
Abstract
Background and purpose
The nasal base muscles are of great functional importance in health and disease. Particularly, the one lacking terminological consensus, but often termed as myrtiformis muscle, which has been mostly omitted by anatomists may have significance for rhinoplasty. The purpose of the current study was to re-examine the anatomical features of myrtiformis muscle.
Materials and methods
Conducted on 40 sides of 20 formalin-fixed amputated heads, we followed a dissection routine to fully expose the origin and insertion sites of the nasal base muscles. We measured the respective morphometric via digital caliper.
Results
Based on the number of bellies and their muscular attachment sites, we described an anatomical classification that consists of three different types of MM which had a single and broad origin. We classified the double-bellied muscle as Type 1 occurred in 10% (4/40), whereas the single-bellied ones as Types 2 and 3, occurred in 80% (32/40) and 10% (4/40), respectively. Measured distance between the medial margin of myrtiformis muscle origin and midline passing through the anterior nasal spine did not differ between any statistical comparisons (P > 0.05).
Conclusion
We revisited the muscle which was at some occasions termed as myrtiformis muscle, depressor septi nasi or depressor alae nasi muscles. Considering that there are differential forms of the muscle with the same muscular origin but bearing single or double bellies and/or different insertion sites, our classification may overcome possible terminological confusion by ensuring single muscle term with easily distinguishable morphological types. We invite anatomists to enlarge the data set and comment on our classification, and surgeons to conduct prospective examinations to add deeper insight regarding the functional importance of anatomical classifications by correlating pre vs post-operative functional differences.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Muscular dynamics of the nose is crucial to the phonation, facial expression and breathing [1, 4, 5]. Therefore, proper acknowledging of the anatomy and functions of nasal muscles is a prerequisite for planning any rhinoplasty. In particular, since nasal base muscles have major responsibility for controlling the tip of the nose and depressing the nostrils, interventions to those muscles have direct outcomes in rhinoplasty [2, 3, 11, 15]. Understanding the anatomy of the myrtiformis muscle is particularly relevant in cleft rhinoplasty, careful reconstruction of nasolabial muscular integrity being required to correct the deformity of the lower lateral cartilage in cleft patients [14].
Interestingly, such functionally important region still does not have unity at anatomical and nomenclature levels regarding its muscles [3, 8, 11, 13]. Depressor septi nasi, depressor alae nasi and myrtiformis are the terms used at different sources to describe an individual muscle or a part of the muscle at the region [3, 11]. Whether each aforementioned describing term qualifies an individual muscle or are they representing variations of a particular muscle is still debatable.
Gray made the first muscle description at the nasal base and termed it as depressor alae nasi [9]. Almost two decades later, Philibert Constant Sappey, a French surgeon and anatomist, described a fan-shaped muscle at the nasal base and proposed the term as myrtiformis [12]. Morphology of myrtiformis muscle (MM) was elaborately described in the original report by Sappey in French language. With a simplified classical definition, MM originates from the fossa termed as myrtiformis on maxilla, just above the lateral incisor and canine teeth, has an inner (medial) and an outer (lateral) part, which extend to the mobile subseptum and surround the nasal base, and functionally regarded as depressor septi nasi and depressor alae nasi [12]. Based on the current knowledge, whether the muscle that Sappey described was the same or entirely different to what Gray defined is still not clear [9, 12].
As emphasized by Figalo and Acosta and repointed by Daniel et al., MM was sequentially defined and omitted by respective anatomists throughout many decades [3, 8, 10, 13]. A relatively recent systematic review, covering many anatomical and surgical studies, stated that there was a divergence with regard to the anatomical nomenclature and muscle characteristics, referring to depressor septi nasi muscle (DSNM) [13]. Intriguingly, this review paper did not mention about the depressor alae nasi muscle (DANM) or MM [13].
In the current study, we carefully examined the anatomy of the lower nasal region to help clarifying the anatomical features of muscular structures, which were named as DSNM and/or DANM in some sources and as parts of the MM in the others [3, 7, 8, 13]). Lastly, morphometric of the muscles of nasal base was underrepresented by the previous anatomical studies. Therefore, we also provided a simple morphometric data set.
Materials and methods
This study was conducted on 40 sides of 20 formalin-fixed amputated heads belonged to the female (n = 10) and male (n = 10) cadavers (mean age with standard deviation; 71.6 ± 13.59) exempt of external pathology or anomaly that were in the inventory of Anatomy Department of Mersin University, Faculty of Medicine. The use of formalin-fixed amputated heads from the archive of the Anatomy Department for the current study was approved by Mersin University, Ethics Board of Clinical Research (Approval Decision Number: 25.08.2021-581). This study conforms to recognized standards of Helsinki Declaration. All the dissections were performed under a surgical microscope (Carl Zeiss f 170) and photographed with a digital camera.
