
Abstract
Purpose
The aim of this study was to analyze the impact of calcification on the 12 and 24 months outcomes of the Eluvia™ (Boston Scientific®) drug-eluting stent (DES) for femoropopliteal occlusive disease using three different calcium scoring systems.
Material and Methods
A single-center, retrospective cohort-study (March-2016 to December-2018) of patients treated with the Eluvia™ DES for femoropopliteal atherosclerosis was performed. Outcomes included primary and secondary patency rates and freedom from target lesion revascularization (FTLR) and were analyzed by comparing the impact of calcium burden according to the following calcium scores: Peripheral Arterial Calcium Scoring System (PACSS) score, number of vessel quadrants affected (0–4) and calcification score per Peripheral Academic Research Consortium (PARC) definitions.
Results
In total, 111 Patients were included (mean age: 71.2 ± 7.9; 64% male). Most patients presented with Rutherford class 3 (79.9%), followed by class 5 (12.7%), class 4 (10%) and class 6 (6.4%). The mean lesion length was 197.6 ± 108.5 mm and 74.3% of patients had chronic total occlusions. There were no differences in primary patency between the calcification scores at 12 months (PACSS, LogRank = 0.28; quadrants, LogRank = 0.29; PARC, LogRank = 0.42) and 24 months (PACSS, LogRank = 0.13; quadrants, LogRank = 0.42; PARC, LogRank = 0.13). FTLR was significantly lower at 12 months in patients with calcification affecting 3 or 4 quadrants (LogRank = 0.022) but not at 24 months (LogRank = 0.36).
Conclusions
In this study, the Eluvia™ DES showed promising performance in calcified disease and the analysis according to the quadrant model predicted an increased risk for TLR at 12 months.
Graphical Abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Endovascular revascularization (ER) is indicated as primary option in most patients with peripheral artery disease [1,2,3]. However, the early benefits of endovascular treatment in terms of lower morbidity and mortality have been challenged by the lower patency rates in the long run [1, 2]. Drug-eluting technologies have been used to address this issue with paclitaxel being the most studied agent used to decrease the risk of restenosis [4, 5]. Although drug-coated balloons are usually preferred for more plain lesions, in more complex disease, drug-eluting stents (DES) have shown to perform better [1, 2]. The Eluvia™ (Boston Scientific®) DES, which has a polymer coating, has been shown to have promising results at 2 years in patients with complex femoropopliteal (FP) disease and compared favorably with other non-polymer coated DES and uncoated scaffolds [5, 6].
Arterial calcification has been increasingly recognized as an independent risk factor for loss of patency and clinical failure [7,8,9].Several scores have been developed to quantify the burden of calcium and predict its impact on revascularization outcomes [10, 11]. However, there is a great variation between the different scores as to the severity of calcification and there is no commonly accepted definition regarding the calcium burden. Furthermore, the impact of arterial calcification on the outcomes of the Eluvia™ DES has not been assessed to date and most prospective trials excluded patients with severely calcified disease [6, 12].
The aim of this study was to analyze the impact of calcification burden using three different calcium scoring systems on the 12 and 24 months outcomes of the Eluvia™ DES for FP occlusive disease.
Materials and Methods
This study followed the reporting guidelines from the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cohort studies [13].
Study Design, Setting and Participants
This is a retrospective analysis of prospectively collected data performed in line with the requirements of the local ethics committee and adhering to the declaration of Helsinki. The study is a secondary analysis of the “Muenster registry of the Eluvia drug-eluting stent for the Treatment of Complex Femoropopliteal Lesions, which was previously published, including all patients who had collected information of anatomical calcification scores [5]. Patients were included consecutively between March 2016 and December 2018. Inclusion criteria included ER of de novo or restenotic FP lesions using the Eluvia™ (Boston Scientific®) drug-eluting stent. Decision for using the Eluvia™ stent was based on the physician’s discretion. General indications for stenting were presence of recoil or flow-limiting dissection after plain old balloon angioplasty (POBA)—Fig. 1. The exclusion and inclusion criteria of this study have been previously reported (5). Finally, for the purposes of this analysis we excluded patients with no periprocedural imaging, which did not allow a quantification of the circumferential calcification of the vessel.

