
Abstract
Background
Several anatomical studies regarding the value of hip rotation center (HRC) and femoral offset (FO) have been performed in Western populations. However, there are a few data on hip morphological values in the Chinese population based on CT scans. This study measured the values of the hip and pelvis, especially HRC and FO, in a Chinese population and compared them with the published values obtained from Western populations.
Patients and methods
One hundred patients (50 females and 50 males) were included in the present study, and 3D-CT reconstructions of the hip and pelvis were generated. The mean age was 51.4 ± 8.9 years and mean body mass index (BMI) was 23.5 ± 2.6 kg/m2. All the morphologic measurements were compared between genders and sides, and the relationships between different parameters were analyzed.
Results
The mean FO values were 38.4 ± 4.7 mm and 35.6 ± 4.4 mm for the males and females, respectively. A significant negative correlation was noted between FO and neck shaft angle (NSA) in both genders (r = − 0.262, P = 0.009 for the males, r = − 0.350, P ≤ 0.001 for the females). A significant positive correlation was found between horizontal distance (HD) and diameter of the femoral head (DFH) in both genders (r = 0.734, P ≤ 0.001 for the males, r = 0.658, P ≤ 0.001 for the females). A significant positive correlation was noted between HD and pelvic width (PW) in males (r = 0.455, P ≤ 0.001). A significant positive correlation was also noted between HD and pelvic height (PH) in males (r = 0.318, P ≤ 0.001). A significant positive correlation was observed between FO and pelvic cavity height (PCH) in males (r = 0.411, P ≤ 0.001), and a significant positive correlation was observed between VD and PCH in females (r = 0.497, P ≤ 0.001). The tip of the greater trochanter was, on average, 7.0 mm higher than the femoral head center. Relationships between DFH and pelvic morphometric parameters were also observed.
Conclusion
The present morphological data and the relationships between them can be applied to design better ethnic-specific THA prostheses and preoperative plans.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The accurate restoration of the hip joint during total hip arthroplasty (THA) results in the improvement of abductor muscle strength [3, 13, 22] and reduced risk of post-operative complications such as dislocation, limp, and wear-related implant failure [5, 17, 29, 31]. During THA, hip rotation center (HRC) and femoral offset (FO) [5, 6, 18, 22, 31] are important factors, which exert a strong effect on clinical outcomes. Although a standardized positioning protocol is used, the method for obtaining the X-ray radiographs has a potential bias, for both femoral rotation and positioning of the calibration marker depend on the judgment of the technician. Moreover, limitations of the 2D characteristics of radiographs include errors resulting from magnification [7] and inaccurate patient position [25, 28, 34]. In contrast, the morphology can be well assessed using CT scans independent of the position of the patient and eliminating the magnification by post-processing techniques. CT can also evaluate many planes in detail with high accuracy [1].
The values of HRC and FO have been well illustrated in Western populations, yet a few studies have focused on these morphological parameters in the Chinese population based on CT scans. As bone geometry differs between regions and races [4, 24, 35], it is necessary to perform an anatomical study of the HRC and FO in a Chinese population based on 3D-CT reconstruction for better ethnic-specific THA prostheses and preoperative plans.
Patients and methods
In accordance with the ethical standards of the 1964 Declaration of Helsinki, the study was approved by the local ethics committee. Inclusion criteria included patients who underwent pelvic CT scanning for reasons unrelated to symptoms of the hip. Exclusion criteria included patients who had neurological, functional, or morphological disorders affecting gait. All images were reviewed by a senior surgeon (ZX) and a radiologist (RL), confirming the absence of proximal femoral or hip deformity. Finally, 100 randomly selected patients (50 females and 50 males) scanned between June 2016 and September 2017 were retrospectively reviewed. Their mean age was 51.4 ± 8.9 years (range 29–67), and mean body mass index (BMI) was 23.5 ± 2.6 kg/m2 (range 19.5–29.3). Patients were positioned supine, with their legs in neutral rotation and were scanned in a body region including the pelvis from the iliac crest proximally to the femoral isthmus distally using an iCT256 scanner (Philips, Holland) with 0.625 mm CT slices at 300 mA and 120 kV. All measurements were performed on the Philips IntelliSpace Portal after three-dimensional reconstruction.
