
Abstract
Purpose
To determine the incidence and the risks factors of peripherally inserted central catheter (PICC)-related infectious complications.
Materials and Methods
Medical charts of every in-patient that underwent a PICC insertion in our hospital between January 2010 and October 2013 were reviewed. All PICC-related infections were recorded and categorized as catheter-related bloodstream infections (CR-BSI), exit-site infections, and septic thrombophlebitis.
Results
Nine hundred and twenty-three PICCs were placed in 644 unique patients, mostly male (68.3 %) with a median age of 58 years. 31 (3.4 %) PICC-related infections occurred during the study period corresponding to an infection rate of 1.64 per 1000 catheter-days. We observed 27 (87.1 %) CR-BSI, corresponding to a rate of 1.43 per 1000 catheter-days, 3 (9.7 %) septic thrombophlebitis, and 1 (3.2 %) exit-site infection. Multivariate logistic regression analysis showed a higher PICC-related infection rate with chemotherapy (odds ratio (OR) 7.2–confidence interval (CI) 95 % [1.77–29.5]), auto/allograft (OR 5.9–CI 95 % [1.2–29.2]), and anti-coagulant therapy (OR 2.2–95 % [1.4–12]).
Conclusion
Chemotherapy, auto/allograft, and anti-coagulant therapy are associated with an increased risk of developing PICC-related infections.
Clinical Advance
Chemotherapy, auto/allograft, and anti-coagulant therapy are important predictors of PICC-associated infections. A careful assessment of these risk factors may be important for future success in preventing PICC-related infections.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Peripherally inserted central catheters (PICC) are venous catheters inserted into a peripheral upper limb vein, with a tip located at the junction of the superior vena cava with the right atrium, categorized as central venous catheters (CVC).
The use of PICC has significantly grown for hospitalized patients needing intermediate to long-term reliable venous access. Indeed, this device presents several advantages: it represents a less invasive and a less risky alternative to classic central venous catheters (CVC), the introduction of which through the internal jugular or sub-clavian vein can result with pneumothorax [1]. Furthermore, PICCs are easily removed and remain a safe and cost-effective technique [2].
But, one of the main reasons of this increased use of PICC is that initial studies showed that PICC-related bloodstream infection (BSI) rates were significantly lower than rates associated with CVCs [3, 4]. However, more recent studies questioned this fact and suggested that PICC-related BSI rate was not uniform [3, 5]. For instance, Ajenjo et al. retrospective study showed that PICC-related BSI was almost twice as likely for PICCs inserted in intensive care unit (ICU) settings compared with non-ICU settings [3, 6]. Furthermore, the PICC-related BSI rate they observed was comparable to rates for all central venous catheter-associated bloodstream infection [6], which was confirmed by Chopra et al. [5] in a meta-analysis.
However, few data exist concerning risk patterns of infections associated with PICC in hospitalized adult patients [6–8]. Therefore, we decided to retrospectively study the incidence and identify risk factors of PICC-related infections in a large cohort of patients.
Materials and Methods
Study Population and Setting
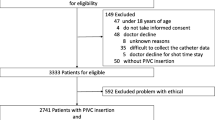
This retrospective study was set in a hospital that included surgical and medical units, as well as medical and hematological oncology units (performing autologous and allogeneic stem cells transplantation). We identified all hospitalized patients who underwent PICC line insertion between January 2010 and October 2013. Patients coming to our hospital from another facility only for the duration of the PICC insertion procedure were excluded.
Ethics committee of our hospital (May 2015) approved our protocol.
PICC Insertion Procedure
All PICCs were inserted under ultrasound and fluoroscopic guidance either by a trained senior interventional radiologist or by a junior radiologist. The procedure occurred in an angiography operating room using maximal sterile barrier precaution as recommended by the Centers for Disease Control and Prevention (CDC) including mask, hat, sterile gloves, sterile gown, and a sterile full body drape [9]. Prior to the PICC insertion, all patients had a cutaneous preparation consisting in showering with a chlorhexidine surgical scrub and a second skin preparation at the time of the insertion, in accordance to the CDC’s recommendations. Four-, five- and six-French single or dual lumen Bard PowerPICC and PowerPICC Solo (Bard Access Systems, Salt Lake City, UT, USA) catheters were used in our patients. We systematically used the smallest caliber of PICC in the largest vein available. PICCs were inserted in an upper limb vein, preferentially in the basilic vein to reduce the risks of brachial artery puncture or, if not possible because of anatomic variations or poor quality or thrombosed vein, in the brachial or cephalic vein. The non-dominant upper limb was preferred to the dominant one mainly for reasons of comfort and convenience for the patient.
PICC was held in place with StatLock adhesive dressings (StatLock, Bard, Murray Hill, NJ, USA). Once the PICC was placed, the insertion site was covered with a sterile dressing.