Intravascular lithotripsy prior to Eluvia™ Drug-eluting stent deployment for severely calcified femoropopliteal disease
Procedures were performed using an institutional protocol which has been explained elsewhere, including vessel preparation with POBA for 60 s (1 mm diameter less than the reference target vessel), followed by angiographic assessment [5]. In cases of flow-limiting dissection or residual stenosis > 50% one or multiple Eluvia™ stents were deployed to cover the respective length, followed by post-dilation with uncoated balloon sized at the reference stent diameter. The details and characteristics of the Eluvia™ stent have been described elsewhere [4, 5].
Following treatment, patients were followed by clinical assessment and duplex ultrasound at 6, 12 and 24 months. Patients were kept on dual anti-platelet therapy for 3 months with clopidogrel (75 mg/day) and aspirin (100 mg/day), followed by lifelong monotherapy with one or other. Patients previously on anti-coagulants, maintained their usual medication with an addition of aspirin or clopidogrel for 3 months. In case of clinical worsening and positive findings on duplex ultrasound (any flow-limitation or thrombosis) an angiography was performed followed by re-intervention.
Variables, Data Sources/Measurement, Bias and Study Size
Collected variables included patient demographics (age and sex), cardiovascular risk factors, and comorbidities (hypertension, diabetes mellitus, dyslipidemia, coronary artery disease, previous myocardial infarction, COPD, obesity, cerebrovascular disease, chronic kidney disease, smoking habits, and previous revascularizations). The Rutherford classification was used to classify the chronic lower limb ischemia (Categories 0–6). Chronic limb-threatening ischemia was considered for Rutherford categories 4–6. Extent of lesion was assessed on the pre- and intra-operative imaging (CT-angiography, fluoroscopy and digital subtraction angiography). Vessel calcification was assessed using the Peripheral Arterial Calcium Scoring System (PACSS) score (grade 0–4) [14], number of vessel quadrants affected (0,1,2,3 or 4) [11], presence of full lesion calcification (360°) and calcification score per Peripheral Academic Research Consortium (PARC) definitions (focal, mild, moderate, or severe) [10]—Table 1. Both the PACSS and PARC scores are based on antero-posterior views of fluoroscopy and digital subtraction angiographies performed intraoperatively; while, the analysis of quadrant involvement (circumferential involvement) was analyzed by pre-operative CT-angiography or periprocedural intravascular ultrasound imaging. Lesion length was analyzed as a continuous and categorical variable (> 150 cm and > 250 cm). Disease extension was classified according to the area of involvement (proximal SFA; mid SFA; distal SFA; popliteal P1, P2 and P3 levels).
Study Outcomes and Definitions
The main outcome was primary patency; while, secondary patency rate and freedom from target lesion revascularization (TLR) were additionally analyzed. All outcomes were analyzed by comparing the impact of calcium burden according to the different target vessel calcium scores.
Primary patency was defined as freedom from significant restenosis or occlusion without any re-intervention. Significant restenosis was defined as a peak systolic velocity ratio > 2.0, calculated as peak systolic flow velocity in the lesion divided by peak systolic velocity 1 cm proximal to the lesion. Secondary patency was defined as restored flow in the treated segment after occlusion or restenosis.
Statistical Analysis
Statistical analysis was carried out using SPSS 26.0 (IBM SPSS 26 Inc). Continuous variables are presented as mean ± standard deviation when normally distributed and median (with interquartile range-IQR) when not. Categorical variables are expressed in numbers (percentage). Students t-test was used when comparing continuous variables and the χ2 test to compare categorical variables, however, when necessary, the Mann–Whitney or Fisher exact test were used instead, respectively. Time to event outcomes (patency rates and TLR) were analyzed using Kaplan–Meier graphs and LogRank test for group comparison. Kaplan–Meyer graphs were produced using Stata/IC 16.1 (StataCorp, TX, USA). Statistics are presented comparing the different calcium scores. Calcium scores were group in three groups per each calcification being the baseline absent calcification and the remainder divided in two. All analyses were considered statistically significant if a two-tailed p-value < 0.05 was observed.