The dissection routine for each cadaver was as follows; after the upper lip skin was removed, a deep incision was made on the orbicularis oris muscle (OOM) and the fascia above it, by making a parallel incision to the base of the nose. The MM was identified and the overlying structures and surrounding tissue were gently cleared. The origin and insertion locations of the MM were exposed (Fig. 1). The distance from the medial margin of MM origin in the maxilla to the midline passing through the anterior border of nasal base was measured by using a digital caliper with ± 0.01 mm precision. All measurements were blindly repeated in duplicates by two investigators (Uzmansel D and Öztürk NC). Average standard deviation was used for descriptive statistics of all the parameters used.

Removing the skin of the upper lip (a), dissecting and pulling down the superficial part of OOM attached to the nasal wings and septum along with the superficial fascia parallel to the nasal base are shown (b). MM (shown via asterisk) and the medial margin of MM origin to the midline (shown via dashed line) passing through anterior nasal spine was demonstrated (c)
Statistical analyses
Statistical analyses were performed with the free trial version of IBM SPSS Statistics 26 software. Initially, the normality data were tested using Shapiro–Wilk Test. Independent-Samples T Test was performed to analyze the distance of the origin of this muscle to the midline passing through the anterior nasal spine and the same morphometric between female and male subjects.
Results
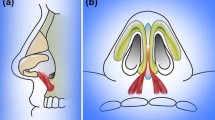
We observed that all the MM entities among our dissections were originated from the central, lateral incisors in the maxilla, the alveolar ridges of the canines and the pits on the ridges and the upper lip mucosa. Based on our morphological evaluations, we detected three distinguishable MM types. We observed two-bellied MM among the 10% of the cases (4/40). Occurred in two cadavers bilaterally, medial belly was inserted to the nasal floor and septum, whereas the lateral belly to the nasal floor only (Fig. 2a). Rest of the MM cases were appeared as single bellied (36/40). Based on the differences in the insertion site, we classified single-bellied cases into two different types (Type 2 and Type 3). In Type 2, large portion of the muscle was inserted to the nasal base and a small portion was attached the septum (32/40) (Fig. 2b). Observed in two heads bilaterally, in Type 3, MM was attached to the septum, nasal base and nasal wing (4/40) (Fig. 2). In all the Type 3 cases, we observed continuation of the lateral fibers with the nasal muscles (Fig. 2c). MM classifications shown in (Fig. 2) representing Types 1–3 were illustrated respectively (Fig. 3a–c). We also detected a modiolus-like structure formed by OOM and levator muscles of the upper lip (Fig. 4).

Types of myrtiformis muscle. Type 1: extending from the maxilla to the base of the nose (red) and from the base of the nose to the septum (blue), with lateral and medial bellies (a), Type 2: extending from the maxilla to the base of the nose and septum (b), Type 3: extending from the maxilla to the septum, nasal base and wings, in continuity with the nasal muscles (c). MM myrtiformis muscle, NM nasal muscles (color figure online)

Illustration: MM classifications shown in Fig. 2 representing Types 1–3, were exhibited, respectively (a–c)

Myrtiformis muscle, the modiolus-like structure, indicated via blue triangle (a) and rectangle (b) on the dissection, by OOM and upper lip levator muscles were shown. Muscle transitions between OOM and MM (blue rectangle) was represented (c). MM myrtiformis muscle, OOM orbicularis oris muscle, deep labial part, LM levator muscles of the upper lip (color figure online)
We presented the measured distance (in mm) between the medial margin of MM origin and the midline passing through the anterior nasal spine as mean ± standard deviation (Table 1). Based on the Shapiro–Wilk Test significance (P > 0.05), the normality was not violated. Using Independent-Samples T Test, we found no significant difference of the measured distance (P > 0.05), among the right and left sides or between the female and male subjects.
Discussion
The original definition of the MM defines two bellies or parts, the first and medial part is the belly that extends to the nasal septum and by referring to high likely functions, termed as depressor septi nasi, and the second, laterally, as depressor alae nasi [12]. Whilst, some researchers called the corresponding structures as DSNM or DANM rather than the bellies of the MM [11]. There are conflictions whether these muscles with septal and alar attachments are the variations of the same muscle, for example variations of MM, or are MM, DSNM and DANM independent muscles. Besides, if MM is an individual muscle, then does it coexist with other depressor muscles at the nasal base?
