional Review Board. We enrolled a total of 63 patients (convenience sample based on investigator availability) intending vaginal delivery, admitted to the labor and delivery unit at Lucile Packard Children’s Hospital, Stanford, California, a large tertiary US obstetric center. Women were enrolled between December 24, 2012 and September 5, 2013. In 2012, a total of 2939 vaginal deliveries occurred at our hospital. Written informed consent was obtained from each patient prior to delivery. Inclusion criteria were women aged 18–50 years admitted in spontaneous labor or for a planned induction of labor. Patients with known hemoglobinopathies, thalessemias, and significant inherited or acquired bleeding disorders and those with severe maternal or obstetrical disease were excluded. We assessed HRQoL and maternal fatigue using two validated survey instruments, the RAND 36-Item Short-Form Survey (SF-36) [13] and the Multidimensional Fatigue Inventory (MFI), respectively [14]. These assessments were made at two time points: on admission to the labor and delivery unit (predelivery) and on the first postpartum day. Using the Edinburgh Postpartum Depression Scale (EPDS) [15], we also assessed patients for postpartum depression on the first postpartum day. Details of each survey instrument are summarized below. Relevant demographic and obstetric data were abstracted from medical records.
The acute RAND/SF-36 (hereafter referred to as SF-36) is a survey instrument designed to measure a patient’s HRQoL over the previous 7 days. The SF-36 provides HRQoL data, which can be used to compare the relative burden of disease and for differentiating health benefits of various treatments. The SF-36 has been validated previously among postpartum women [16]. Each survey comprises a series of 36 multiple-choice questions that assess patients’ perceptions of their health in the following eight domains: physical functioning, role limitations due to physical reasons, role limitations due to emotional reasons, pain, energy, social functioning, mental health, and general health. The overall scores for each domain range from 0 to 100 (with higher scores indicating better health) and are based on answers to a particular set of questions. The physical functioning category, for instance, is based on ten questions that assess the impact of each patient’s health on their physical activity. For each question, respondents may select one of three answers: (1) “yes, limited a lot,” (2) “yes, limited a little,” or (3) “not limited at all.” These answers are then reassigned values based on scoring guidelines (1 = 0, 2 = 50, 3 = 100). Scores from questions in each category are aggregated and a mean score is calculated. Higher scores indicate better functioning or wellbeing. For the postpartum assessment, patients were asked to base their answers on their health status over the preceding 24 h.
The MFI is a 20-item survey that assesses the following five dimensions of fatigue: general fatigue, physical fatigue, mental fatigue, reduced motivation, and reduced activity. The MFI has been used to assess fatigue in a prior study of postpartum women [16]. Patients respond to statements in the survey using a numerical (whole integer) score, anchored at extremes of 1 and 5 (1 = “yes, that is true,” and 5 = “no, that is not true”). Scores range from 4 to 20, with higher scores indicating a greater degree of fatigue.
The EPDS is the most commonly used self-report assessment for postpartum depression [15] and includes ten questions designed to assess the frequency with which the patient has experienced the given symptoms in the previous week. Each item is scored on a scale from 0 to 3, with an overall composite score ranging from 0 (least depressed) to 3 (most depressed). Based on the EPDS scoring guidelines, women with scores ≥10 on the EPDS were classified as depressed [15, 17, 18].
Maternal Hb levels were measured at the time of hospital admission and on the first postpartum day. Because iron deficiency is the most common cause of anemia during pregnancy [19] and ferritin levels are the preferred mode of testing for iron deficiency [20], we also assessed maternal ferritin levels on admission and on the first postpartum day. We calculated the incidence of mild and severe postpartum anemia (Hb < 12 g/dl and Hb < 8 g/dl, respectively), using previous criteria described by the Centers for Disease Control [21] and Prevention and the World Health Organization [22].
