
Abstract
Large and systematic studies of non-Hodgkin lymphoma (NHL) in the Far East (FE) with good comparative data are scarce in the literature. In this study, five expert hematopathologists classified 730 consecutive cases of newly-diagnosed NHL from four sites in the FE (excluding Japan) using the World Health Organization classification. The results were compared to 399 cases from North America (NA). We found a significantly higher male to female ratio in the FE compared to NA (1.7 versus 1.1; p < 0.05). The median ages of patients with low-grade (LG) and high-grade (HG) B-NHL in the FE (58 and 51 years, respectively) were significantly lower than in NA (64 and 68 years, respectively). The FE had a significantly lower relative frequency of B-NHL and a higher frequency of T-NHL (82 vs. 18 %) compared to NA (90.5 vs. 9.5 %). Among mature B cell lymphomas, the FE had a significantly higher relative frequency of HG B-NHL (54.8 %) and a lower frequency of LG B-NHL (27.2 %) than NA (34.3 and 56.1 %, respectively). Diffuse large B cell lymphoma was more common in the FE (49.4 %) compared to NA (29.3 %), whereas the relative frequency of follicular lymphoma was lower in the FE (9.4 %) compared to NA (33.6 %). Among T-NHL, nasal NK/T cell NHL was more frequent in the FE (5.2 %) compared to NA (0 %). Peripheral T cell lymphoma was also more common in the FE (9.1 %) than in NA (5.3 %). Further epidemiologic studies are needed to better understand the pathobiology of these differences.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Non-Hodgkin lymphoma (NHL) consists of many biologically distinctive disease subtypes, as listed in the 2008 World Health Organization (WHO) classification [1]. The relative frequencies of the various NHL subtypes vary by age, sex, and race/ethnicity, with significant geographic differences [2, 3], suggesting that multiple environmental and lifestyle factors, in addition to host genetic makeup, play a role in the development of NHL [4].
Numerous epidemiologic studies have investigated the etiologic factors that contribute to NHL risk such as immune modulation, infections with various viruses and bacteria, and lifestyle factors such as diet, occupational exposures, and host factors [4, 5]. Furthermore, the relative distribution of NHL subtypes has been reported in numerous studies from different geographic regions including North America (NA) [2, 6], Central and South America (CSA) [3], Europe [2, 6], Africa [7, 8], the Middle East (ME) [9–14] and Far East (FE) [15–22], and Australia [23].
One goal of the International NHL Classification Project was to investigate the geographic differences in NHL subtype distribution, as well as the clinical features, in various countries around the world [2, 6]. During the last 18 years (1995–2012), the project investigators have visited 26 sites (24 countries) in six geographic regions around the world, including four sites in the Far East. The aim of this study is to report the relative distribution of NHL subtypes in different countries of the FE and compare the data to a cohort from NA [2]. To our knowledge, this is the first large and systematic study of NHL subtype distribution in the FE that involves multiple countries with good comparative data.
Materials and methods
International NHL classification project
Four institutions from three countries in the FE, including China (Hong Kong and Shanghai), Indonesia, and Thailand, participated in the study. All participating institutions were academic centers. Japan was not included in the study. Each institution was instructed to collect 200 consecutive, newly diagnosed and untreated cases of NHL. These cases were accrued between the years 1988 and 2008. The design of the current study is the same as to that of the original study by the International NHL Classification Project [3, 6].
At each site, hematoxylin and eosin-stained slides, immunostains, pathology reports, clinical data, and the results of ancillary studies were organized for review. A panel of five expert hematopathologists (J. D., K. A. M., H. K. M-H., B. N. N., and D. D. W) then reviewed all of the collected cases using the 2001 World Health Organization classification [3, 24]. Each expert independently reviewed all of the materials available for each case, including the clinical data, at the same time and recorded a diagnosis. A consensus diagnosis was reached when at least four of the experts agreed on the diagnosis. However, a consensus on the grade of follicular lymphoma was reached when at least three experts agreed on the grade. For cases in which a consensus diagnosis could not be reached, a specific diagnostic algorithm for each case was developed and agreed upon by the group of experts. Requested clinical data and materials, either paraffin blocks or unstained slides from each site, were then sent to one of the experts who performed additional ancillary testing and assigned the case to a diagnostic category based on the algorithm. For cases in which a specific NHL subtype could not be established because of suboptimal morphology or inadequate or insufficient material, the diagnostic categories of unclassifiable low-grade or high-grade NHL were used. The data from the FE was then compared to a cohort of 399 previously published NA cases accrued in Omaha, Nebraska, and Vancouver, British Columbia [2]. Approval for this study was obtained from the Institutional Review Board at the University of Nebraska Medical Center and at each of the participating institutions as required by individual institutional policy. This study was conducted in accordance with the Declaration of Helsinki.