Based on our dissections, we detected a wide muscle origin at the nasal base, covering central and lateral incisors in the maxilla, the alveolar ridges of the canines and the pits on the ridges, as well as the upper lip mucosa. We were able to trace either single (Type 2 or Type 3) or double (Type 1) bellies extending towards the insertion sites form this large origin. Detecting a single origin covering a wide attachment site rather than two or more narrow muscle origins was the first rationale for us to assess the structure as MM. Aside the MM, we did not notice any other muscle at the nasal base.
In this sense, there was only one study to report that DSNM was a distinct entity and separate from MM or vice versa. But when evaluating this paper in detail, we thought there was still a little confusion to our understanding. Daniel et al. claimed that DSNM and MM were independent muscles. However, our finding of single and broad muscular origin in the nasal base is discordant with what Daniel et al. found as two separate muscle origins [3]. On the other hand, from an alternative perspective, one can consider that two muscle bellies of the MM were the DSNM and DANM, respectively. Also, in Type 2, the larger portion that was inserted to the nasal base can be considered as the DANM and the small portion that was attached to the septum as the DSNM.
We assume that morphological classifications of the nasal base muscles may help to clarify such confusions at the anatomical level. To the best of our knowledge, there were only two anatomical classification studies for the respective nasal base muscles [6, 11]. Conducted on 55 fresh cadavers, Rohrich et al. defined three morphological classifications of DSNM [11]. They classified a fully visible interdigitation with OOM from the origin at the medial crural foot plate in Type 1, while having little or no interdigitation with OOM in Type 2 (22%) [11]. Rohrich et al. reported no or only a visible rudimentary, DSNM in 16% of the cases (Type 3). In contrast to Type 1 by Rohrich et al., Daniel et al. reported only 1 case that was originating from OOM among 15 freshly dissected cadavers [3]. They claimed that this single case originating from OOM was an error of dissection [3]. By referring to Rohrich’s Type 3, Daniel et al. mentioned that they did not observe any rudimentary or absence of DSNM in their study [3]. Intriguingly, Rohrich et al. did not mention about MM, while Daniel et al. emphasized on MM [3, 11]. Whether Rohrich et al. (2000) did not observe any other nasal base muscle rather than DSNM corresponding to DANM or MM, or whether they detected but omitted those cases because the focus of their study was DSNM, were not stated in their paper.
Our observations pointed out a single muscle with a broad origin showing three distinct morphology based on the number of bellies and insertion sites what we prefer to call MM rather than DSNM. In some sources, DSNM is considered as a part of MM. From this angle, if we were to compare Rohrich’s morphological descriptions with our assessments, considering that we did not observe any interdigitation with OOM, their most frequent Type 1 is far from our classifications [11]. Fiber continuity rather than an interdigitation from origin of MM to OOM in a cadaver (bilaterally), may be the closest similarity to Rohrich's definition of DSNM with our cases.
On the other hand, based on the Sappey’s description, MM had two bellies [12]. But this information overlaps only 10% with our evaluations (Type 1). Despite sharing the common muscle origin similar to the double-bellied Type 1, we observed 90% (36/40) of the cases (Type 2 and Type 3) as single bellied. Most of those single-bellied cases were attached to the nasal base and less frequently to the septum (Type 2, %80). Although Type 2 and Type 3 MM were both single bellied, unlike Type 2, the distal attachment site of Type 3 was much larger and extended laterally to the nasal wing and continued upward with other nasal muscles. Rohrich et al. thoroughly discussed the anatomical relevancy of DSNM to identify the abnormalities during preoperational phase and to the outcomes of rhinoplasty [11]. Briefly, the surgical importance of depressor nasal muscle/s were first enlightened via “overactive depressor septi muscle” description by Wright and followed by other descriptions such as “rhino-gingivolabial syndrome of the smile” by Cachay-Velasquez [2, 15]. A decent example to the surgical importance of MM was particularly seen in cleft rhinoplasty, careful reconstruction of nasolabial muscular integrity being required to correct the deformity of the lower lateral cartilage in cleft patients [14].