Statistical analysis
Data are presented as mean (standard deviation), median [interquartile range], and number (percentages), as appropriate. For our primary analyses, we performed linear regression to assess the association between postpartum Hb with SF-36 physical functioning score. Of all the SF-36 domains, physical functioning has the highest internal consistency, meaning that the questions within the subscale are correlated and thus each measures the same outcome [16]. The score for physical functioning also correlates most closely with the commonly used “physical component summary” measure [23]. For our primary analyses, we performed unadjusted and adjusted linear regression analyses, accounting for the following covariates: maternal age, race/ethnicity, parity, and mode of delivery. We considered P < 0.05 as statistically significant.
For our secondary analyses, we assessed the following associations: postpartum Hb with other SF-36 and MFI domain scores, postpartum ferritin levels with SF-36 and MFI domain scores, and percentage change in Hb and ferritin levels with SF-36 and MFI domain scores. The percentage change was calculated as \( \left(\frac{\mathrm{postdelivery}\ \mathrm{H}\mathrm{b}\ \mathrm{or}\ \mathrm{ferritin}-\mathrm{predelivery}\ \mathrm{H}\mathrm{b}\ \mathrm{or}\ \mathrm{ferritin}}{\mathrm{predelivery}\ \mathrm{H}\mathrm{b}\ \mathrm{or}\ \mathrm{ferritin}}\right)\times 100 \). Lastly, we compared predelivery vs. postdelivery SF-36 scores and MFI scores and postpartum Hb values of women with vs. without postpartum depression (as determined by the EPDS). Continuous variables were compared by paired t tests, Wilcoxon signed-rank test, or Mann-Whitney U test, as appropriate. As our secondary analyses involved multiple comparisons, we considered P < 0.01 as statistically significant. Statistical analysis was performed using STATA version 12.1 (Stata Corp., College Station, TX).
Results
Sixty-three women were enrolled in the study. Three women did not complete the postpartum surveys; reasons for non-completion were not provided. Therefore, the final cohort comprised 60 women who completed predelivery and postdelivery surveys. Demographic, obstetric, and intrapartum characteristics of the study cohort are presented in Table 1. Within our cohort, 53 women (88.3 %) had vaginal delivery and 7 (11.7 %) had cesarean delivery. The median total EBL was 250 ml (191–403). Data on postdelivery Hb levels was missing for two patients. Data on predelivery and postdelivery ferritin levels were missing for one and five patients, respectively. The mean predelivery and postpartum Hb levels were 12.3 (1.2) and 10.8 (1.4) g/dl, respectively. In our cohort, 15/58 women (25.9 %) had a postpartum Hb < 12 g/dl, which meets criteria for postpartum anemia [21, 22], and 1/58 (1.7 %) women had a postpartum Hb < 8 g/dl consistent with severe postpartum anemia [22]. One patient had a postpartum Hb of 7 g/dl; her predelivery Hb was 12.7 g dl and her EBL was 405 ml. Only 9/60 (15 %) women had an EBL >500 ml, and only one patient had an EBL >1000 ml. The median predelivery and postdelivery ferritin levels were 19 (10–35) and 27 (12–46) ng/mL, respectively. Because ferritin levels <12 ng/ml are consistent with iron deficiency [24], we calculated frequencies of women with low predelivery and postdelivery ferritin levels. Using this criteria, 19/59 (32.2 %) and 12/55 (21.8 %) women had low ferritin levels before and after delivery, respectively.
Predelivery and postdelivery HRQoL and maternal fatigue data are presented in Table 2. The median predelivery and postpartum SF-36 physical functioning scores were similar: 55 (45–85) vs. 55 (35–65), respectively (P = 0.06). Compared to the predelivery period, patients reported that limitations due to both physical health and emotional problems worsened in the postpartum period (Table 2). No other prepartum vs. postpartum differences were observed for other SF-36 or MFI subscales (Table 2).
In our unadjusted and adjusted linear regression analyses, we observed no statistically significant associations between postpartum Hb levels and physical functioning on the SF-36 survey (Table 3). In our secondary analyses, we found no statistically significant associations between postpartum Hb with other HRQoL subscales or any MFI subscale (Table 3). Similarly, we found no statistically significant associations between postpartum ferritin levels with any SF-36 or MFI subscale, and no significant associations were observed between the percentage change in Hb or ferritin levels with any SF-36 and MFI subscale (data not presented).