Results
Patients, Demographics and Risk Factors
Overall, 111 patients met the inclusion criteria of this study. Mean age was 71.2-year-old (± 7.9) and 64% (n = 71) were male. Most patients presented with Rutherford class 3 (n = 78, 79.9%), followed by class 5 (n = 14, 12.7%), class 4 (n = 11, 10%) and class 6 (n = 7, 6.4%)—Table 2.
The majority presented with TASC C/D lesions (n = 67, 61.5%) and 74.3% (n = 81) had chronic total occlusions. Mean lesion length was 197.6 mm (± 108.5); whereas, 58.6% (n = 65) and 40.4% (n = 44) had lesions longer than 150 and 250 mm, respectively—Table 3. Table 2 summarizes patient’s demographics and baseline characteristics.
Regarding the target vessel treated, proximal, middle, and distal SFA were involved in 50.9% (n = 54), 71.7% (n = 76) and 81.1% (n = 86) of cases, respectively. Furthermore, in 35.8% (n = 38) and 7.6% (n = 8) of cases, the P1 and P2 levels of the popliteal artery was involved. In no cases the treatment extended to the distal popliteal artery—Table 4.
Calcium Classification Scores
The burden of calcium according to each classification is described in Table 3 and Fig. 2. Regarding the PARC calcium score, 24 patients (21.6%) showed no visible calcification, 27 patients (24.3%) focal/mild calcification and 60 patients (54%) moderate/severe calcification. Regarding the PACSS, 24 patients (21.6%) were classified as grade 0, 23 patients (20.7%) as grade 1/2 and 64 patients (57.6%) as grade 3/4. Regarding the number of quadrants affected, in 16 patients (14.4%) 0 quadrants were affected, in 43 (38.7%) 1 to 2 quadrants affected and in 52 (46.8%) 3 to 4 quadrants.

Patient classification according to the different calcification scores. Y column represents the number of patients. Calcification score per Peripheral Academic Research Consortium (PARC) definitions (0- absent; 1-focal, 2-mild, 3-moderate, or 4-severe), Peripheral Arterial Calcium Scoring System (PACSS) score (grade 0–4), number of vessel quadrants affected (0,1,2,3 or 4)
Primary Outcome
Primary Patency
There were no differences in primary patency between the different calcification scores at 12 months (PARC score, LogRank = 0.42; PACSS, LogRank = 0.28; quadrants, LogRank = 0.29) and 24 months (PARC score, LogRank = 0.13; PACSS, LogRank = 0.13; quadrants, LogRank = 0.42)—Fig. 3.

Primary patency rates according to calcification scores. A primary patency rates according to the Peripheral Arterial Calcium Scoring System (PACSS) score; B primary patency rates according to the number of vessel quadrants affected (0–4) and C primary patency rates according to the calcification score per Peripheral Academic Research Consortium (PARC) definitions
Among other factors analyzed, only proximal SFA involvement and lesion length > 250 mm showed lower patency rates. Proximal SFA involvement showed lower patency at 12 months (LogRank = 0.022), but not at 24 months (LogRank = 0.08) and lesion length > 250 mm showed lower patency at 12 months (LogRank = 0.003) and 24 months (LogRank = 0.012), respectively.
Secondary Outcomes
Freedom from TLR
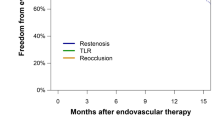
Freedom from TLR was significantly lower at 12 months in patients with calcification affecting 3 or 4 quadrants (LogRank = 0.022) but not at 24 months (LogRank = 0.36). The analysis of all other calcification scores revealed no significant differences at 12 months (PARC score, LogRank = 0.90; PACSS, LogRank = 0.0.78) or 24 months (PARC score, LogRank = 0.09; PACSS, LogRank = 0.11)—Fig. 4.