For this analysis, only information on age and sex is included because the clinical data collected at the various institutions was often incomplete and quite variable. Cases of composite lymphoma were classified according to the low-grade component. Mature B cell NHL was further subdivided into low- and high-grade subgroups, with the low-grade subgroup including cases of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), lymphoplasmacytic lymphoma (LPL), mantle cell lymphoma (MCL), follicular lymphoma (FL, all grades), marginal zone lymphoma (MZL, all types), and cases of unclassifiable low-grade B cell lymphoma. The high-grade B cell lymphoma subgroup included cases of diffuse large B cell lymphoma (DLBCL), primary mediastinal B cell lymphoma, Burkitt lymphoma (BL), high-grade B cell lymphoma, Burkitt-like, and cases of unclassifiable high-grade B cell lymphoma. Because of the small number of cases of T cell lymphoma, cases of peripheral T cell lymphoma, not otherwise specified, angioimmunoblastic T cell lymphoma, anaplastic large T/null cell lymphoma, hepatosplenic T cell lymphoma, subcutaneous panniculitis-like T cell lymphoma, and enteropathy-associated T cell lymphoma were all grouped together under the general category of peripheral T cell lymphoma (PTCL).
Statistical analysis
Data analysis was done using SAS software version 9.3 (SAS Institute Inc, Cary, NC). Comparisons of medians for continuous variables were conducted using the Wilcoxon rank sum test. Comparisons of categorical variables were done using chi-square or Fisher's exact tests; the latter was used when the chi-square test may not have been valid due to small numbers. P values for pairwise comparisons were adjusted using the Bonferroni method, and P values less than 0.05 were considered statistically significant.
Results
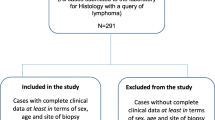
Of the 730 cases reviewed in the FE, including 231 from Shanghai, 199 from Hong Kong, 200 from Indonesia, and 100 from Thailand, 673 cases (92.2 %) were confirmed to be NHL, and 57 cases (7.8 %) with diagnoses other than NHL were excluded from further analysis. Among the latter cases, 18 were Hodgkin lymphoma, 19 had diagnoses other than lymphoma, and 20 were unclassifiable cases. We compared the number of reclassified cases between the FE and NA (1.0 %) and found a significantly higher number of reclassified cases in the FE (p < 0.05).
The overall distribution of NHL subtypes in the FE and the distribution by individual site are shown in Table 1. Of the 673 cases, 552 (82 %) were B cell lymphomas, and 121 (18 %) were T cell lymphomas. The FE had a significantly lower relative frequency of B-NHL (82 %) and a higher frequency of T-NHL (18 %) compared to NA (90.5 and 9.5 %, respectively; p < 0.05). Furthermore, among mature B cell lymphomas, the FE had a significantly higher relative frequency of HG B-NHL (54.8 %) and a lower frequency of LG B-NHL (27.2 %) than NA (34.3 and 56.1 %, respectively; Table 2). Comparison of the individual FE sites with NA showed a significantly higher relative frequency of HG B-NHL in Shanghai, Indonesia, and Thailand and significantly lower frequencies of LG B-NHL in all four FE sites. Furthermore, Indonesia had a lower relative frequency of LG B-NHL and a higher frequency of HG B-NHL when compared to the rest of the FE, whereas Hong Kong had a lower frequency of HG B-NHL. When we compared the relative frequency of T-NHL at the individual sites with NA, we found that Shanghai and Hong Kong had significantly higher frequencies. Hong Kong also had a higher relative frequency of T-NHL compared to the rest of the FE. We also examined the relative frequencies of T-NHL, and LG and HG B-NHL by age groups (≤60 and >60 years), and the findings were very similar to the data shown in Tables 1 and 2.