Data Collection
All data were retrospectively extracted from angiographic and electronic medical records. The PICC-related infections were identified using those same records and the hospital laboratory database for the microbiology data with the help of a biologist.
We collected information concerning the patients’ demographic characteristics (gender, age), medical history (active cancer, solid or hematologic malignancy, metastatic disease), cardiovascular risk factors (hypertension, dyslipidemia, type II diabetes, and active smoking), and white cells blood count (neutropenia) at the time of the PICC placement.
We also collected data concerning the PICC insertion: indication (including chemotherapy, antibiotic therapy, blood transfusion, autologous and allogeneic stem cell transplantation, total parenteral nutrition, hydration and poor peripheral venous access), operator (senior or junior radiologist), date of PICC insertion and removal, site of insertion (side and vein), and device characteristics (size, number of lumens, valved or clamped PICC).
Definitions
We took in consideration three different types of PICC-related infectious complications: PICC-related bloodstream infection (BSI), exit-site infection, and septic thrombophlebitis.
The following definitions were used:
-
Catheter-related bloodstream infection (CR-BSI) was defined, according to the Infectious Diseases Society of America (IDSA) guidelines, as a bacteremia in a patient who has an intravascular device and at least one positive blood culture result obtained from the peripheral vein, clinical manifestations of infection (e.g., fever, chills, and/or hypotension), and no apparent source for bloodstream infection (with the exception of the catheter). One of the following should be present:
-
a positive result of semiquantitative (>15 colony-forming unit (cfu) per catheter segment) or quantitative (>102 cfu per catheter segment) catheter culture, whereby the same organism is isolated from a catheter tip and a peripheral blood culture;
-
simultaneous quantitative cultures of blood with a ratio at least of 3:1 cfu/ml of blood (catheter vs. peripheral blood): differential time to positivity (growth in a culture of blood obtained through a catheter hub is detected by an automated blood culture system at least 2 h earlier than a culture of simultaneously drawn peripheral blood of equal volume) [10].
-
-
Exit-site infection: we used the Infectious Diseases Society of America recommendations clinical definition, which consists in the presence of erythema, induration, and/or tenderness within 2 cm of the catheter exit site, which may be associated with other signs and symptoms of infection, such as fever or pus emerging from the exit site, with or without concomitant bloodstream infection [10, 11].
-
Septic thrombophlebitis: it was defined as induration or erythema, warmth, pain, or tenderness along the tract catheterized vein as defined by Mermel et al. [10]. The septic thrombophlebitis also met the criteria of CR-BSI giving that, as exposed bellow, we had the germs involved for all those thrombophlebitis.
According to the CDC’s National Healthcare Safety Network (NHSN), central line-associated bloodstream infection (CLABSI) was defined as a primary bloodstream infection in a patient with a central line within the 48-h prior to the onset of symptoms and the infection was not bloodstream related to an infection from another site.
These events were classified as “CLABSI: microbiologic” if the decision to remove the CVC was based upon exit swab or blood culture result (central or peripheral), where criteria for the CR-BSI definition were not fulfilled, and classified as “CLABSI: clinical” if the decision to remove the CVC was based upon clinical factors only (cause of fever not identified by septic workup, or fever persisting despite empiric antimicrobial therapy) [10, 12].
Statistical Analysis
All calculations and description of the patient group used PICC placements and not individual patients as the unit for counting. Each PICC insertion was regarded as a separate event. The main outcome was the occurrence of PICC-related infections as defined above.
Then we estimated the overall incidence rates (incidence rate per 1000 catheter-days) of PICC-related infections. The PICC-related infections rate was defined as the number of PICC-related infections divided by the number of catheter-days during the study period, multiplied by 1000.
To compare distribution of qualitative variables between groups (infection vs. absence of infection), Pearson χ 2 test was used if the applying conditions were verified and otherwise Fisher’s exact test. Variables for which p value was ≤0.20 were included in a multivariate logistical regression model.
We considered p values of less than 0.05 to be statistically significant.
Data analysis was performed using (STATA 12®) Software.
Results
Patients and PICC Characteristics
Between January 2010 and October 2013, 923 PICCs were placed in 644 unique patients for a total of 18,888 catheter-days. 179 patients had more than one PICC inserted during this period: 127 patients had 2, 26 patients had 3, 13 patients had 4, 7 patients had 5, 4 patients had 6, 1 patient had 7, and 1 patient had 8 PICCs placed.
Most of patients were male (68.3 %) with a median age of 58 years (range 18–103). 64.4 % of our patients presented with an oncologic underlying condition: 433 patients (72.9 % of the oncologic sub-cohort) suffered from a hematological malignancy and 161 from a solid neoplasia.
The two most common indications for PICC insertion were chemotherapy (37.9 %, n = 350) and long-term antibiotic administration (37.2 %, n = 343). The median PICC dwell time was 15 days (mean 20.5 days; range 0–433); 176 (19.1 %) PICCs were in place less than 1 week and 325 (35.2 %) at least 3 weeks.
