
Abstract
Purpose
The purpose of the present study was to analyze the dimensions of the crista galli (CG) in preserved skulls, and to examine the role of the morphometry and morphology of the CG on the sex estimation.
Methods
Anteroposterior, superoinferior, and laterolateral diameters of the CG were measured of 207 preserved adult skulls of Anatolia origin with known sex (108 males, 99 females) in the Anatolian population. CG were morphologically classified into three types according to the dimensions. The success of CG dimensions in sex determination was evaluated with ROC analysis, and univariate and multivariate binary logistic regression analysis. The relationship between morphological types of the CG and sex was analyzed with the Chi-square test.
Results
The anteroposterior and superoinferior diameters of the CG significantly were longer in males than females while the laterolateral diameter of the CG was wider in females (p < 0.001). Superoposterior diameter (88.4%) of the CG showed higher sex classification accuracy for sex estimation compared to the laterolateral (82.6%) and anteroposterior diameters (80.6%). When all three parameters were used together, the sex classification accuracy rate was 94.2%. The presence of ossified and tubular types of CG identified the male sex with 85% and 74.6% accuracy rates, respectively while teardrop type CG identified female sex with a 72.2% accuracy rate.
Conclusion
CG exhibits sexual dimorphism both morphometrically and morphologically. The height, length, and width measurements and the morphological types of CG can be used in sex determination directly from the skull with high accuracy rates.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Personal identification is one of the most challenging aspects of forensic science. Determination of the sex from unidentified skeletal remains is a fundamental step in creating a biological profile of an individual in both forensic anthropology and bioarcheology [25]. Accurate sex prediction is important for the accurate determination of other biological characteristics such as race, age, and stature [20].
Skeletal characteristics specific to different populations make population-specific analyses necessary for sex determination. The pelvis and the skull are regarded as the most useful anatomical structures in the human skeleton for sex estimation [3, 19]. As the skull has more preserved integrity than the pelvis, which tends to be found more fragmented, it is a reliable indicator for sex determination when the pelvis is unavailable [9, 17, 24]. Differences in shape and size underlie the dimorphic features of the skull [12]. As it is resistant to varying environmental conditions, the skull retains dimorphic characteristics relatively better than other bones. Therefore, to date, various approaches have been described for sex determination based on the morphometrical and morphological characteristics of the skull [17, 19].
The skull may not always be found complete or intact. Sex determination is more difficult from skull fragments brought for forensic examination. Therefore, for accurate and reliable identification it is extremely important that methods are developed and confirmed which examine smaller fragments of the skeleton [2, 7]. The inner surface of the skull and the anatomic structures enclosed within it are more protected, making them less vulnerable to various destructive forces. Therefore, sex determination performed using anatomic structures on the inner surface of the skull may be useful in identity determination from remains which have been greatly destroyed.
The crista galli (CG), upward bony protrusion of the ethmoid bone, is a pyramidal shaped structure located in the anterior cranial fossa. The morphological characteristics of the CG, which is a compact bony structure or sometimes pneumatized, show variability from individual to individual. This study was carried out to examine dimensions of the CG in preserved adult skulls and to classify morphologically the CG according to unbiased morphometric criteria, and analyze the role of the dimensions and types of the CG in sex estimation.
Materials and methods
This study was approved by the Ethics Committee of Hitit University. The study was performed on a total of 207 (108 males, 99 females) adult preserved skulls of Anatolia origin unknown age that were obtained from the Departments of Anatomy of Hitit University and Akdeniz University. Pediatric skulls and those with pathology, deformation, or fracture in the ethmoid bone were excluded from the study. Morphometric and morphological examinations of the CG were performed by an investigator who was experienced in osteometric studies.
Morphometric measurements and morphological classification of the CG
Maximum anteroposterior, maximum superoinferior, and maximum laterolateral diameters of the CG were measured using digital calipers (Figs. 1, 2, 3). The morphological classification of the CG was based on the methodology proposed by Komut and Golpinar [8].