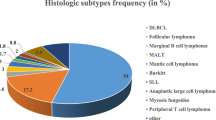
Among the B cell lymphomas (Table 1), DLBCL was the most common subtype (50.5 %), and it was the most common NHL at all four FE sites. Follicular lymphoma (9.4 %) was the second most common subtype in the region, as well as in Shanghai (14.6 %) and Thailand (9.3 %). Follicular lymphoma was uncommon (3.6 %) in Indonesia. Marginal zone lymphoma of MALT type was common in Hong Kong (13.5 %), where it was the second most common subtype, whereas this subtype was infrequent in Shanghai (1.8 %). Mantle cell lymphoma was relatively frequent in Shanghai (5.8 %), whereas plasmacytoma (4.2 %) and BL (6 %) were common in Indonesia.
The data from the FE was then compared to NA, and it demonstrated a significantly higher relative frequency of DLBCL (50.5 vs. 29.3 %, respectively) and a lower frequency of FL (9.4 vs. 33.6 %, respectively) in the FE (Table 1). Analysis of DLBCL showed that of this subtype was more common in all four sites compared to NA. Furthermore, FL was less common in four sites. Compared to the other FE sites, the relative frequency of DLBCL was lower in Hong Kong and higher in Indonesia, whereas FL was lower in Indonesia and higher in Shanghai. Marginal zone lymphoma of MALT type was more frequent in Hong Kong and less frequent in Shanghai compared to both NA and the rest of the region. The relative frequency of MCL was significantly lower, and plasmacytoma was significantly higher in the FE than in NA. Indonesia had a high relative frequency of plasmacytoma compared to NA and rest of the FE. Finally, BL was more frequent in Indonesia than in NA or the rest of the region.
Among T-NHL, PTCL was the most common subtype in all sites except Thailand, where nasal NK/T cell lymphoma (5.8 %) was the most common. Nasal NK/T cell lymphoma was also common in Shanghai (4.9 %) and Hong Kong (8.3 %), and precursor T lymphoblastic lymphoma was relatively common in Shanghai (4.9 %). Compared to NA, the FE had a significantly higher relative frequency of PTCL and nasal NK/T cell lymphoma. As for the individual sites, the relative frequency of PTCL was higher in Hong Kong, and the frequency of nasal NK/T cell lymphoma was higher in both Shanghai and Hong Kong compared to NA.
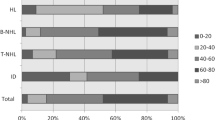
The distribution of NHL by sex and age is shown in Table 3. The age of patients in the FE ranged from 1 to 98 years, and 62.3 % were male. The FE had a significantly higher number of male patients compared to NA (52.9 %). The median ages of patients with LG B-NHL (58 years) and HG B-NHL (51 years) were significantly lower in the FE than in NA (64 and 68 years, respectively). The lower median age of patients with HG B-NHL was observed in all sites in the region. Indonesia also had a significantly lower median age of LG B-NHL patients compared to both NA and the rest of the FE. There was no significant difference in median age of patients with T-NHL between the FE and NA. However, Indonesia had a significantly lower median age for T-NHL when compared to the rest of the region.
Discussion
This large and systematic study of NHL subtypes included 730 cases initially diagnosed as NHL at four sites in the FE. Of the 730 cases, 673 cases (92.2 %) were confirmed to be NHL, and 57 cases (7.8 %) were excluded from further analysis since they were found to have diagnoses other than NHL. The FE had significantly more misclassified cases compared to NA. We have also found a high rate of misclassified cases in other developing countries in Central and South America (CSA) [3], eastern Europe, and North Africa/Middle East (manuscripts in preparation). Furthermore, a recent study from Taiwan [25] that examined discrepancies in lymphoma diagnosis between general pathologists and hematopathologists found the rate of discrepancy to be over 50 %. These findings indicate that lymphoma pathology is challenging in developing and resource-poor countries where pathologists lack subspecialty training and the technology needed to correctly diagnose lymphomas.