Freedom from target lesion revascularization (TLR) according to calcification scores. A Freedom from TLR according to the Peripheral Arterial Calcium Scoring System (PACSS) score; B freedom from TLR according to the number of vessel quadrants affected (0–4) and C freedom from TLR according to the calcification score per Peripheral Academic Research Consortium (PARC) definitions
Lesion length > 250 mm showed lower freedom from TLR at 12 (LogRank = 0.029) and 24 months (LogRank = 0.020). At 24 months proximal SFA involvement also increased the risk for TLR (LogRank = 0.043).
Secondary Patency
No differences in secondary patency were found between any of the different calcification scores at 12 months (PARC score, LogRank = 0.10; PACSS, LogRank = 0.09; quadrants, LogRank = 0.46) and 24 months (PARC score, LogRank = 0.13; PACSS, LogRank = 0.13; quadrants, LogRank = 0.42)—Fig. 5.

Secondary patency rates according to calcification scores. A Secondary patency rates according to the Peripheral Arterial Calcium Scoring System (PACSS) score; B secondary patency rates according to the number of vessel quadrants affected (0–4) and C secondary patency rates according to the calcification score per Peripheral Academic Research Consortium (PARC) definitions
Proximal SFA involvement showed lower secondary patency at 12 months (LogRank = 0.031) and at 24 months (LogRank = 0.011) and lesion length > 250 mm showed lower secondary patency at 12 months (LogRank = 0.007) and 24 months (LogRank < 0.001). Involvement of P1 and P2 showed lower secondary patency rates only at 24 months (LogRank = 0.022 and LogRank = 0.027, respectively).
Discussion
Calcification represents the Achilles’s heel of endovascular therapy and one of the main predictors of patency loss and TLR [15]. Different strategies have been developed to address this problem including specialty balloons, atherectomy, interwoven stents and intravascular lithotripsy [16]. Despite the promising performance of paclitaxel-coated balloons to inhibit restenosis in fibrotic lesions, the efficacy of this agent in calcified disease has been questioned and the outcomes of the new generation DES in heavily calcified disease has not been adequately investigated [17]. In this study, regardless the calcium score used, the presence of severe calcification did not influence the primary patency of the treated vessels. However, the freedom from TLR was significantly reduced in patients with 3 or 4 arterial quadrants affected by calcification. Regarding other factors affecting revascularization outcomes, lesion length > 250 mm, involvement of the proximal SFA and extension into the popliteal artery were found to be significant.
Long lesions have been considered at risk for restenosis especially if the lesion is not completely covered by the Eluvia™ (Boston Scientific®) stent. In the DESAFINADO registry primary patency at one year was 91% if the lesion was completely covered versus 42% if the DES was used in combination with BMS or POBA [18]. Spot stenting was significantly associated with increased risk of one-year restenosis in the Japanese CAPSICUM experience [19].
Previous studies evaluating the Eluvia™ DES results have shown acceptable results in complex FP lesions at both 12 and 24 months [4, 5, 20]. Stavroulakis et al. have published the 2-year results of the Eluvia™ DES in complex FP lesions, including 130 patients and showed a primary patency of 71%, secondary patency and freedom from TLR of 80%, freedom from major amputation of 98% and freedom from surgical conversion of 89% [5]. Additional studies have also shown good results with the Eluvia™ DES in complex disease with favorable results compared to both bare metal stents but also compared to previous DES [12, 21, 22]. Shehada et al. showed that the use of the Eluvia™ DES was associated with comparable mortality to bare metal stents for FP arterial disease, and improved patency in lesions longer than 15 cm6. The IMPERIAL trial [6, 22] compared the revascularization of FP lesions with the Eluvia DES compared to the Zilver PTX drug-coated stent. At 24 months, both stents showed adequate results with the Eluvia™ DES having a higher degree of freedom from TLR. Recent studies have also suggested that the Eluvia™ DES is more cost-effective than other available DES [23]. The ULTIMATE study also compared the Eluvia™ DES with a covered self-expanding stent and found the Eluvia™ DES to have higher rates of primary patency in lesions < 15 cm and higher freedom from TLR and acute limb ischemia [24]. Finally, in the EMINENT randomized controlled trial a higher primary patency was observed following Eluvia™ deployment compared to uncoated counterparts [6].