Considering their insertion sites, Type 1 and Type 2 of our classification possibly delineate the functions of drawing the ala of nose downwards hence increasing the size of the nostril. But what about the possible function/s of Type 3 of MM which inserted to the septum, nasal base and nasal wing and continuing upward with the nasal muscles? Given its attachment to the nasal wing and continuing upward with nasal muscles aside the nasal septum base and wing; most obvious question regarding Type 3 MM is whether it contributes as a dilator of the nose during deep breathing similar to the alar part of the nasal muscle or oppositely, to nasal depression or construction. Another question is that what is the clinical relevance of two bellies (Type 1) versus one (Types 2, 3)? Do both belly active at the same time? Such questions could be best deciphered by correlating the pre vs. post-operational functional differences with delicate identification of anatomical muscle variations that were exposed during the surgeries. Prospective awareness of the anatomical classifications of MM prior to the surgical procedures may add deeper insights to the functional understanding of this muscle.
When we were planning the current study, we realized that the existed literature involving the muscles of the nasal base were devoid of morphometric data. Therefore, we designated a simple course, the distance from the midline (passing through the anterior nasal spine) to the medial margin of the muscle, which can be instructive for planning the rhinoplasty surgeries. The measurement of this course can be useful when assessing the force line to estimate the functional outcomes of the surgery.
We predict that a solid anatomical classification manifested with anatomical studies may be beneficial to understand the structures in the region which might be important during various surgical techniques, especially rhinoplasty.
Data availability
Data will be made available on request.
References
Berson ML (1963) Atlas of plastic surgery. Grune and Stratton, New York
Cachay-Velásquez H (1992) Rhinoplasty and facial expression. Ann Plast Surg 28(5):427–433. https://doi.org/10.1097/00000637-199205000-00006
Daniel RK, Glasz T, Molnar G, Palhazi P, Saban Y, Journel B (2013) The lower nasal base: an anatomical study. Aesthetic Surg J 33(2):222–232. https://doi.org/10.1177/1090820X12472695
Diamond HP (1971) Rhinoplasty technique. Surg Clin North Am 51:317–331. https://doi.org/10.1016/s0039-6109(16)39379-3
Dufourmentel C, Mouly R (1959) Chirurgie Plastique. Medicales Flammarion, Paris, p 637
Ebrahimi A, Nejadsarvari N, Motamedi MH, Rezaee M, Koushki ES (2012) Anatomic variations found on dissection of depressor septi nasi muscles in cadavers. Arch Facial Plast Surg 14(1):31–33. https://doi.org/10.1001/archfacial.2011.1216
Figallo EE (1995) The nasal tip: a new dynamic structure. Plast Reconstr Surg 95:1178–1184. https://doi.org/10.1097/00006534-199506000-00006
Figallo EE, Acosta JA (2001) Nose muscular dynamics: the tip trigonum. Plast Reconstr Surg 108:1118–1126. https://doi.org/10.1097/00006534-200110000-00003
Gray H (1858) Anatomy. Descriptive and Surgical, Parker JW, London
Gray H (1901) Anatomy. Bounty Books, New York, Descriptive and Surgical
Rohrich RJ, Huynh B, Muzaffar AR, Adams WP Jr, Robinson JB Jr (2000) Importance of the depressor septi nasi muscle in rhinoplasty: anatomic study and clinical application. Plast Reconstr Surg 105(1):376–83. https://doi.org/10.1097/00006534-200001000-00059
Sappey PC (1876) Traitè d anatomie descriptive, Tome 2, 3rd edn. A Delahaye, Paris, pp 135–142
Sinno S, Chang JB, Saadeh PB, Lee MR (2015) Anatomy and surgical treatment of the depressor septi nasi muscle: a systematic review. Plast Reconstr Surg 135(5):838e–848e. https://doi.org/10.1097/PRS.0000000000001169
Talmant JC (1993) Nasal malformations associated with unilateral cleft lip accurate diagnosis and management. Scand J Plast Reconstr Surg Hand Surg 27(3):183–191. https://doi.org/10.3109/02844319309078110
Wright WK (1976) Symposium: the supra-tip in rhinoplasty: a dilemma II Influence of surrounding structure and prevention. The Laryngoscope 86(1):50–52. https://doi.org/10.1288/00005537-197601000-00010
Acknowledgements
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. The results of such studies can contribute to the improvement of the health service that humanity receives. For this reason, we would like to express our gratitude to these donors and their families on behalf of researchers and humanity
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
UD collected data and prepared the figures. ÖNC analyzed the data. Both authors wrote the main manuscript and reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
The anatomical proposal of this study was approved by Mersin University, Ethics Board of Clinical Research (Approval Decision Number: 25.08.2021-581). This study conforms to recognized standards of Helsinki Declaration.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Uzmansel, D., Öztürk, N.C. Revisiting the anatomy of myrtiformis muscle. Surg Radiol Anat 45, 789–794 (2023). https://doi.org/10.1007/s00276-023-03154-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-023-03154-3