
Abstract
Persistent trigeminal artery (PTA) and its variant (PTAV) are the most prevalent types of carotid-vertebrobasilar anastomosis, but bilateral anastomoses are exceedingly rare. We report a case of a right PTAV and tiny left lateral-type PTA from which the cerebellar artery (presumed anterior inferior cerebellar artery) arose. And also, bilateral ophthalmic arteries arose from the cavernous segments of the internal carotid arteries and entered the orbits via the superior orbital fissures. Selective cerebral angiography, especially 3-dimensional angiography, is superior to magnetic resonance (MR) angiography to identify rare variations of the cerebral arteries. Careful observation of MR angiographic source images is important for identifying unique arterial coursing.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The term persistent trigeminal artery (PTA) describes anastomosis between the cavernous or precavernous segment of the internal carotid artery (ICA) and midportion of the basilar artery (BA), and PTA variant (PTAV) describes a cerebellar artery (usually the anterior inferior cerebellar artery, AICA) arising from the cavernous or precavernous ICA without communication with the BA. These are the most common types of carotid-vertebrobasilar anastomosis, with a reported prevalence of 0.20–0.68% [3, 4, 7, 10, 14]. Low spatial resolution on magnetic resonance (MR) angiography prevents visualization of some tiny PTAs and PTAVs.
Since Binet and Young first reported a case of bilateral PTAs in 1977 [5], several cases of bilateral PTAs, PTA and PTAV, and bilateral PTAVs have been reported [1, 2, 6, 8, 9, 12, 13].
We report a case of a right PTAV and tiny left lateral-type PTA from which a cerebellar artery (presumed AICA) arose. And also, the bilateral ophthalmic arteries (OAs) originated from the cavernous segments of the ICAs and entered the orbits via the superior orbital fissures instead of the optic canals.
Case report
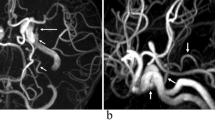
A 56-year-old woman with an incidentally discovered cerebral aneurysm was transferred to our institution from a private hospital for further evaluation and possible treatment. Selective cerebral angiography showed an aneurysm at the paraclinoid segment of the left ICA (Fig. 1) and a small artery arising on either side from the precavernous segment of the ICA. Typical coursing of an AICA by the artery on the right without communication with the BA indicated it was a PTAV. The proximal segment of the artery on the left took the same course as that on the right, but a distal segment of this artery was faintly identified. Careful observation of special projections of the left internal carotid angiography, including 3D images, revealed the tiny artery as a lateral-type PTA from which a small cerebellar artery (presumed AICA) arose ( Fig. 1c–f), and the bilateral OAs arose from the cavernous segments of the ICAs. The left vertebral angiography showed tiny right AICA and dominant type left AICA (Fig. 1g).

Selective catheter angiography before coiling of aneurysm. a Lateral projection of the right internal carotid angiography shows the right anterior inferior cerebellar artery (AICA) arising from the precavernous segment of the right internal carotid artery (ICA), indicative of a persistent trigeminal artery variant (PTAV) (long thick arrows). The right ophthalmic artery arises from the cavernous segment of the right ICA (long thin arrow). b Lateral projection of the left internal carotid angiography shows an aneurysm at the paraclinoid segment of the left ICA (long dotted arrow). A tiny artery arises from the precavernous segment of the left ICA, just as on the right side, but the peripheral portion is faintly visualized (short thick arrow). The left ophthalmic artery arises from the cavernous segment of the left ICA (short thin arrow). c–f Special projections of the left internal carotid angiography and its 3-dimensional image show that the small artery arising from the precavernous ICA is a persistent trigeminal artery (PTA), not a PTAV (short thick arrows and long thin arrows). Short thin arrows indicate tiny cerebellar branch (presumed AICA), and dotted arrows indicate basilar artery (BA). The BA is visualized momently (c, d). g Anteroposterior projection of the left vertebral angiography shows tiny right AICA and dominant type left AICA
The patient provided informed consent and underwent coiling of the unruptured aneurysm without complication. Two months after the treatment, she underwent follow-up MR imaging and MR angiography using a 3-Tesla scanner. MR angiography showed no residual aneurysm. Arterial variations previously detected by selective cerebral angiography were reconfirmed. However, the distal segment of the tiny left PTA was not identified clearly even on MR angiographic source images. The bilateral OAs originating from the cavernous ICAs ran laterally and entered the orbits via the superior orbital fissures instead of the optic canals (Fig. 2). Previous selective cerebral angiography did not detect this unique coursing of the bilateral OAs.