The distribution of NHL subtypes in the FE was very different from NA. The FE had a significantly higher relative frequency of T-NHL and a lower frequency of B-NHL compared to NA. These differences were observed in the two sites in China, but not in Indonesia and Thailand. Also, a higher relative frequency of HG B-NHL and a lower frequency of LG B-NHL were observed in the FE compared to NA, and these differences were seen at all sites in the region. The most common lymphoma in the FE was DLBCL, whereas the relative frequency of FL was low. This distribution of LG and HG B-NHL, with a high relative frequency of DLBCL and low frequency of FL, is similar to that reported in other studies from the FE [15–22], as well as the Middle East [9–13] and CSA [3] and suggests that socioeconomic status [26, 27] plays a significant role in lymphoma development (Table 4). Another factor that has been associated with the development of FL is a high intake of meat and saturated fat [28–30]. Therefore, we compared meat consumption per capita in the countries of the FE and NA (Table 4) [31] and found that Shanghai, Thailand, and Indonesia have significantly lower meat consumption, whereas Hong Kong was more similar to NA. However, the relative frequencies of FL in the FE sites did not correlate with meat consumption, indicating that other etiologic factors contribute to the development of FL in the FE.
We observed a high relative frequency of MZL of MALT type in Hong Kong (13.5 %), significantly higher than in NA and the rest of the FE. Most epidemiologic studies from the FE [15–19, 21, 22] have reported a lower frequency of MZL of MALT type, ranging from 2.5 to 9.7 %, whereas one study from Korea reported a frequency of 13 % [20]. The cause of the high relative frequency of MZL of MALT type in Hong Kong is not clear but could potentially be attributed to the time period (1988–1990) when these cases were accrued, during which the prevalence of Helicobacter pylori (H. pylori) infection was relatively high in the FE [32]. More recently, the prevalence of H. pylori infection has been steadily declining in Asia [32, 33] with significantly higher rates observed in the 1990s than after the year 2000. Since H. pylori is one of the main etiologic factors associated with MZL of MALT type [1], this decrease in H. pylori prevalence has likely led to a decreased frequency of MZL of MALT type in the FE. Of note, the epidemiologic studies from the FE referenced above were all published after the year 2004 [16–22], with the exception of one Japanese study published in 2000 [15]. Further study of recent cases of MZL of MALT type in Hong Kong would be of interest to see whether the relative frequency has remained stable or decreased over time.
A high relative frequency of BL was observed in Indonesia (6 %), significantly higher than in the other FE countries or NA. A review of the literature did not reveal any other studies from Indonesia that have reported on the frequency of NHL subtypes. However, other studies from the FE [17–22] have reported BL frequencies ranging from 1.1 to 4.1 %. Epstein-Barr virus (EBV) infection is an important cause of BL [1], and the occurrence of EBV in BL is higher in developing countries where EBV seroconversion occurs at an early age [34]. To the best of our knowledge, there are no studies from Indonesia that reported on the seroprevalence of EBV in the population or the frequency of EBV in BL, but it is likely that these are endemic cases based on the latitude of Indonesia. Another interesting finding in Indonesia was the high relative frequency of plasmacytoma (4.2 %), which was markedly higher than in the other countries of the FE or NA. An explanation for this finding is also unclear, but a study from Korea reported an association between EBV and plasmacytoma of the gastrointestinal tract [35]. In the series from Korea, plasmacytoma comprised 6.4 % of all gastrointestinal NHL, which was significantly higher than in a Japanese cohort (0.7 %) also reported in this paper. Of four Korean plasmacytoma cases tested, two were positive for EBV. Despite the small numbers, these findings suggested an association between EBV and plasmacytoma in Korea. In our study, we did not perform EBV studies on the BL or plasmacytoma cases and, therefore, we are unsure if an association with EBV exists in our series. However, the high relative frequency of BL and plasmacytoma in Indonesia suggests a possible role for EBV in lymphoma development in this country, and studies to confirm this hypothesis should be performed.