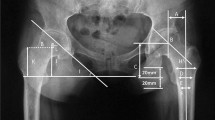
With the help of circles and related view ports superimposed on the femoral head, the best-fitting circle was used to determine the HRC in coronal and horizontal planes. We measured the HRC and FO in the coronal plane in accordance with Taichiro’s method [33] but based on 3D-CT reconstruction in a transparent model (Fig. 1).

To depict the teardrop, the image was reconstructed with the help of the coronal transparent hip model. FO femoral offset, HD horizontal distance, VD vertical distance, TH trochanteric height, NSA neck shaft angle
The parameters were defined as follows:
FO: femoral offset, length of the perpendicular line between HRC and the femoral axis [18]. HD: horizontal distance, length of the perpendicular line between HRC and the vertical line across the inferior edge of the teardrop center. VD: vertical distance, length of the perpendicular line between HRC and the line tangent to the inferior edge of the teardrop center. TH: trochanteric height, the height of the greater trochanter relative to the HRC [14]. DFH: diameter of the femoral head. NSA: neck shaft angle.
In addition, we evaluated the pelvic morphometric parameters shown in Fig. 2. In the coronal plane, the bone window and the transparent model were used to reconstruct the pelvis.

Pelvic morphometric parameters. a, b Coronal 3D pelvis model in the bone window. c Coronal transparent 3D pelvis model. PH pelvic height, PW pelvic width, PCW pelvic cavity width, PCH pelvic cavity height, BWLA body weight lever arm, ITD inter-teardrop distance, IHT ilium height from teardrop edge
Pelvic morphometric parameters:
PH: pelvic height.
PW: pelvic width.
PCW: pelvic cavity width.
PCH: pelvic cavity height.
BWLA: body weight lever arm.
ITD: Inter-teardrop distance.
IHT: ilium height from teardrop edge.
Statistical method
A single-measure intraclass correlation coefficient (ICC) was used for the quantification of inter- and intra-observer reliability of the measurements. Measurements were performed by two observers (LHY and XZ) two times each, with a minimum interval of 4 weeks, for ten specimens. Values greater than 0.80 indicated satisfactory reliability. The two-sample t test was used to compare the differences between genders. The paired Student’s t test was used to compare the differences between sides. Pearson’s correlation was used to assess the relationship between linear variables. The variability of sensitivity and specificity estimates was expressed in 95% exact confidence intervals. Statistical analysis was performed using SPSS version 19.0 (SPSS Inc. Chicago), and significance was defined as P < 0.05.
Results
Intraclass correlation coefficients of intra-observer repeat measurements ranged from 0.93 to 0.99, and the intraclass correlation coefficients of interobserver repeat measurements ranged from 0.91 to 0.99. All correlations were statistically significant, and the level of measurement reliability was excellent.
Morphometric parameters of the series are summarized in Table 1. For the parameters of the hip, the mean values of FO, HD, DFH, and TH of the males were larger than those of the females (P < 0.05). The mean values of VD, BWLA, and NSA of the males were similar to those of the females. There was no significant difference between the left and right sides for any of these values (P > 0.05). For the parameters of the pelvis, the mean values of PH and IHT of the males were larger than those of the females (P < 0.05). However, the mean values of PCH and ITD of the males were lower than those of the females (P < 0.05). The mean values of PW and PCW of the male were similar to those of the females.
The key relationships between measures are detailed in Figs. 3, 4, 5, 6, and 7. Figure 3a, b shows the relationship between FO and NSA in males (r = − 0.262, P = 0.009 and FO = 64.71 − 0.21 × NSA) and females (r = − 0.350, P ≤ 0.001 and FO = 71.39 − 0.28 × NSA), respectively. Figure 4a, b shows the relationship between HD and DFH in males (r = 0.734, P ≤ 0.001 and HD=-3.04 + 0.75 × DFH) and females (r = 0.658, P ≤ 0.001 and HD = − 4.31 + 0.79 × DFH), respectively. Figure 5a, b shows the relationships between HD and PW (r = 0.455, P ≤ 0.001 and HD = 12.2 + 0.08 × PW) and between HD and PH (r = 0.318, P ≤ 0.001 and HD = 13.97 + 0.1 × PH) in males. Figure 6 shows the relationship between FO and PCH (r = 0.411, P ≤ 0.001 and FO = 24.23 + 0.24 × PCH) in males. Figure 7 shows the relationship between VD and PCH (r = 0.497, P ≤ 0.001 and VD = 3.19 + 0.13 × PCH) in females.