Magnetic resonance (MR) angiographic source image. a Slightly angled thick axial reformatted image shows that anomalous arteries arise from the precavernous segment of the bilateral internal carotid arteries (ICAs) and course posteriorly (long and short thick arrows). Bilateral ophthalmic arteries (OAs) arise from the cavernous segments of the ICAs and enter the orbits via the superior orbital fissures instead of the optic canals (long and short thin arrows). Dotted arrows indicate the bilateral optic canals. b Sagittal reformatted image of the left side shows that the origin of the left OA is the proximal siphon level, not supraclinoid/ophthalmic segment
Discussion
PTAs, including PTAVs, represent the most common type of carotid-vertebrobasilar anastomosis, with a reported prevalence of approximately 0.5% [3, 4, 7, 10, 14]. However, reports of bilateral PTAs [1, 2, 5, 6], PTA and PTAV [8, 9, 12], and bilateral PTAVs [13] are exceedingly rare. If bilateral PTAs or PTAVs occur independently during early gestation, their prevalence is estimated at about 0.0025%.
Traditionally, Saltzman [11] classified PTA according to the branching pattern of the posterior communicating artery (PCoA) and posterior cerebral artery, but O’uchi [10] doubts, and we agree, that this system of classification is useful, because the PCoA belongs to the supratentorial arteries, and the PTA is related to the arteries of the brainstem. Four types of PTA and PTAV have recently been classified according to the branching of the vessel from the PTA and the vessel’s course (Fig. 3): (1) lateral-type PTA (usual type); (2) medial-type PTA (so-called intrasellar type or trans-sphenoidal type); (3) PTAV (most are AICA type); and (4) lateral-type PTA from which the superior cerebellar artery arises [10, 14]. Our patient had a right PTAV and left lateral-type PTA from which the cerebellar artery (presumed AICA) arose. The small size of the cerebellar artery allowed its visualization only by selective cerebral angiography (Fig. 1c–f).

Schematic illustration of the four types of PTA and PTAV in infero-superior projection (Modified from Reference#14). 1 Right lateral-type PTA; 2 left medial-type PTA; 3 right PTAV, AICA type; 4 left lateral-type PTA from which the superior cerebellar artery arises; 5 bilateral ICAs
Cerebral arterial variations coexistent with PTA have been reported [4], but none resemble the case of our patient, with bilateral OAs originating from the cavernous ICAs and entering the orbits via the superior orbital fissures. One group reported a prevalence of such concurrent variations on MR angiography of 0.42% [15] and indicated right-side predominance, but they described no case of bilateral type. During early gestation, there are primitive dorsal and ventral OAs; the dorsal OA usually regresses and the ventral OA remains and forms a normal OA. If the situation is reversed and the ventral OA disappears and the dorsal OA remains, a persistent dorsal OA results [15]. The persistent vessel usually arises from the inferolateral trunk, a tiny branch of the cavernous segment of the ICA. Our patient demonstrated two extremely rare arterial variations simultaneously. Figure 4 shows a schematic illustration of the intracranial arterial system of our patient. The unique course of the bilateral OAs identified on MR angiographic source images (Fig. 2) could not be recognized on selective cerebral angiography.