The FE had a significantly higher proportion of T-NHL compared to NA, with the highest relative frequencies observed in Hong Kong and Shanghai. Among the T cell lymphomas, nasal NK/T cell lymphoma and PTCL were more common in the FE than in NA. Other studies from the FE have also reported a high proportion of T-NHL, ranging from 13.3 to 25.5 % [15–20, 22]. The relative frequency of PTCL in reports from the FE ranges from 7.7 to 18.6 % (median 11.6 %), which is comparable to our study [15–22]. The relative frequency of nasal NK/T cell lymphoma reported in different Asian countries ranges from 0.6 to 17.1 % (median 3.1 %), which is slightly lower than in our cohort [15, 17–22]. Nasal NK/T cell lymphoma is strongly associated with EBV infection [1, 36]. We also observed a high relative frequency of nasal NK/T cell lymphoma in our study from CSA, especially among Native American populations in Guatemala, Chile, and Peru [3, 37]. Asian and Native American populations share a common genetic background [38], which suggests a genetic susceptibility to develop nasal NK/T cell lymphoma. Furthermore, studies have shown a similar high incidence of this lymphoma among both foreign-born and US-born Asians, providing further evidence of genetic susceptibility to this disease [39–41].
The median age of patients with B-NHL in the FE was significantly lower than in NA, and this difference was observed in both LG (58 years) and HG B-NHL (51 years). This finding was more pronounced in HG B-NHL with the patients at all four sites being significantly younger than in NA. However, there was no significant age difference among T-NHL patients in the FE and NA. Other studies from the FE have also reported a lower median age for B-NHL, ranging from 49.7 to 60 years, whereas the median age for T-NHL ranged from 43.7 to 52.1 years which is similar to our study [17–20, 22]. We also observed a lower median age of B-NHL patients in our study from CSA [3]. Similarly, studies from developing countries in North Africa and the Middle East have also reported lower median ages for B-NHL [9–11, 13, 42]. Our findings, together with other reported studies, indicate that B-NHL occurs earlier in life in developing countries compared to the western world, suggesting that socioeconomic and lifestyle factors play an important role in lymphomagenesis. Furthermore, the FE had a significantly higher number of male patients compared to NA (male to female ratio, 1.7:1.1). Several studies from the FE have also reported male to female ratios in NHL patients ranging from 1.3 to 2:1, which are similar to our findings [18–20, 22]. Even though lymphomas are generally more common in males [43], the reason for the significant difference in gender distribution observed in our study is not clear, and further studies are needed to confirm and explain these differences.
In conclusion, our study represents the first large and systematic study to examine the distribution of NHL subtypes in several countries of the FE. We have found significant differences in the relative frequencies of various NHL subtypes between the FE and NA, as well as differences in the age and gender distribution of NHL. These findings suggest differences in etiologic risk factors, and further large epidemiologic studies are needed in this region to better understand the pathobiology of these differences. Since the cases from NA and Hong Kong were accrued during an earlier time period (1988–1990) than cases from the other sites (1990–2008), some of the differences we observed might be due to the rapid industrialization and westernization which has occurred in the FE in recent years. This possibility also requires further study.
References
Swerdlow SH, Campo E, Harris NL et al (2008) World Health Organization classification of tumours of haematopoietic and lymphoid tissues. IARC, Lyon
Anderson JR, Armitage JO, Weisenburger DD (1998) Epidemiology of the non-Hodgkin’s lymphomas: distributions of the major subtypes differ by geographic locations. Non-Hodgkin’s lymphoma classification project. Ann Oncol 9:717–720
Laurini JA, Perry AM, Boilesen E et al (2012) Classification of non-Hodgkin lymphoma in Central and South America: a review of 1028 cases. Blood 120:4795–4801