Correlations between FO and NSA in Chinese males (a) and females (b). Significant negative correlations were noted between FO and NSA in both genders (r = − 0.262, P = 0.009, and FO = 64.71 − 0.21 × NSA for the males; r = − 0.350, P ≤ 0.001, and FO = 71.39 − 0.28 × NSA for the females)

Correlations between HD and DFH in Chinese males (a) and females (b). Significant positive correlations were noted between HD and DFH in both genders (r = 0.734, P ≤ 0.001, and HD = − 3.04 + 0.75 × DFH for the males; r = 0.658, P ≤ 0.001, and HD = − 4.31 + 0.79 × DFH for the females)

Correlations between HD and PW (a) and between HD and PH (b) in Chinese males. Significant positives correlation were noted between HD and PW (r = 0.455, P ≤ 0.001, and HD = 12.2 + 0.08 × PW) and between HD and PH (r = 0.318, P ≤ 0.001, and HD = 13.97 + 0.1 × PH)

Correlation between FO and PCH in Chinese males. A significant positive correlation was observed between FO and PCH (r = 0.411, P ≤ 0.001, and FO = 24.23 + 0.24 × PCH)

Correlation between VD and PCH in Chinese females. A significant positive correlation was observed between VD and PCH (r = 0.497, P ≤ 0.001, and VD = 3.19 + 0.13 × PCH)
Relationships between DFH and pelvic morphometric parameters, DFH, and body height were also observed. Regression equations of the parameters are summarized in Table 2.
In addition, the overall mean value of the ratio between DFH and PH was 0.229 (0.197–0.262, 95% CI 0.227–0.231). The mean ratios between DFH and PH were 0.235 (0.211–0.262) and 0.223 (0.197–0.243) in the males and the females, respectively.
Discussion
Most previous studies related to hip morphology have concentrated on plain radiographs. In planning total hip replacement, the conventional radiography measurements are still the most convenient method. However, poor reproducibility can result from the positioning of the patients and the imaging conditions [16], such as film-focus distance and X-ray incident angle. Usually, femoral offset (FO) is measured on plain radiographs. However, due to the femoral anteversion and external rotation, the real offset corresponds to the projection on the frontal view in a two-dimensional (2-D) plane [28, 32], leading to measurement error to some extent. The morphology can be well assessed using CT scans regardless of the position of the patient using post-processing techniques. CT can also evaluate different planes in detail with high accuracy by thin-slice reconstruction. Recently, Sariali et al. [32] reported that the femoral offset might be underestimated by up to 13.7 mm when measured on plain radiographs rather than with a 3D-CT scan, leading to functional impairment. In a previous study [20], Ma et al. measured a series of 35 morphometric parameters on CT images of the acetabulum in a Chinese population, but the lack of the transparent model to show the teardrop led to a failure to measure HRC and FO.
Uncorrected restoration of FO has been associated with increased joint reactive force and, therefore, increased polyethylene wear [9, 31]. Little et al. [19] found that an increase in FO beyond 5 mm of the contralateral hip might result in increased polyethylene wear. Asayama et al. [3] reported that optimally reconstructed hip function could be achieved through normal or slightly increased FO with restoration of the HRC at near-normal or slightly inferomedial to normal position. Clement et al. [6] demonstrated that medialization of the acetabular prostheses with increased FO resulted in improved functional outcome. Cassidy et al. [5] reported that decreased FO led to decreased function at 1-year follow-up. A recent study [10] suggested that hip offset (FO + HD) should be well reconstructed in patients with primary HOA or mild developmental dysplasia of the hip (DDH), as it demonstrated an additive effect on clinical outcome. However, their study failed to evaluate the relationships between HRC and clinical outcomes. Meanwhile, a study [12] focused on displaced femoral neck fracture suggested that restoring the original FO had clinical relevance to the functional outcome, even in bipolar hemiarthroplasty.