Based on the EPDS, only one woman was depressed, with a total score of 19 out of 30. Her prepartum and postpartum Hb levels were 12.9 and 11.2 g/dl, respectively, and her prepartum and postpartum ferritin levels were 73 and 69 ng/ml, respectively.
Discussion
In this prospective exploratory study, in the early postpartum period, maternal Hb levels were not associated with physical functioning scores on the SF-36 survey. Additionally, neither postpartum Hb nor ferritin levels were associated with other maternal HRQoL or fatigue subscales. These findings suggest that, in the early postpartum period, Hb levels among women who undergo uncomplicated delivery may not influence maternal HRQoL or fatigue.
In our study, we did not find evidence of an association between postpartum Hb and HRQoL. Findings from other studies assessing HRQoL and fatigue according to Hb levels are inconsistent. Our findings are similar to those reported by Van Der Woude et al. who observed no differences in any SF-36 scale or fatigue measure between women with vs. without postpartum anemia; anemia was classified by an Hb <10.5 g/dl [25]. In contrast, Jansen et al. reported that postpartum Hb levels correlated with physical HRQoL and fatigue [12]. In a different study, Prick et al. assessed women with severe postpartum anemia who were randomized to receive red blood cells or no transfusion [26]. At 1 week postpartum, women in the non-intervention group had lower physical functioning HRQoL scores and higher fatigue scores compared to those receiving transfusion. However, these between-group differences were relatively small: 5.5 point difference in the SF-36 physical functioning score (scores range from 0 to 100) and a 1.1 point difference in the MFI physical fatigue score (scores range from 4 to 20).
These conflicting findings may be partly explained by the different postpartum Hb values and timing of postpartum Hb measurement reported across these studies. In our study cohort, the mean postpartum Hb level was 10.8 g/dl, a level which only just met the criteria for mild postpartum anemia as defined by the World Health Organization (10–10.9 g/dl) [22]. In contrast, in the study by Jansen et al [12]., the minimum and maximum Hb levels after vaginal delivery were 7 and 15 g/dl respectively, with Hb levels assessed at 12–24 h after vaginal delivery or 24–48 h after cesarean delivery. Prick et al. [26] recruited women with severe postpartum anemia (Hb levels between 4.8 and 7.9 g/dl) between 12 and 24 h postpartum. Van Der Woude et al. enrolled women who had Hb levels measured within 48 h of delivery [25]. Based on this combined evidence, it is possible that associations may exist between postpartum Hb levels with HRQoL and fatigue, but only for women with moderate or severe postpartum anemia.
Iron deficiency has been associated with maternal and perinatal morbidities during the postpartum period, including postpartum depression [27], impaired mother-child interactions [28], maternal stress, and impaired cognitive functioning [10]. Although 21 % of women had low ferritin levels after delivery, in our secondary analyses, we did not observe any association between postpartum ferritin and a percentage change in ferritin levels with any HRQoL or MFI domain. Further studies are needed to determine whether ferritin levels or other iron indices consistent with severe iron deficiency are associated with key maternal health-related outcomes.
Our study findings also indicate that, compared to the period prior to delivery, role limitations due to physical health and emotional problems worsen in the early postpartum period. Other SF-36 domains and MFI scores did not appear to be significantly affected after delivery. Therefore, limitations due to physical health and emotional problems may be preferable measures for assessing maternal HRQoL in the early postpartum period.
Our study has a number of limitations. The majority of women had predelivery Hb levels that were close to or above the normal range and did not incur excessive blood loss at delivery. Therefore, the majority of postdelivery Hb levels were above thresholds indicative of anemia. Although we found no statistically significant associations between postpartum Hb and ferritin with HRQoL or fatigue, future studies are needed to assess these relations among women with moderate or severe postpartum anemia. Additionally, measures of HRQoL may be influenced by the quality of obstetric, anesthetic, and nursing care during the peripartum period. However, we did not assess patients’ satisfaction with medical or nursing care and therefore could not account for these factors in our adjusted models. Postdelivery Hb and ferritin levels were only measured once after delivery; therefore, we acknowledge that longitudinal studies are needed to assess Hb levels, ferritin levels, and maternal health status beyond 24 h postdelivery.