Schematic illustration of the arterial variations of our patient in infero-superior projection. 1 Right persistent trigeminal artery variant (PTAV, anterior inferior cerebellar artery type); 2 left lateral-type PTA from which the cerebellar artery (presumed AICA) arises; 3 right ophthalmic artery (OA) arising from the cavernous segment of the internal carotid artery (ICA); 4 left OA arising from the cavernous segment of the ICA; 5 bilateral ICAs
Conclusions
We have presented selective cerebral angiographic images of a patient with a right PTAV, left lateral-type PTA from which a tiny cerebellar artery (presumed AICA) arose, and bilateral OAs arising from the cavernous ICAs. MR angiographic source images showed entry of the bilateral OAs into the orbits via the superior orbital fissures instead of the optic canals. Selective cerebral angiography is superior to MR angiography for the evaluation of tiny arteries. Careful evaluation of MR angiographic source images is important to confirm rare arterial variations including their unique arterial coursing.
References
Ali S, Walker MT (2007) Bilateral persistent trigeminal arteries associated with bilateral carotid aneurysms. J Vasc Interv Radiol 18:692–694
Alleyne CH Jr, Krisht A, Yoo FK, Silverstein A, Colohan AR (1997) Bilateral persistent trigeminal arteries associated with cerebral aneurysms and aortic arch vessel anomaly. South Med J 90:434–438
Arráez-Aybar LA, Fuentes-Redondo T, Millán JM (2016) Persistent trigeminal artery: a cross-sectional study based on over 3 years conventional angiography, CT angiography and MR angiography images. Surg Radiol Anat 38:445–453
Bai M, Guo Q, Li S (2013) Persistent trigeminal artery/persistent trigeminal artery variant and coexisting variants of the head and neck vessels diagnosed using 3 T MRA. Clin Radiol 68:e578–e585
Binet EF, Young RF (1977) Bilateral persistent trigeminal arteries. Case report. J Neurosurg 47:619–622
Chen D, Chen CJ, Chen JJ, Tseng YC, Hsu HL, Ku JW (2013) Bilateral persistent trigeminal arteries with unilateral trigeminal artery to cavernous sinus fistula. A case report. Interv Neuroradiol 19:339–343
Kim MJ, Kim MS (2015) Persistent primitive trigeminal artery: analysis of anatomical characteristics and clinical significances. Surg Radiol Anat 37:69–74
Meila D, Papke K, Schlunz-Hendann M, Mangold A, Jacobs C, Brassel F (2011) Bilateral persistent trigeminal arteries, one of them ending in the posterior inferior cerebellar artery: case report and review of the literature. Clin Neuroradiol 21:95–99
Okada Y, Shima T, Nishida M, Yamada T, Yamane K, Okita S, Kagawa R (1992) Bilateral persistent trigeminal arteries presenting with brain-stem infarction. Neuroradiology 34:283–286
O’uchi E, O’uchi T (2010) Persistent primitive trigeminal arteries (PTA) and its variant (PTAV): analysis of 103 cases detected in 16,415 cases of MRA over 3 years. Neuroradiology 52:1111–1119
Saltzman GF (1959) Patent primitive trigeminal artery studied by cerebral angiography. Acta Radiol 51:329–336
Son B, Yang S, Sung J, Lee S (2013) Bilateral persistent primitive trigeminal arteries associated with trigeminal neuralgia. Clin Neuroradiol 23:45–49
Uchino A (2011) Bilateral persistent trigeminal artery variants diagnosed by MR angiography. Cerebellum 10:745–747
Uchino A, Saito N, Okada Y, Kozawa E, Mizukoshi W, Inoue K, Takahashi M (2012) Persistent trigeminal artery and its variants on MR angiography. Surg Radiol Anat 34:271–276
Uchino A, Saito N, Takahashi M, Kozawa E, Mizukoshi W, Nakajima R, Okano N (2013) Persistent dorsal ophthalmic artery and ophthalmic artery arising from the middle meningeal artery diagnosed by MR angiography at 3 T. Surg Radiol Anat 35:775–782
Acknowledgements
We thank Rosalyn Uhrig, M.A., for editorial assistance in the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We declare that we have no conflict of interest.
Rights and permissions
About this article

Cite this article
Uchino, A., Neki, H. & Yamane, F. Right persistent trigeminal artery variant (PTAV) and tiny left PTA associated with bilateral ophthalmic arteries arising from the cavernous segments of the internal carotid arteries. Surg Radiol Anat 39, 1279–1283 (2017). https://doi.org/10.1007/s00276-017-1862-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-017-1862-7