In the present study, significant negative correlations were observed between FO and NSA in both genders (r = − 0.262, P = 0.009 and FO = 64.71 − 0.21 × NSA for the males, r = − 0.350, P ≤ 0.001 and FO = 71.39 − 0.28 × NSA for the females). In the males, a significant positive correlation was also observed between FO and PCH (r = 0.437, P ≤ 0.001 and FO = 23.51 + 0.25PCH). To our knowledge, this is the first study to describe a regression equation for FO. A significant negative correlation was found between FO and NSA, which should be considered when designing femoral stem prostheses.
Various data and regression formulae for determining HRC have been reported based on radiographic analyses. For HD, Taichiro et al. [33] reported the equations of HD = 12.657 + 0.083 × PW for the males and HD = 5.521 + 0.091 × PW for the females. Pierchon et al. [30] found relationships of HD = 0.3 × PH in the males and HD = 0.25 × PCH in the females, and HD = 0.2 × ITD in the males and HD = 0.18 × ITD in the females. In the present study, we found formulae of HD = 12.2 + 0.08 × PW, HD = 13.97 + 0.1 × PH and HD = −3.04 + 0.75DFH (for the males) and HD = − 4.31 + 0.79DFH (for the females). Taichiro et al. and the present study found similar positive correlations between HD and PW in the males. For VD, Taichiro et al. [33] reported an equation of VD = 9.692 + 0.098 × PCH in Japanese females. In contrast, we found VD = 3.19 + 0.13PCH in the females.
For hip morphology in relation to FO and HRC, most previous reports mentioned above suggested that FO should be reconstructed in normal or slightly increased OA patients. The mean FO values were 38.4 ± 4.7 and 35.6 ± 4.4 mm for the males and the females, respectively. The FO values in our study were close to the data reported by Taichiro et al. [33] (36.0 ± 5.8 and 33.4 ± 4.9 mm for Japanese males and females). However, the mean FO values in Western populations were significantly different from those of the Chinese: they were reported as 43.0 ± 6.8 mm [27], 42.6 mm (ranging from 26.9 to 53.9 mm) [17], 44.7 mm [23], and 42.2 ± 5.1 mm [32]. Acetabular cup position has a significant impact on THA, which affects the dislocation rate, gait, range of motion (ROM), limb length, abductor muscle strength, wear, loosening, and cup failure [2, 15, 26]. Individualized depth and height of the cup placement are based on achieving optimum cup fixation. Choosing a medialized position in a person with large native offset should be done carefully, for medialization, can result in medial movement of HRC up to 14 mm [21]. In the present study, the males had the parameters of HD = 34.4 ± 3.1 and VD = 12.9 ± 2.9 mm, and the females had parameters of HD = 30.5 ± 2.6 and VD = 12.2 ± 2.9 mm. Zhang et al. [37] reported that Western bone size was significantly larger than Chinese without adjusting for any covariates; however, after adjusting for height, age, and weight, hip bone size was larger in the Chinese compared to Westerners. A recent study [11] compared three different cementless stem designs in patients with primary HOA, demonstrating that multiple shape and offset options allowed for a better metaphyseal stem fit and offered minor clinical advantages for leg length reconstruction. Therefore, racial discrepancies of hip morphology should be carefully considered when choosing the best-fitted prostheses in THA.
Severe primary hip osteoarthritis or secondary hip osteoarthritis might cause the collapse of the femoral head, resulting in failure to measure the real diameter of the femoral head (DFH). With regard to the strong relationships between DFH and pelvic parameters and between DFH and height (Table 2), the regression equation might provide us a reference to measure the DFH. Crowe et al. [8] measured 50 normal hips in a Western population but failed to report specific measurement data. Zhang et al. [36] reported that the overall mean ratio between DFH and PH was 0.215 based on X-ray measurements in a Chinese population. In present study, the overall mean ratio between DFH and PH was 0.229. Our results also suggest that Chinese surgeons could effectively use the Crowe classification to classify patients with hip dysplasia.
The tip of the greater trochanter was, on average, 7.0 mm higher than that of the femoral head center, but the common misconception is that these two points are on the same perpendicular line to the femur axis in the normal population. Sariali et al. [32] reported that the trochanteric height (TH) value was 9.5 mm based on 3D-CT scans. Krishnan et al [14] reported that the TH value was 8 mm. Thus, we should be cautious when using the TH as a height reference, to avoid limb lengthening in THA.