Regarding arterial calcification scores, different classifications and diagnostic modalities might influence the reporting of the results [10, 24, 25]. Current calcification scores are heterogenous and might difficult a head-to-head comparison between different studies [10, 11, 23]. Both the PACSS and PARC scores are assessed by fluoroscopy and digital subtraction angiographies on an antero-posterior projections, and both consider the lateral involvement and length of calcification, with the main difference being that the PARC uses a ratio of lesion length to vessel length; while, PACSS uses a cutoff of 5 cm for length (Table 1) [10, 14]. The circumferential analysis of calcification (quadrant classification) is based on an axial view of the vessel either with CT-angiography or IVUS. The differences of the classifications are highlighted in Table 1. In our results, the presence of severe calcification based on the PARC and PACSS scores did not predict any adverse outcomes. On the contrary, quadrant calcification involvement did predict a higher rate of TLR. Accordingly, in cases of severely calcified disease an additional imaging modality, which would enable the detection of circumferential calcification, might be more helpful than the fluoroscopic assessment of calcium burden [26]. Adequate stent expansion and wall apposition might be related with this finding, since circular calcification might be more challenging for adequate vessel preparation with POBA and stent expansion compared to non-circular calcifications [25]. Previous studies have shown the negative impact of calcification on outcomes of femoropopliteal stenting with DES, with higher rates of in-stent restenosis [27]. Circumferential calcification distribution has also been shown to predict worse post-operative outcomes after drug-eluting balloon treatment as shown previously by Fanelli et al. probably due to the limitations in drug delivery to complete or near complete circular calcified arteries [17]. This has been mirrored in other studies including drug-coated balloons [28]. Additionally, Bernardini et al. also demonstrated that calcification burden was an independent risk factor for failed antegrade crossing in patients with femoropopliteal chronic total occlusions [29]. All of these studies highlight the importance of an adequate pre-treatment assessment of the calcification burden of femoropopliteal lesions. However, angiography-based calcification scores have been shown to underestimate the degree of calcium burden on previous histological studies [30]. Furthermore, Yin et al. performed an analysis of femoropopliteal calcium severity using IVUS as the goldstandard compared to both PARC and PACSS scores and found a 59%, 100%, 100% and 14% sensitivity, specificity, positive predictive value, and negative predictive value of angiography-based scores compared to IVUS assessment [31]. Additionally, axial imaging analysis of vessel wall allowed for a more precise calcium location assessment including differentiating between medial calcification and intimal calcification, which have different pathophysiologic and prognostic implications [31]. These findings underscore the added benefit of having a pre-treatment axial anatomical analysis of the vessel wall.
Currently, vessel preparation techniques have been developed to treat severe calcified and complex lesions [32]. In the present study, vessel preparation was performed with POBA. In complete circular and complex calcified lesions, POBA might not be sufficient to adequately prepare the vessel to the delivery of the scaffold. These lesions might benefit from either a more aggressive vessel prep strategy (high-pressure-/scoring balloon angioplasty) or with the use of dedicated calcium devices (Fig. 1).
Similar to calcification there is a great variability among different position documents in regard to the definition of a ‘long-lesion’. Current European guidelines suggest that a lesion longer than 250 mm should be considered a long lesion; whereas, the PARC position document defined a long lesion as 150 mm [2, 10]. Moreover, in the IMPERIAL trial patients with a lesion length > 140 mm and ≤ 190 mm were analyzed in the subgroup of ‘long-lesions’ [20]. In this cohort, a lesion length > 250 mm was associated with increased risk for loss of primary and secondary patency as well as TLR. Accordingly, the definition suggested from the ESC/ESVS guidelines better predicted the risk for treatment failure.
