
Abstract
We present an extremely rare case of an aberrant course of the precavernous–cavernous junction of the internal carotid artery (ICA), which was observed by magnetic resonance (MR) angiography. The patient was a 67-year-old woman with no symptoms related to the anomalous ICA. The anomalous segment of the ICA was stenotic and formed a loop postero-supero-laterally. We found no similar cases in the relevant English-language literature. Segmental agenesis of the ICA with collateral formation, probably via the proximal segment of the primitive trigeminal artery, may be associated with the development of this variation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An aberrant course of the internal carotid artery (ICA) in the petrous bone is a rare but well-known arterial variation. It is diagnosed radiologically by a lateralized course, presence in the middle ear cavity, and absence of the vertical segment of the petrous ICA [1,2,3]. We herein present a case in which the ICA showed an aberrant course in the precavernous–cavernous junction, which was detected by magnetic resonance (MR) angiography. To our knowledge, no similar cases have been reported in the relevant English-language literature.
Case report
A 67-year-old woman with chronic renal failure visited the neurosurgical department of a general hospital complaining of myoclonus. The results of a neurological examination were normal. Cranial computed tomography without contrast media showed no abnormalities, however, cerebral MR imaging and MR angiography were subsequently performed using a 1.5 T scanner. MR angiography was performed with a standard 3-dimensional time-of-flight (3D-TOF) technique.
MR imaging showed nonspecific small white matter lesions. MR angiography showed an aberrant course of the left ICA in the precavernous–cavernous junction, with stenosis at the segment that was abnormally located postero-supero-laterally (Fig. 1). The A1 segment of the left anterior cerebral artery (ACA) was hypoplastic, and the left posterior communicating artery (PCoA) was absent. Thus, only the left middle cerebral artery (MCA) was supplied by the left ICA.

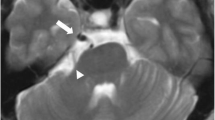
source image of MR angiography show a narrow and postero-laterally located affected segment of the left ICA (arrow)
Magnetic resonance (MR) angiography obtained using a 1.5-T scanner. a, b Left lateral and left anterior oblique projections of MR angiograms show a tortuous and narrow precavernous–cavernous junction of the left internal carotid artery (ICA). The anomalous segment takes a postero-supero-lateral course (arrows). c An anteroinferior–posterosuperior projection of MR angiography shows the absence of the left A1 segment of the left anterior cerebral artery (arrow). The left posterior communicating artery is also absent. d A
Because there were no symptoms of ICA stenosis, she was treated conservatively. The clinical course was uneventful.
Discussion
An aberrant course of the petrous ICA is a rare but clinically significant arterial variation that may cause objective pulsatile tinnitus, hearing loss, otalgia, and aural fullness [4, 5]. Although incidentally found cases are not rare, it is dangerous during middle ear surgery, because it runs in the middle ear cavity [6]. Lasjaunias et al. [2] hypothesized that the genesis of an aberrant ICA as an alternate flow of blood, in which involution of the cervical ICA—due to the persistence of the pharyngeal artery system—leads to blood flowing via the ascending pharyngeal artery to the enlarged inferior tympanic artery with retrograde flow through the caroticotympanic vessels into the horizontal segment of the petrous ICA. This theory may explain the radiological features.
In our patient, the aberrant course was seen at the precavernous–cavernous junction of the ICA. Therefore, a different etiology may have been present. A persistent trigeminal artery (PTA) frequently arises from the affected segment [7]. A PTA arising from the arterial ring of the cavernous ICA is a known variation [8]. We hypothesized that segmental agenesis of the precavernous–cavernous junction of the ICA with collateral circulation via the proximal segment of the PTA may lead to the formation of this segmentally dysplastic ICA. This new type of aberrant ICA has no clinical significance itself; however, the stenotic segment seems to have a high risk of occlusion.
The A1 segment of the ipsilateral ACA is usually absent or hypoplastic when the petrous ICA shows an aberrant course [1, 3, 9]. The reduced diameter of the aberrant ICA may cause blood flow to decrease in the ICA. Thus, the aberrant ICA only supplies the MCA, and the contralateral A1 segment of the ACA is the main supply of the ipsilateral A2 segment of the ACA via the anterior communicating artery (ACoA). Our patient had similar findings. If the ipsilateral A1 segment is absent, there is no cross flow to the MCA from the contralateral ICA via the ACoA when the stenotic aberrant ICA is occluded. In our patient, because the ipsilateral PCoA is also absent, there is no cross flow to the MCA from the vertebrobasilar system.
The ICA also takes an aberrant course at the cervical segment, coursing medially and reaching the midline of the oropharynx submucosa [10]. Because it mimics a retropharyngeal mass during physical examinations, it should be correctly diagnosed before any surgical procedure in the oropharynx.
Conclusions
In the present case, an aberrant course of the precavernous–cavernous junction of the ICA was incidentally diagnosed. This variation has not previously been reported. Segmental agenesis of the ICA with collateral circulation, to which the proximal segment of the PTA probably contributed, may cause the formation of this rare variation.
References
Celebi I, Oz A, Yildirim H, Bankeroglu H, Basak M (2012) A case of an aberrant internal carotid artery with a persistent stapedial artery: association of hypoplasia of the A1 segment of the anterior cerebral artery. Surg Radiol Anat 34:665–670
Lasjaunias P, Moret J, Manelfe C, Theron J, Hasso T, Seeger J (1977) Arterial anomalies at the base of the skull. Neuroradiology 13:267–272
Uchino A, Saito N, Okano N, Kakehi Y (2015) Aberrant internal carotid artery associated with occipital artery arising from the internal carotid artery. Surg Radiol Anat 37:1137–1140
Endo K, Maruyama Y, Tsukatani T, Furukawa M (2006) Aberrant internal carotid artery as a cause of objective pulsatile tinnitus. Auris Nasus Larynx 33:447–450
Song YS, Yuan YY, Wang GJ, Dai P, Han DY (2012) Aberrant internal carotid artery causing objective pulsatile tinnitus and conductive hearing loss. Acta Otolaryngol 132:1126–1130
Sauvaget E, Paris J, Kici S, Kania R, Guichard JP, Chapot R, Thomassin JM, Herman P, Tran Ba Huy P (2006) Aberrant internal carotid artery in the temporal bone: imaging findings and management. Arch Otolaryngol Head Neck Surg 132:86–91
Uchino A, Saito N, Okada Y, Kozawa E, Mizukoshi W, Inoue K, Takahashi M (2012) Persistent trigeminal artery and its variants on MR angiography. Surg Radiol Anat 34:271–276
Uchino A, Saito N, Kurita H, Ishihara S (2012) Persistent trigeminal artery arising from the arterial ring/fenestration of the cavernous segment of the internal carotid artery. Surg Radiol Anat 34:651–654
Shimizu S, Sasahara G, Iida Y, Shibuya M, Numata T (2009) Aberrant internal carotid artery in the middle ear with a deficiency in the origin of the anterior cerebral artery: a case report. Auris Nasus Larynx 36:359–362
Srinivasan S, Ali SZ, Chwan LT (2013) Aberrant retropharyngeal (submucosal) internal carotid artery: an under-recognized, clinically significant variant. Surg Radiol Anat 35:449–450
Author information
Authors and Affiliations
Contributions
AU carried out the study design and drafted the manuscript. All authors reviewed the manuscript critically, and have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
We declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Uchino, A., Kimura, H. Aberrant course of the precavernous–cavernous junction of the internal carotid artery. Surg Radiol Anat 43, 1979–1981 (2021). https://doi.org/10.1007/s00276-021-02839-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-021-02839-x