Ferritin behaves like an acute phase reactant and, in the setting of acute or chronic inflammation, ferritin levels may be disproportionally elevated [29]. This may explain why a higher proportion of women had a low ferritin level predelivery compared to postdelivery (32 vs. 22 %, respectively). We did not collect clinical data on infectious diseases processes, such as chorioamnionitis, laboratory markers of inflammation, nor other delivery-related factors that may explain why ferritin levels increased postpartum. To account for physiological variation of ferritin during pregnancy, other indices, such as serum-soluble transferrin receptor/ferritin ratio, may be more accurate in detecting iron deficiency [9, 30]. In addition, the modest peripartum changes in Hb levels are not consistent with the increase in erythropoietic activity observed in the early puerperium [31]. Further studies are needed to assess whether markers of erythropoietic activity are more closely associated with changes in maternal health indicators.
Our study cohort was chosen to represent a low risk cohort intending vaginal delivery. Although women intending vaginal delivery at other tertiary centers may share similar characteristics to those of our study cohort, it is uncertain whether our findings are generalizable to women delivering at non-tertiary obstetric centers. Because only one patient met the criteria for postpartum depression, we were unable to perform statistical analyses to compare Hb or ferritin levels between women with vs. without postpartum depression. A larger study cohort would be ideal for performing relevant comparative analyses.
In conclusion, our findings suggest that, in the early postpartum period, maternal Hb or ferritin levels are not associated with maternal health status indicators after delivery. However, few patients in our study cohort had postpartum Hb levels indicative of moderate or severe anemia. Therefore, our findings likely only apply to women without predelivery anemia and excessive blood loss at delivery. Future studies are needed to determine whether postpartum women with severe iron deficiency anemia incur impaired HRQoL, fatigue, or postpartum depression and to assess whether relevant hematologic indices are potentially worthwhile markers of these adverse maternal outcomes.
References
Wilson IB, Cleary PD (1995) Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. Jama 273:59–65
Ware JE Jr, Brook RH, Davies AR, Lohr KN (1981) Choosing measures of health status for individuals in general populations. Am J Public Health 71:620–625
U.S. Department of Health and Human Services Healthy people (2020) Office of disease prevention health promotion., https://www.healthypeople.gov/
Brown S, Lumley J (2000) Physical health problems after childbirth and maternal depression at six to seven months postpartum. BJOG 107:1194–1201
Webb DA, Bloch JR, Coyne JC, Chung EK, Bennett IM, Culhane JF (2008) Postpartum physical symptoms in new mothers: their relationship to functional limitations and emotional well-being. Birth 35:179–187
Sakala C, Declercq ER, Corry MP (2002) Listening to mothers: the first national U.S. survey of women’s childbearing experiences. J Obstet Gynecol Neonatal Nurs 31:633–634
Schytt E, Lindmark G, Waldenstrom U (2005) Physical symptoms after childbirth: prevalence and associations with self-rated health. BJOG 112:210–217
Bergmann RL, Richter R, Bergmann KE, Dudenhausen JW (2010) Prevalence and risk factors for early postpartum anemia. Eur J Obstet Gynecol Reprod Biol 150:126–131
Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L (2016) Iron deficiency anaemia. Lancet 387:907–916
Beard JL, Hendricks MK, Perez EM, Murray-Kolb LE, Berg A, Vernon-Feagans L, Irlam J, Isaacs W, Sive A, Tomlinson M (2005) Maternal iron deficiency anemia affects postpartum emotions and cognition. J Nutr 135:267–272
Corwin EJ, Murray-Kolb LE, Beard JL (2003) Low hemoglobin level is a risk factor for postpartum depression. J Nutr 133:4139–4142