Limitations
This study has several limitations. The low number of patients might explain the lack of statistically significant different in some of the outcomes. The calcification scoring was performed in non-automatized fashion. Although it was performed by experience interventionalists an automatized method of grading might be more accurate. Additionally, longer follow-up times would be of interest to analyze the long-term patency of the Eluvia™ DES in calcified disease. Although we standardized by calcium scores, multiple other factors influence revascularization outcomes. Future studies with more patients with detailed anatomic and clinical data, might allow a more robust analysis of the impact of calcium. Future studies are also needed to analyze the impact of different vessel preparation devices in both drug-coated balloons and drug-eluting stent technology. Furthermore, a clear definition of calcium arterial burden and adequate diagnostic modalities in the FP sector is necessary considering the circular involvement of the artery.
Conclusion
In this study, regardless the calcium score used, the presence of severe calcification did not influence the primary patency of the treated vessels after Eluvia™ DES deployment. However, the freedom from TLR was significantly reduced in patients with 3 or 4 arterial quadrants affected by calcification. Of the calcium scores used, only quadrant calcification involvement predicted revascularization failure. A more detailed anatomic evaluation of complex lesions might be necessary, and a fluoroscopic assessment alone might not be sufficient to appreciate these lesions.
References
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1):S1-109.
Aboyans V, Ricco JB, Bartelink MEL, Björck M, Brodmann M, Cohnert T, et al. Editor’s choice—2017 esc guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the european society for vascular surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55:305–68.
Stavroulakis K, Borowski M, Torsello G, Bisdas T, CRITISCH Collaborators. One-year results of first-line treatment strategies in patients with critical limb ischemia (CRITISCH registry). J Endovasc Ther. 2018;25:320–9.
Bisdas T, Beropoulis E, Argyriou A, Torsello G, Stavroulakis K. 1-Year all-comers analysis of the Eluvia drug-eluting stent for long femoropopliteal lesions after suboptimal angioplasty. JACC Cardiovasc Interv. 2018;11(10):957–66.
Stavroulakis K, Torsello G, Bosiers M, Argyriou A, Tsilimparis N, Bisdas T. 2-Year outcomes of the Eluvia drug-eluting stent for the treatment of complex femoropopliteal lesions. JACC Cardiovasc Interv. 2021;14(6):692–701.
Gouëffic Y, Torsello G, Zeller T, Esposito G, Vermassen F, Hausegger KA, Tepe G, Thieme M, Gschwandtner M, Kahlberg A, Schindewolf M, Sapoval M, Diaz-Cartelle J, Stavroulakis K, EMINENT Investigators. Efficacy of a drug-eluting stent versus bare metal stents for symptomatic femoropopliteal peripheral artery disease: primary results of the EMINENT randomized trial. Circulation. 2022;146(21):1564–76.
Konijn LC, Takx RA, de Jong PA, Spreen MI, Veger HT, Mali WP, van Overhagen H. Arterial calcification and long-term outcome in chronic limb-threatening ischemia patients. Eur J Radiol. 2020;132: 109305.
He HP, Weng JC, Zhao Y, Cai SH, Zhang XL, Yin HH. Impact of plaque calcification and stent oversizing on clinical outcomes of atherosclerotic femoropopliteal arterial occlusive disease following stent angioplasty. Eur J Vasc Endovasc Surg. 2019;58(2):215–22.
Tokuda T, Oba Y, Koshida R, Suzuki Y, Murata A, Ito T. The impact of femoropopliteal artery calcium score after endovascular treatment. Ann Vasc Surg. 2020;66:543–53.
Patel MR, Conte MS, Cutlip DE, Dib N, Geraghty P, Gray W, et al. Evaluation and treatment of patients with lower extremity peripheral artery disease: consensus definitions from Peripheral Academic Research Consortium (PARC). J Am Coll Cardiol. 2015;65(9):931–41.