Measurement of the superoinferior diameter of the CG on the adult skull. The red dotted lines indicate superior and inferior borders of the CG

Measurement of the laterolateral diameter of the CG on the adult skull. The red dotted lines indicate lateral borders of the CG

Measurement of the anteroposterior diameter of the CG on the adult skull. The red dotted lines indicate the anterior and posterior borders of the CG
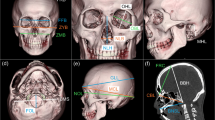
In this study, the CG was classified as teardrop type, tubular type, or ossified type, according to the dimensions of the CG and the presence of a cavitary component of the CG on CT images (Fig. 4). Accordingly, CGs with a width more than a third greater than its height and including a broad cavitary component was classified as teardrop type (Fig. 5A, D). CGs with a width less than one-third of its height and containing a cavitary component from the base to the apex were categorized as tubular type (Fig. 5B, E). CGs with a width less than a third of its height but not including a cavitary component were classified as ossified type (Fig. 5C, F).

Schematic drawing of the morphological classification of the CG: A teardrop type, B tubular type, C ossified type

Superior view of an adult skull. Morphological classification of the CG on the adult skull: A teardrop type, B tubular type, and C ossified type. Latero-posterior view of an adult skull. Morphological classification of the CG on the adult skull: D teardrop type, E tubular type, and F ossified type
Statistical analysis
Statistical analysis of data was performed using SPSS version 22.0 software (SPSS Inc., Chicago, IL, USA). Two independent groups of numerical variables were compared using the Student’s t-test or the Mann–Whitney U test according to the conformity of the variables to normal distribution. Comparison of categorical variables were performed using the χ2 test or Fisher’s exact test. The success classification rates in sex estimation of the morphological types and dimensions of the CG were assessed using receiver-operating characteristic (ROC) analysis. Optimal cutoff points of the three morphometric parameters of the CG were determined with the Youden Index (maximum sensitivity and specificity). The effect of the anteroposterior, superoinferior and laterolateral diameters of the CG on sex estimation was analyzed using univariate and multivariate binary logistic regression analysis.
Results
No statistically significant difference was determined between male (n = 108) and female skulls (n = 99) in respect of the number of samples (p = 0.482). The mean superoinferior, laterolateral, and anteroposterior diameters of the CG were 12.01 ± 2.31 mm, 3.70 ± 1.27 mm, and 15.15 ± 1.54 mm, respectively (Table 1). The comparisons of the CG dimensions between males and females are presented in Table 2. There were significant differences in dimensions of the CG between males and females (p < 0.001) (Fig. 6). ROC analysis findings indicating the classification success of the superoinferior, laterolateral, and anteroposterior diameters of the CG on sex estimation are presented in Table 3. In identifying the sex, the superoinferior and laterolateral diameters of the CG were found to be significant at an excellent level and the anteroposterior diameter of the CG at a good level (AUC = 0.937; p < 0.001, AUC = 0.920; p < 0.001, AUC = 0.888; p < 0.001, respectively).

Box plots for A superoinferior diameter, B laterolateral diameter, and C anteroposterior diameter measurements of CG regarding gender. Dotted lines on the graphs indicate the cutoff scores of the superoinferior diameter, laterolateral diameter, and anteroposterior diameter measurements of the CG
The cutoff point for the superoinferior diameter of the CG was found to be 11.81 mm, and this point indicated 84.8% sensitivity for distinguishing male sex and 91.6% specificity for distinguishing female sex. The cutoff point of the laterolateral diameter of the CG was 3.11 mm, and this point indicated 90.9% sensitivity for distinguishing male sex and 75% specificity for distinguishing female sex. The cutoff point of the anteroposterior diameter of the CG was identified as 15.79 mm, and this point had 95.9% sensitivity for distinguishing male sex and 66.6% specificity for distinguishing female sex (Table 3). The ROC curves representing the classification success of the superoinferior, laterolateral, and anteroposterior diameters measurements of the CG in sex determination are shown in Fig. 7. The predictive power of the obtained cutoff points in distinguishing male and female sex are presented in Table 4.