Chiu BC, Hou N (2015) Epidemiology and etiology of non-Hodgkin lymphoma. Cancer Treat Res 165:1–25
Alexander DD, Mink PJ, Adami HO et al (2007) The non-Hodgkin lymphomas: a review of the epidemiologic literature. Int J Cancer 120(Suppl 12):1–39
A clinical evaluation of the International Lymphoma Study Group Classification of non-Hodgkin’s lymphoma. The Non-Hodgkin’s Lymphoma Classification Project. (1007) Blood 89:3909-3918
Cool CD, Bitter MA (1997) The malignant lymphomas of Kenya: morphology, immunophenotype, and frequency of Epstein-Barr virus in 73 cases. Hum Pathol 28:1026–1033
Chetty M, Sudi S, Abayomi EA (2012) Prevalence and spectrum of head and neck lymphomas at Tygerberg hospital, South Africa, 2003 to 2007. SADJ 67:270–272, 4,276-277
Castella A, Joshi S, Raaschou T, Mason N (2001) Pattern of malignant lymphoma in the United Arab Emirates—a histopathologic and immunologic study in 208 native patients. Acta Oncol 40:660–664
Almasri NM, Habashneh MA, Khalidi HS (2004) Non-Hodgkin lymphoma in Jordan. Types and patterns of 111 cases classified according to the WHO classification of hematological malignancies. Saudi Med J 25:609–614
Ameen R, Sajnani KP, Albassami A, Refaat S (2010) Frequencies of non-Hodgkin’s lymphoma subtypes in Kuwait: comparisons between different ethnic groups. Ann Hematol 89:179–184
Mozaheb Z, Aledavood A, Farzad F (2011) Distributions of major sub-types of lymphoid malignancies among adults in Mashhad, Iran. Cancer Epidemiol 35:26–29
Yaqo RT, Hughson MD, Sulayvani FK, Al-Allawi NA (2011) Malignant lymphoma in northern Iraq: a retrospective analysis of 270 cases according to the World Health Organization classification. Indian J Cancer 48:446–451
Otrock ZK, Saab J, Aftimos G et al (2013) A collaborative nationwide lymphoma study in Lebanon: incidence of various subtypes and analysis of associations with viruses. Pathol Oncol Res 19:715–722
Lymphoma study group of Japanese pathologists (2000) The World Health Organization classification of malignant lymphomas in Japan: incidence of recently recognized entities. Pathol Int 50:696–702
Sukpanichnant S (2004) Analysis of 1983 cases of malignant lymphoma in Thailand according to the World Health Organization classification. Hum Pathol 35:224–230
Lee MY, Tan TD, Feng AC, Liu MC (2006) Clinicopathological analysis of 598 malignant lymphomas in Taiwan: seven-year experience in a single institution. Am J Hematol 81:568–575
Gross SA, Zhu X, Bao L, Ryder J, Le A, Chen Y, Wang XQ, Irons RD (2008) A prospective study of 728 cases of non-Hodgkin lymphoma from a single laboratory in Shanghai, China. Int J Hematol 88:165–173
Chen WL, Tsai WC, Chao TY, Sheu LF, Chou JM, Kao WY, Chen YC, Ho CL (2010) The clinicopathological analysis of 303 cases with malignant lymphoma classified according to the World Health Organization classification system in a single institute of Taiwan. Ann Hematol 89:553–562
Yoon SO, Suh C, Lee DH, Chi HS, Park CJ, Jang SS, Shin HR, Park BH, Huh J (2010) Distribution of lymphoid neoplasms in the republic of Korea: analysis of 5318 cases according to the World Health Organization classification. Am J Hematol 85:760–764
Yang QP, Zhang WY, Yu JB et al (2011) Subtype distribution of lymphomas in southwest China: analysis of 6,382 cases using WHO classification in a single institution. Diagn Pathol 6(77):1596
Sun J, Yang Q, Lu Z et al (2012) Distribution of lymphoid neoplasms in China: analysis of 4,638 cases according to the World Health Organization classification. Am J Clin Pathol 138:429–434
van Leeuwen MT, Turner JJ, Joske DJ et al (2014) Lymphoid neoplasm incidence by WHO subtype in Australia 1982–2006. Int J Cancer 135:2146–2156
Jaffe ES, Harris NL, Stein H et al (2001) World Health Organization classification of tumours: pathology and genetics of tumours of haematopoietic and lymphoid tissues. IARC Press, Lyon
Chang C, Huang SW, Su IJ, Chang KC (2014) Hematopathologic discrepancies between referral and review diagnoses: a gap between general pathologists and hematopathologists. Leuk Lymphoma 55:1023–1030