Konijn LCD, van Overhagen H, Takx RAP, de Jong PA, Veger HTC, Mali WPTM. CT calcification patterns of peripheral arteries in patients without known peripheral arterial disease. Eur J Radiol. 2020;128: 108973.
Müller-Hülsbeck S, Benko A, Soga Y, Fujihara M, Iida O, Babaev A, O’Connor D, Zeller T, Dulas DD, Diaz-Cartelle J, Gray WA. Two-year efficacy and safety results from the IMPERIAL randomized study of the Eluvia polymer-coated drug-eluting stent and the Zilver PTX polymer-free drug-coated stent. Cardiovasc Interv Radiol. 2021;44(3):368–75.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12:1495–9.
Rocha-Singh KJ, Zeller T, Jaff MR. Peripheral arterial calcification: prevalence, mechanism, detection, and clinical implications. Catheter Cardiovasc Interv. 2014;83:E212–20.
Okuno S, Iida O, Shiraki T, Fujita M, Masuda M, Okamoto S, et al. Impact of calcification on clinical outcomes after endovascular therapy for superficial femoral artery disease: assessment using the peripheral artery calcification scoring system. J Endovasc Ther. 2016;23:731–7.
Stavroulakis K, Bisdas T, Torsello G, Tsilimparis N, Damerau S, Argyriou A. Intravascular Lithotripsy and drug-coated balloon angioplasty for severely calcified femoropopliteal arterial disease. J Endovasc Ther. 2022;7:15266028221075564.
Fanelli F, Cannavale A, Gazzetti M, Lucatelli P, Wlderk A, Cirelli C, et al. Calcium burden assessment and impact on drug-eluting balloons in peripheral arterial disease. Cardiovasc Interv Radiol. 2014;37:898–907.
Kum S, Ipema J, Huizing E, Tan YK, Lim D, Lok IY, et al. Outcomes of the paclitaxel-eluting Eluvia stent for long femoropopliteal lesions in Asian patients with predominantly chronic limb-threatening ischemia. Vasc Med. 2021;26:267–72.
Iida O, Takahara M, Soga Y, Yamaoka T, Fujihara M, Kawasaki D, et al. 1-Year outcomes of fluoropolymer-based drug-eluting stent in femoropopliteal practice: predictors of restenosis and aneurysmal degeneration. JACC Cardiovasc Interv. 2022;15:630–8.
Golzar J, Soga Y, Babaev A, Iida O, Kawasaki D, Bachinsky W, et al. Effectiveness and safety of a paclitaxel-eluting stent for superficial femoral artery lesions up to 190 mm: one-year outcomes of the single-arm IMPERIAL long lesion substudy of the Eluvia drug-eluting stent. J Endovasc Ther. 2020;27:296–303.
Shehada Y, Bisdas T, Argyriou A, Torsello G, Tsilimparis N, Beropoulis E, Stavroulakis K. Efficacy analysis following polymer coated drug eluting stent and bare metal stent deployment for femoropopliteal arterial disease. Vascular. 2022;7:17085381221126216.
Iida O, Fujihara M, Kawasaki D, Mori S, Yokoi H, Miyamoto A, Kichikawa K, Nakamura M, Ohki T, Diaz-Cartelle J, Müller-Hülsbeck S, Gray WA, Soga Y. 24-Month efficacy and safety results from Japanese patients in the imperial randomized study of the Eluvia drug-eluting stent and the zilver ptx drug-coated stent. Cardiovasc Interv Radiol. 2021;44(9):1367–74.
Gray WA, Griffiths RI, Elroy PWM, Amorosi SL, McGovern AM, Jaff MR, et al. Cost-effectiveness of a paclitaxel-eluting stent (Eluvia) compared to Zilver PTX for endovascular femoropopliteal intervention. J Med Econ. 2022;25:880–7.