There were certain limitations to the current study. First, our sample size may not be sufficient to represent the general Chinese population. Second, there are only normal Chinese population data about the hip and pelvis. Therefore, a cross-sectional study of asymptomatic individuals of multiple races with the use of 3D-CT scans will be necessary. The main goal of this study was to provide morphological data and the correlations between them at the time of hip arthroplasty to contribute to better ethnic-specific THA prostheses and preoperative plans. Since the body type of Japanese and Koreans is similar to those of Chinese, the results of this study may be a reference for patients from those countries, as well.
References
Abel MF, Sutherland DH, Wenger DR et al (1994) Evaluation of CT scans and 3-D reformatted images for quantitative assessment of the hip. J Pediatr Orthop 14:48–53
Abolghasemian M, Samiezadeh S, Jafari D et al (2013) Displacement of the hip center of rotation after arthroplasty of Crowe III and IV dysplasia: a radiological and biomechanical study. J Arthroplasty 28:1031–1035
Asayama I, Chamnongkich S, Simpson KJ et al (2005) Reconstructed hip joint position and abductor muscle strength after total hip arthroplasty. J Arthroplasty 20:414–420
Blum MA, Ibrahim SA (2012) Race/ethnicity and use of elective joint replacement in the management of end-stage knee/hip osteoarthritis: a review of the literature. Clin Geriatr Med 28:521–532
Cassidy KA, Noticewala MS, Macaulay W et al (2012) Effect of femoral offset on pain and function after total hip arthroplasty. J Arthroplasty 27:1863–1869
Clement ND, Macdonald SP-PR D et al (2016) Total hip replacement: increasing femoral offset improves functional outcome. Arch Orthop Trauma Surg 136:1317–1323
Conn KS, Clarke MT, Hallett JP (2002) A simple guide to determine the magnification of radiographs and to improve the accuracy of preoperative templating. J Bone Jt Surg Br 84:269–272
Crowe JF, Mani VJ, Ranawat CS (1979) Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Jt Surg Am 61:15–23
Devane PA, Horne JG (1999) Assessment of polyethylene wear in total hip replacement. Clin Orthop Relat Res 369:59–72
Innmann MM, Maier MW, Streit MR et al (2018) Additive influence of hip offset and leg length reconstruction on postoperative improvement in clinical outcome after total hip arthroplasty. J Arthroplasty 33:156–161
Innmann MM, Spier K, Streit MR et al (2017) Comparative analysis of the reconstruction of individual hip anatomy using three different cementless stem designs in patients with primary hip osteoarthritis. J Arthroplasty 33:1126–1132
Ji HM, Won SH, Han J et al (2017) Does femoral offset recover and affect the functional outcome of patients with displaced femoral neck fracture following hemiarthroplasty? Injury 48:1170–1174
Kiyama T, Naito M, Shitama H et al (2009) Effect of superior placement of the hip center on abductor muscle strength in total hip arthroplasty. J Arthroplasty 24:240–245
Krishnan SP, Carrington RWJ, Mohiyaddin S et al (2006) Common misconceptions of normal hip joint relations on pelvic radiographs. J Arthroplasty 21:409–412
Kurtz WB, Ecker TM, Reichmann WM et al (2010) Factors affecting bony impingement in hip arthroplasty. J Arthroplasty 25:624–634
Larson AN, Rabenhorst B, Rocha ADL et al (2012) Limited intraobserver and interobserver reliability for the common measures of hip joint congruency used in dysplasia. Clin Orthop Relat Res 470:1414–1420
Lecerf G, Fessy MH, Philippot R et al (2009) Femoral offset: Anatomical concept, definition, assessment, implications for preoperative templating and hip arthroplasty. Orthop Traumatol Surg Res 95:210–219
Liebs TR, Nasser L, Herzberg W et al (2014) The influence of femoral offset on health-related quality of life after total hip replacement. Bone Jt J 96-B(1):36–42
Little NJ, Busch CA, Gallagher JA et al (2009) Acetabular polyethylene wear and acetabular inclination and femoral offset. Clin Orthop Relat Res 467:2895–2900