Jansen AJ, Duvekot JJ, Hop WC, Essink-Bot ML, Beckers EA, Karsdorp VH, Scherjon SA, Steegers EA, van Rhenen DJ (2007) New insights into fatigue and health-related quality of life after delivery. Acta Obstet Gynecol Scand 86:579–584
Ware JE Jr, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30:473–483
Smets EM, Garssen B, Bonke B, De Haes JC (1995) The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res 39:315–325
Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 150:782–786
Jansen AJ, Essink-Bot ML, Duvekot JJ, van Rhenen DJ (2007) Psychometric evaluation of health-related quality of life measures in women after different types of delivery. J Psychosom Res 63:275–281
Murray L, Carothers AD (1990) The validation of the Edinburgh Post-natal Depression Scale on a community sample. Br J Psychiatry 157:288–290
Harris B, Huckle P, Thomas R, Johns S, Fung H (1989) The use of rating scales to identify post-natal depression. Br J Psychiatry 154:813–817
Milman N (2008) Prepartum anaemia: prevention and treatment. Ann Hematol 87:949–959
WHO/UNICEF/UNU (2001) Iron deficiency anaemia: assessment, prevention and control, a guide for programme managers. World Health Organization, Geneva
Centers for Disease Control and Prevention (1998) Recommendations to prevent and control iron deficiency in the United States. MMWR Recomm Rep 47:1–29
World Health Organization (2011) Haemoglobin concentrations for the diagnosis of anemia and assessment of severity. Vitamin and mineral nutrition information system. Department of Reproductive Health and Research, WHO, Geneva
Ware JE Jr, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A (1995) Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med Care 33:AS264–AS279
Milman N (2006) Iron and pregnancy—a delicate balance. Ann Hematol 85:559–565
Van Der Woude D, Pijnenborg JM, Verzijl JM, Van Wijk EM, De Vries J (2014) Health status and fatigue of postpartum anemic women: a prospective cohort study. Eur J Obstet Gynecol Reprod Biol 181:119–123
Prick BW, Jansen AJ, Steegers EA, Hop WC, Essink-Bot ML, Uyl-de Groot CA, Akerboom BM, van Alphen M, Bloemenkamp KW, Boers KE, Bremer HA, Kwee A, van Loon AJ, Metz GC, Papatsonis DN, van der Post JA, Porath MM, Rijnders RJ, Roumen FJ, Scheepers HC, Schippers DH, Schuitemaker NW, Stigter RH, Woiski MD, Mol BW, van Rhenen DJ, Duvekot JJ (2014) Transfusion policy after severe postpartum haemorrhage: a randomised non-inferiority trial. BJOG 121:1005–1014
Albacar G, Sans T, Martin-Santos R, Garcia-Esteve L, Guillamat R, Sanjuan J, Canellas F, Gratacos M, Cavalle P, Arija V, Gaviria A, Gutierrez-Zotes A, Vilella E (2011) An association between plasma ferritin concentrations measured 48 h after delivery and postpartum depression. J Affect Disord 131:136–142
Murray-Kolb LE, Beard JL (2009) Iron deficiency and child and maternal health. Am J Clin Nutr 89:946S–950S
Lipschitz DA, Cook JD, Finch CA (1974) A clinical evaluation of serum ferritin as an index of iron stores. N Engl J Med 290:1213–1216
Milman N (2011) Postpartum anemia I: definition, prevalence, causes, and consequences. Ann Hematol 90:1247–1253
Richter C, Huch A, Huch R (1995) Erythropoiesis in the postpartum period. J Perinat Med 23:51–59
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was supported by the Department of Anesthesiology, Perioperative, and Pain Medicine, Stanford University School of Medicine. A.J.B was supported by an award from the Eunice Kennedy Shriver National Institute of Child Health and Development (K23HD070972).
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Miller, C.M., Ramachandran, B., Akbar, K. et al. The impact of postpartum hemoglobin levels on maternal quality of life after delivery: a prospective exploratory study. Ann Hematol 95, 2049–2055 (2016). https://doi.org/10.1007/s00277-016-2817-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-016-2817-5