Ichihashi S, Takahara M, Yamaoka T, Hara M, Kobayashi T, Tamai H, et al. Drug eluting versus covered stent for femoropopliteal artery lesions: results of the ULTIMATE study. Eur J Vasc Endovasc Surg. 2022;S1078–5884(22):00348–53.
Dias-Neto M, Matschuck M, Bausback Y, Banning-Eichenseher U, Steiner S, et al. Endovascular treatment of severely calcified femoropopliteal lesions using the “pave-and-crack” technique: technical description and 12-month results. J Endovasc Ther. 2018;25:334–42.
Fujihara M, Kozuki A, Tsubakimoto Y, Takahara M, Shintani Y, Fukunaga M, et al. Lumen gain after endovascular therapy in calcified superficial femoral artery occlusive disease assessed by intravascular ultrasound (code study). J Endovasc Ther. 2019;26:322–30.
Ichihashi S, Shibata T, Fujimura N, Nagatomi S, Yamamoto H, Kyuragi R, Adachi A, Iwakoshi S, Bolstad F, Saeki K, Obayashi K, Kichikawa K. Vessel calcification as a risk factor for in-stent restenosis in complex femoropopliteal lesions after Zilver PTX paclitaxel-coated stent placement. J Endovasc Ther. 2019;26(5):613–20.
Mori S, Takahara M, Nakama T, Tobita K, Hayakawa N, Iwata Y, Horie K, Suzuki K, Yamawaki M, Ito Y. Impact of calcification on clinical outcomes after drug-coated balloon angioplasty for superficial femoral artery disease: assessment using the peripheral artery calcification scoring system. Catheter Cardiovasc Interv. 2023;101(5):892–9.
Bernardini G, Bisdas T, Argyriou A, Saab F, Torsello G, Tsilimparis N, Stavroulakis K. Risk factor analysis for crossing failure in primary antegrade wire-catheter approach for femoropopliteal chronic total occlusions. J Endovasc Ther. 2023;30(3):433–40.
Maehara A, Mintz GS, Shimshak TM, Ricotta JJ 2nd, Ramaiah V, Foster MT 3rd, et al. Intravascular ultrasound evaluation of JETSTREAM atherectomy removal of superficial calcium in peripheral arteries. EuroIntervention. 2015;11:96–103.
Yin D, Maehara A, Shimshak TM, Ricotta JJ 2nd, Ramaiah V, Foster MT 3rd. Intravascular ultrasound validation of contemporary angiographic scores evaluating the severity of calcification in peripheral arteries. J Endovasc Ther. 2017;24:478–87.
Stavroulakis K, Argyriou A, Watts M, Varghese JJ, Estes BA, Torsello G, et al. How to deal with calcium in the superficial femoral artery. J Cardiovasc Surg (Torino). 2019;60:572–81.
Acknowledgements
None.
Funding
The authors state there was no funding for the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Konstantinos Stavroulakis—Consulting for Phillips, Shockwave, Boston Scientific, Terumo and received Honoraria from Medtronic, Bentley, Abbott and Biotronik; Giovanni Torsello—consulting for Medtronic, Boston Scientific and received grants from Medtronic, Gore, Cook and Cordis; Theodosios Bisdas—Consulting for Boston Scientific, Medtronic, BARD and COOK Medical and Nikolaos Tsilimparis—Proctor for and has received institutional Research funding from Cook Medical. All remaining authors declare no conflict of interest.
Ethical Approval
Ethical approval was obtained from St. Franziskus-Hospital GmbH, Muenster, Germany—Reference number- N:2021-2020-f-S.
Informed Consent
All patients signed the informed consent for both the procedures and publication of the outcomes data.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gouveia e Melo, R., Torsello, G., Argyriou, A. et al. Impact of Calcification on the Outcomes of Femoropopliteal Artery Endovascular Treatment Using a Polymer Coated Drug-Eluting Stent. Cardiovasc Intervent Radiol 47, 543–553 (2024). https://doi.org/10.1007/s00270-024-03662-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-024-03662-8