Ma H, Han Y, Yang Q et al (2014) Three-dimensional computed tomography reconstruction measurements of acetabulum in Chinese adults. Anat Rec (Hoboken) 297:643–649
Maratt JD, Esposito CI, Mclawhorn AS et al (2015) Pelvic tilt in patients undergoing total hip arthroplasty: when does it matter? J Arthroplasty 30:387–391
Mcgrory BJ, Morrey BF, Cahalan TD et al (1995) Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Jt Surg Br 77:865–869
Merle C, Waldstein W, Pegg E et al (2012) Femoral offset is underestimated on anteroposterior radiographs of the pelvis but accurately assessed on anteroposterior radiographs of the hip. J Bone Jt Surg Br 94:477–482
Mikhail MB, Vaswani AN, Aloia JF (1996) Racial differences in femoral dimensions and their relation to hip fracture. Osteoporos Int 6:22–24
Mineta K, Goto T, Wada K et al (2016) CT-based morphological assessment of the hip joint in Japanese patients: association with radiographic predictors of femoroacetabular impingement. Bone Jt J 98-B:1167–1174
Ng VY, Kean JR, Glassman AH (2013) Limb-length discrepancy after hip arthroplasty. J Bone Jt Surg Am 95:1426–1436
Noble PC, Alexander JW, Lindahl LJ et al (1988) The anatomic basis of femoral component design. Clin Orthop Relat Res 235:148–165
Pasquier G, Ducharne G, Ali ES et al (2010) Total hip arthroplasty offset measurement: Is C T scan the most accurate option? Orthop Traumatol Surg Res 96:367–375
Patel AB, Wagle RR, Usrey MM et al (2010) Guidelines for implant placement to minimize impingement during activities of daily living after total hip arthroplasty. J Arthroplasty 25:1275–1281
Pierchon F, Migaud H, Duquennoy A et al (1993) Radiologic evaluation of the rotation center of the hip. Rev Chir Orthop Reparatrice Appar Mot 79:281–284
Sakalkale DP, Sharkey PF, Eng K et al (2001) Effect of femoral component offset on polyethylene wear in total hip arthroplasty. Clin Orthop Relat Res 388:125–134
Sariali E, Mouttet A, Pasquier G et al (2009) Three-dimensional hip anatomy in osteoarthritis. Analysis of the femoral offset. J Arthroplasty 24:990–997
Takamatsu T, Shishido T, Takahashi Y et al (2015) Radiographic determination of hip rotation center and femoral offset in japanese adults: a preliminary investigation toward the preoperative implications in total hip arthroplasty. Biomed Res Int 2015:610763
Varghese B, Muthukumar N, Balasubramaniam M et al (2011) Reliability of measurements with digital radiographs—a myth. Acta Orthop Belg 77:622–625
Warden SJ, Hill KM, Ferira AJ et al (2013) Racial differences in cortical bone and their relationship to biochemical variables in Black and White children in the early stages of puberty. Osteoporos Int 24:1869–1879
Zhang Y, Jiang J, Wang C et al (2014) The ratio of femoral head diameter to pelvic height in the normal hips of a Chinese population. Eur J Orthop Surg Traumatol 24:947–951
Zhang YY, Liu PY, Lu Y et al (2010) Race and sex differences and contribution of height: a study on bone size in healthy Caucasians and Chinese. Am J Hum Biol 17:568–575
Acknowledgements
This work has received the financial support from the National Natural Science Foundation of China (81672184), Key Program of Science and Technique Development Foundation in Jiangsu Province (BE2015627), Research Project of Jiangsu Provincial Health Department (H201528), China Postdoctoral Science Foundation Funded Project (2016M591929, 2017T100408), and Jiangsu Provincial Medical Youth Talent (QNRC2016801).
Author information
Authors and Affiliations
Contributions
KJG and XZ: protocol development. LHY, XZ, and RL: data collection. ZYZ, JLT, and CWB: data analysis. LHY and FCZ: manuscript writing.
Corresponding authors
Ethics declarations
Conflict of interest
The author declares that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Yi, Lh., Li, R., Zhu, Zy. et al. Anatomical study based on 3D-CT image reconstruction of the hip rotation center and femoral offset in a Chinese population: preoperative implications in total hip arthroplasty. Surg Radiol Anat 41, 117–124 (2019). https://doi.org/10.1007/s00276-018-2143-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-018-2143-9