ROC curves showing the predictive power of A superoinferior diameter, B laterolateral diameter, and C anteroposterior diameter measurements of CG in sex determination
The distribution of the CG types regarding sex are presented in Table 5. Of the total samples, 108 (52.2%) were teardrop type CG, 59 (28.5%) were tubular type CG, and 40 (19.3%) were ossified type CG. A significant relationship between all CG types and sex was observed (p < 0.001). The findings of the univariate and multivariate binary logistic regression analysis showing the effect of the CG morphometry on sex estimation are presented in Table 6. In the multivariate logistic regression model, the odds ratios determined for the superoinferior, laterolateral, and anteroposterior diameters of CG were 48.47, 42.59, and 31.83, respectively.
Discussion
Sex estimation from human skeletal structures is one of the essential steps for identification procedures in forensic medicine [14]. The skull is accepted as the second best indicator of sex after the pelvis [21]. The CG, which is a projecting part of the ethmoid bone extending upwards, is the most prominent anatomical structure in the anterior cranial fossa.
There is a limited number of studies which have examined CG morphometry, and the findings in those studies of the relationship between sex and the morphometric characteristics of CG have been conflicting. Mladina et al. examined cone beam computed tomography (CBCT) scans of 102 dry skulls (76 males, 26 females) and found that the superoinferior diameter of CG was significantly longer in females (14.2 mm) than in males (9.5 mm), whereas there was no difference between the genders in respect of the laterolateral (2.8 mm vs. 3.1 mm) and anteroposterior diameters (7.4 mm vs. 7.5 mm) of pneumatized CG [11]. Manea and Mladina investigated the morphometric characteristics of the pneumatized CG from the paranasal CT images of 196 subjects. No significant difference was found between males (5.3–13.8 mm and 5.1–12.7 mm, respectively) and females (5.0–12.4 mm and 4.7–11.2 mm, respectively) in respect of the length and height of the CG while the CG was determined to be significantly wider in males (3.3–6.8 mm) than females (3.0–5.7 mm) [10]. In a study evaluating the CBCT scans of 300 healthy subjects, Uçar et al. reported no significant differences between the sexes in respect of the mean anteroposterior (14.05 ± 2.98 mm vs 14.02 ± 2.90 mm) and laterolateral diameters (3.69 ± 1.53 mm and 3.77 ± 1.43 mm) of the CG [22]. Komut and Golpinar investigated the relationship between CG dimensions and sex from the paranasal CT images of 533 individuals (266 males, 267 females) and found that the CG showed sexual dimorphism in terms of its dimensions [8]. According to the findings of that study, the height (16.28 mm vs. 12.17 mm) and length (14.50 mm vs. 11.06 mm) of the CG were significantly higher in males compared to females while the width (2.59 mm vs. 4.55 mm) of the CG was significantly lower in males than in females. In the current study, the potential relationship between CG dimensions and sex was tested directly from adult dry skulls. The results of the study showed that the CG was sexually dimorphic in terms of dimensions. In the present study, similar to the findings of the study by Komut and Golpinar, the CG was significantly higher (13.64 mm vs. 10.24 mm) and longer (16.10 mm vs. 14.12 mm) in males, while in females it was significantly wider (4.64 mm vs. 2.84 mm) (p < 0.001) [8]. Differences between our findings and findings of previous CT-based studies might have arisen from measurement protocols. This situation is clearer in the height measurement of CG. The base of the CG can be found at the level or sometimes below the cribriform plate. Therefore, radiological measurement of the CG height provides more realistic results than the method used in the present study when the CG continues under the cribriform plate.