The World Bank database. GDP per capita. [Accessed April 16, 2015]. http://data.worldbank.org/indicator/NY.GDP.PCAP.CD
China Statistical Yearbook [Accessed April 16, 2015]. http://www.stats.gov.cn/tjsj/ndsj/2014/indexeh.htm
Cross AJ, Ward MH, Schenk M et al (2006) Meat and meat-mutagen intake and risk of non-Hodgkin lymphoma: results from a NCI-SEER case-control study. Carcinogenesis 27:293–297
Aschebrook-Kilfoy B, Ollberding NJ, Kolar C et al (2012) Meat intake and risk of non-Hodgkin lymphoma. Cancer Causes Control 23:1681–1692
Ollberding NJ, Aschebrook-Kilfoy B, Caces DB, Wright ME, Weisenburger DD, Smith SM, Chiu BC (2013) Phytanic acid and the risk of non-Hodgkin lymphoma. Carcinogenesis 34:170–175
Food and Agriculture Organization of the United Nations—The State of Food and Agriculture 2009. Table A3: Per capita consumption of livestock products, 1995-2005. [Accessed March 1, 2015]. http://www.fao.org/docrep/012/i0680e/i0680e.pdf
Tan HJ, Goh KL (2008) Changing epidemiology of Helicobacter pylori in Asia. J Dig Dis 9:186–189
Lim SH, Kwon JW, Kim N et al (2013) Prevalence and risk factors of helicobacter pylori infection in Korea: nationwide multicenter study over 13 years. BMC Gastroenterol 13:104, 230X-13-104
Anwar N, Kingma DW, Bloch AR et al (1995) The investigation of Epstein-Barr viral sequences in 41 cases of Burkitt's lymphoma from Egypt: epidemiologic correlations. Cancer 76:1245–1252
Tomita Y, Ohsawa M, Hashimoto M, Qiu K, Yang WI, Park CI, Aozasa K (1998) Plasmacytoma of the gastrointestinal tract in Korea: higher incidence than in Japan and Epstein-Barr virus association. Oncology 55:27–32
Vose J, Armitage J, Weisenburger D, International T-Cell Lymphoma Project (2008) International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol 26:4124–4130
Perry AM, Molina-Kirsch H, Nathwani BN et al (2011) Classification of non-Hodgkin lymphomas in Guatemala according to the World Health Organization system. Leuk Lymphoma 52:1681–1688
Morton LM, Wang SS, Devesa SS, Hartge P, Weisenburger DD, Linet MS (2006) Lymphoma incidence patterns by WHO subtype in the United States, 1992–2001. Blood 107:265–276
Herrinton LJ, Goldoft M, Schwartz SM, Weiss NS (1996) The incidence of non-Hodgkin’s lymphoma and its histologic subtypes in Asian migrants to the United States and their descendants. Cancer Causes Control 7:224–230
Au WY, Gascoyne RD, Klasa RD et al (2005) Incidence and spectrum of non-Hodgkin lymphoma in Chinese migrants to British Columbia. Br J Haematol 128:792–796
Pan JW, Cook LS, Schwartz SM, Weis NS (2002) Incidence of leukemia in Asian migrants to the United States and their descendants. Cancer Causes Control 13:791–795
Goldman L, Ezzat S, Mokhtar N et al (2009) Viral and non-viral risk factors for non-Hodgkin’s lymphoma in Egypt: heterogeneity by histological and immunological subtypes. Cancer Causes Control 20:981–987
Surveillance, Epidemiology, and End Results (SEER) Program. SEER Stat Fact Sheets: Non-Hodgkin Lymphoma. [Accessed March 1, 2015]. http://seer.cancer.gov/statfacts/html/nhl.htm
Acknowledgments
We thank all the following pathologists and hematologists who contributed to this study: F. Ho, R. Liang, and W. Au (University of Hong Kong Queen Mary Hospital, Pokfulam, Hong Kong); E. S. R. Hardjolukito (Fakultas Kedokteran Universitas Indonesia, Jakarta, Indonesia); X. Li (Cancer Hospital, Fudan University, Shanghai, China); and P. Wannakrairot and T. Intragumtornchai (Chulalongkorn University, Bangkok, Thailand).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Approval for this study was obtained from the Institutional Review Board at the University of Nebraska Medical Center and at each of the participating institutions as required by individual institutional policy. This study was conducted in accordance with the Declaration of Helsinki.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Perry, A.M., Diebold, J., Nathwani, B.N. et al. Non-Hodgkin lymphoma in the Far East: review of 730 cases from the international non-Hodgkin lymphoma classification project. Ann Hematol 95, 245–251 (2016). https://doi.org/10.1007/s00277-015-2543-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-015-2543-4