In the study by Komut and Golpinar, the sex classification accuracy rates of the superoinferior, laterolateral, and anteroposterior diameters of the CG were 81.4%, 81.2%, and 83.7%, respectively and when all diameter measurements of the CG were taken into consideration, the sex classification accuracy rate was 88.6% [8]. Similarly, in the current study, the CG dimensions showed high classification accuracy rates for sex estimation. According to the ROC analysis results, the classification accuracy rates of the CG dimensions in sex determination were 88.4% for the height parameter, 82.6% for the width parameter, and 80.6% for the length parameter. When the three parameters were used together, the sex classification accuracy rate was 94.2%. Unlike the study performed by Komut and Golpinar, in the current study, the height parameter of the CG had higher classification success in sex estimation than the width and length parameters of the CG [8].
Previously published studies have reported that sex estimation can be performed using various anatomical structures or landmarks in the skull. In a study which examined 101 skulls of the Thai population, Sangvichien et al. reported that sex could be identified with an 88.8% accuracy rate when using the nasion–basion length, maximum breadth of the cranium, facial length, and bizygomatic breadth of the face [18]. Uthman et al. examined the relationship between sex and maxillary sinus dimensions on 88 CT images (45 males, 48 females) and found that maxillary sinus height was the best measurement for sex estimation with a 71.6% accuracy rate [23]. In another study, in which the relationship of the mandibular ramus with sex was examined on 100 orthopantomographs, the accuracy rate of the mandibular ramus measurements was determined to be 76% [6]. In a study which examined the role of the glabella, mastoid process, and occipital protuberance in sex determination in 165 dry skulls of the Greek population, when the three anatomical landmarks were used the accuracy rates were found to be 86.3–94.1% for males and 83.9–93.5% for females [13]. As mentioned above, the skull has important anatomical structures that exhibit sexual dimorphism such as the maxillary sinus, mandibular ramus, mastoid process, and occipital protuberance. Each anatomical structure has its own morphometric or morphological properties that could be used in sex determination. However, these structures could show different degrees of sexual dimorphism and some of them are more vulnerable to various destructive forces. In addition, measurement protocol is not practical for sex estimation when various reference points are used. Therefore, the anatomical structures which show both morphometrically and morphologically sexual dimorphism and are more protected from destructive forces may provide more reliable and accurate data on the identification of the gender.
According to ROC analysis results of the current study, the morphometric cutoff points of the CG in sex estimation were found to be 11.81 mm, 3.11 mm, and 15.79 mm, respectively for height, width, and length parameters. When the cutoff values were taken into consideration, the height parameter of the CG could predict female sex with an accuracy rate of 91.6%, and the width and length parameters could predict male sex with accuracy rates of 90.9% and 95.9%, respectively. When the dry skull samples were assessed in terms of height of the CG > 11.81 mm, width of the CG < 3.11 mm, and length of the CG > 15.79 mm, respectively, 99, 81, and 77 of the total 108 male dry skulls, respectively, could be correctly predicted. When the dry skull samples were assessed in terms of height of the CG ≤ 11.81 mm, width of the CG ≥ 3.11 mm, and length of the CG ≤ 15.79 mm, 84, 90, and 95 of the total 99 female dry skulls, respectively, could be correctly predicted. Although the cutoff points of the CG height, width, and length could predict both male and female sex with high classification accuracy, these cutoff points showed more successful classification in identifying males compared to females. According to the results of the logistic regression analysis, the probability of female sex was 61.6-fold greater in skulls with CG height ≤ 11.81 mm compared to CG height > 11.81 mm. The probability of female sex was 30-fold greater in skulls with CG width ≥ 3.11 mm compared to CG width < 3.11 mm. The probability of female sex was 47.50-fold greater in skulls with CG length ≤ 15.79 mm compared to CG length > 15.79 mm.
There are two main approaches in sex estimation from bone structures, the osteometric and osteomorphological approaches. Although each approach has its own specific benefits when used separately, as they complement each other, much higher accuracy rates are obtained when they are used in combination for sex estimation [16]. In the present study, the relationship of morphological characteristics of the CG with sex was also evaluated in addition to the CG morphometric characteristics. The CGs were classified into three morphological types as teardrop type, tubular type, or ossified type using objective morphometric criteria. The morphological approach in this study is based on objective morphometric criteria, providing high accuracy rates in sex determination, by reducing the error rates in the morphological classification of the CG.
According to the findings of this study, the CG also shows morphologically sexual dimorphism. The presence of ossified and tubular types of CG could identify male sex at the accuracy rates of 85% and 74.6%, respectively. The presence of teardrop type CG could identify female sex at an accuracy rate of 72.2%. Similarly, in the study by Komut and Golpinar, teardrop type CG was the most common type of CG in females at the rate of 82.9% [8]. In males, the most dominant CG type was the ossified type with a rate of 88.7%, followed by the tubular type with a rate of 65.8%. The proposed classification of the CG in the current study provides high classification rates in sex determination, similar to the craniometric methods developed for different anatomical structures in current literature [1, 4, 5, and15]. The limitation of this study was that the age of the study samples was not known. Future examinations of the CG morphometric and morphological properties in dry skull samples of known age will be important in respect of determining the relationship not only with sex but also with age.
Conclusion
In conclusion, this is the first study to have demonstrated the relationship between sex and the morphometric and morphological characteristics of the CG in adult preserved skulls. CG shows sexual dimorphism both morphometrically and morphologically. The CG was significantly higher and longer in males while significantly wider in females. Height, width, and length measurements of the CG are reliable discriminant parameters that could be used for sex estimation. Based on objective morphometric criteria, the CGs in the preserved skulls were classified morphologically. Teardrop type CG was the most common type of CG in females. In males, the most dominant CG type was the ossified type, followed by the tubular type. In addition to the height, length, and width parameters, the morphological types of the CG can be used for sex determination directly from the skull with high rates of accuracy.
References
Abdel Fatah EE, Shirley NR, Jantz RL, Mahfouz MR (2014) Improving sex estimation from crania using a novel three-dimensional quantitative method. J Forensic Sci 59:590–600. https://doi.org/10.1111/1556-4029.12379
Akhlaghi M, Bakhtavar K, Moarefdoost J, Kamali A, Rafeifar S (2016) Frontal sinus parameters in computed tomography and sex determination. Leg Med (Tokyo) 19:22–27. https://doi.org/10.1016/j.legalmed.2016.01.008
d’Oliveira Coelho J, Curate F (2019) Cadoes: an interactive machine-learning approach for sex estimation with the pelvis. Forensic Sci Int 302:109873. https://doi.org/10.1016/j.forsciint.2019.109873
Franklin D, Cardini A, Flavel A, Kuliukas A (2013) Estimation of sex from cranial measurements in a Western Australian population. Forensic Sci Int 229(158):158.e1–158.e8. https://doi.org/10.1016/j.forsciint.2013.03.005
González-Colmenares G, Sanabria Medina C, Rojas-Sánchez MP, León K, Malpud A (2019) Sex estimation from skull base radiographs in a contemporary Colombian population. J Forensic Leg Med 62:77–81. https://doi.org/10.1016/j.jflm.2019.01.006
Indira AP, Markande A, David MP (2012) Mandibular ramus: an indicator for sex determination—a digital radiographic study. J Forensic Dent Sci 4:58–62. https://doi.org/10.4103/0975-1475.109885
Iscan MY, Steyn M (2013) The human skeleton in forensic medicine. Charles C Thomas Publisher, Springfield
Komut E, Golpinar M (2021) A comprehensive morphometric analysis of crista galli for sex determination with a novel morphological classification on computed tomography images. Surg Radiol Anat 43:1989–1998. https://doi.org/10.1007/s00276-021-02799-2
Kranioti EF, Işcan MY, Michalodimitrakis M (2008) Craniometric analysis of the modern Cretan population. Forensic Sci Int 180(2–3):110.e1-110.e1105. https://doi.org/10.1016/j.forsciint.2008.06.018
Manea C, Mladina R (2016) Crista galli sinusitis—a radiological impression or a real clinical entity. Rom J Rhinol 23:167–117. https://doi.org/10.1515/rjr-2016-0019
Mladina R, Antunović R, Cingi C, Muluk NB, Skitarelić N, Malić M (2017) An anatomical study of pneumatized crista galli. Neurosurg Rev 40:671–678. https://doi.org/10.1007/s10143-017-0825-0
Nagaoka T, Shizushima A, Sawada J, Tomo S, Hoshino K, Sato H, Hirata K (2008) Sex determination using mastoid process measurements: standards for Japanese human skeletons of the medieval and early modern periods. Anthropol Sci 116:105–113. https://doi.org/10.1537/ase.07060513
Nikita E, Michopoulou E (2018) A quantitative approach for sex estimation based on cranial morphology. Am J Phys Anthropol 165:507–517. https://doi.org/10.1002/ajpa.23376
Paknahad M, Shahidi S, Zarei Z (2017) Sexual dimorphism of maxillary sinus dimensions using cone-beam computed tomography. J Forensic Sci 62:395–398. https://doi.org/10.1111/1556-4029.13272
Ramamoorthy B, Pai MM, Prabhu LV, Muralimanju BV, Rai R (2016) Assessment of craniometric traits in South Indian dry skulls for sex determination. J Forensic Leg Med 37:8–14. https://doi.org/10.1016/j.jflm.2015.10.001
Robinson MS, Bidmos MA (2009) The skull and humerus in the determination of sex: reliability of discriminant function equations. Forensic Sci Int 186(86):86.e1–86.e5. https://doi.org/10.1016/j.forsciint.2009.01.003
Rösing FW, Graw M, Marré B, Ritz-Timme S, Rothschild MA, Rötzscher K, Schmeling A, Schröder I, Geserick G (2007) Recommendations for the forensic diagnosis of sex and age from skeletons. Homo 58:75–89. https://doi.org/10.1016/j.jchb.2005.07.00218
Sangvichien S, Boonkaew K, Chuncharunee A, Komoltri C, Piyawinitwong S, Wongsawut A, Namwongsa S (2007) Sex determination in Thai skulls by using craniometry: multiple logistic regression analysis. Siriraj Med J 59:216–221
Sinhorini PA, Costa IAP, Lopez-Capp TT, Biazevic MGH, de Paiva LAS (2019) Comparative analysis of four morphometric methods for sex estimation: a study conducted on human skulls. Leg Med (Tokyo) 39:29–34. https://doi.org/10.1016/j.legalmed.2019.06.001
Spradley MK (2016) Metric methods for the biological profile in forensic anthropology: sex, ancestry, and stature. Acad Forensic Pathol 6:391–399. https://doi.org/10.23907/2016.040
Spradley MK, Jantz RL (2011) Sex estimation in forensic anthropology: skull versus postcranial elements. J Forensic Sci 56:289–296. https://doi.org/10.1111/j.1556-4029.2010.01635.x
Uçar H, Bahsi I, Orhan M, Yalçin ED (2021) The radiological evaluation of the crista galli and its clinical implications for anterior skull base surgery. J Craniofac Surg 32:1928–1930. https://doi.org/10.1097/SCS.0000000000007507
Uthman AT, Al-Rawi NH, Al-Naaimi AS, Al-Timimi JF (2011) Evaluation of maxillary sinus dimensions in gender determination using helical CT scanning. J Forensic Sci 56:403–408. https://doi.org/10.1111/j.1556-4029.2010.01642.x
Waldron T (1987) The relative survival of the human skeleton: implications for palaeopathology. Death, decay and reconstruction: approaches to archaeology and forensic science:55–64
Yang W, Liu X, Wang K, Hu J, Geng G, Feng J (2019) Sex determination of three-dimensional skull based on improved backpropagation neural network. Comput Math Methods Med 2019:9163547. https://doi.org/10.1155/2019/9163547
Funding
No funding was received from any source for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest was reported by the author(s).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Golpinar, M., Salim, H., Ozturk, S. et al. Sex estimation with morphometric and morphological characteristics of the crista galli. Surg Radiol Anat 44, 1007–1015 (2022). https://doi.org/10.1007/s00276-022-02971-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-022-02971-2