A trained senior interventional radiologist inserted the large majority of devices (75.6 %, n = 698). Even though some data concerning the PICC size, the number of lumens and the site of insertion (side and vein) were not collected due to incomplete records, most of the PICCs inserted were small to medium size (97.4 %, n = 899 were 4 or 5 French) single-lumen devices (80.6 %, n = 744) and were mainly introduced in the left arm (70.7 %, n = 653) and in the basilic vein (68.2 %, n = 629). The demographic profile of the cohort and the devices characteristics are listed in Table 1.
Infectious Complications
31 (3.4 %) PICC-related infections occurred during the study period corresponding to an infection rate of 1.64 per 1000 catheter-days with a PICC-related BSI rate of 1.43 per 1000 catheter-days. Those complications consisted in 27 (87.1 %) PICC-related bloodstream infections, 3 (9.7 %) septic thrombophlebitis, and 1 (3.2 %) exit-site infection (Table 2).
All of these infections occurred in the oncologic sub-cohort of our study in which infection rate was, therefore, higher (2.64 per 1000 catheter-days) than in the whole cohort. In the onco-hematologic sub-cohort, this rate was even higher (3.13 PICC-related infections per 1000 catheter-days).
Furthermore, among the 923 PICCs included in our study, 40 were removed because they were suspected of developing a PICC-related infection, corresponding to a suspicion of infection rate of 2.12 per 1000 catheter-days. Characteristics of infected and non-infected PICCs are detailed in Table 3.
Microbiology
Almost one-third of the PICC-related infections were polymicrobial infections (32.3 %, n = 10), 4 (12.9 %) were caused by methicillin-resistant Staphylococcus epidermidis and 3 (9.7 %) by Stenotrophomonas maltophilia. All of the different pathogens responsible for the PICC-related BSI, the exit-site infection, and the septic thrombophlebitis are listed in Table 4.
Risk Factors of PICC-Related Infections
Multivariate logistic regression analysis showed that the risk of PICC-related infection was significantly associated with anti-coagulant therapy (OR 4.1–95 % CI [1.4–12.0]) and with the indication of PICC placement, the risk being higher with chemotherapy (OR 7.2–95 % CI [1.8–29.6]) or auto/allograft (OR 6.0 –95 % CI [1.2–29.3]) as compared to other indications (Table 5).
Discussion
In this study, the PICC-related BSI rate was 1.64 per 1000 catheter-days, which was lower than reported in the literature. For instance, Gunst et al. had a rate infection of 2.2 per 1000 catheter-days in their cohort made of surgical intensive care unit patients [13] and Ajenjo et al. found 2.78 PICC-BSIs per 1000 catheter-days in non-ICU patients [6]. Moreover, Chopra et al. reported recently, in a retrospective study, an infection rate of 2.16 per catheter-days [7] in a similar cohort of 966 PICCs inserted in 747 patients.
Our lower infection rate could be due to the fact that very few ICU patients were included in comparison with Gunst’s and Chopra’s cohorts [7, 13]. However, this was partially offset by high recruitment of oncologic (64 %) and onco-hematologic (46 %) patients whom are known to be at increased risk of infection because of immunosuppression [14, 15]. Yet, several authors reported that oncologic patients presented a higher PICC-related infection than non-oncologic ones: 6.61 per 1000 catheter-days in patients with hematological malignancies [15], 2.46 per 1000 catheter-days in oncologic patients (80 % of whom presented with solid tumors) [16] versus 1.1 per 1000 catheter-days in non-oncologic patients [4]. In our different sub-cohorts of solid neoplasia and hematologic malignancy patients, we also observed lower PICC-related infection rates than in the literature since ours are 1.45 and 3.13 per 1000 catheter-days respectively, versus 2.46 and 6.61 in oncologic and onco-hematologic patients, respectively [15, 16]. Despite our low recruitment of ICU patients, we therefore considered that our PICC-related infection rate was low considering the proportion of oncologic patients in our study, especially the important inclusion of onco-hematologic ones, and the absence of outpatients whose PICC-related infection rate, according to the literature, is low (0.52 per 1000 catheter-days [17]).
Two different and independent risk factors of PICC-related infection emerged from this study: chemotherapy or auto/allograft as an indication of PICC placement.
Chemotherapy had previously been suspected of being a risk factor of PICC-related infections in Worth et al. [15] and Chopra et al. [7] studies but none of them found a significant statistical association to prove this assumption: the Odds ratio were 1.23 (p = 0.74) and 1.8 (p = 0.3) respectively, whereas we obtained an Odds-ratio of 7.2 (95 % CI [1.8–29.6]). The higher rate of PICC-related infections in patients undergoing chemotherapy was probably due to the immunosuppression generated by the different chemotherapy agents in patients vulnerable to infection often presenting with a previous altered general state. As previously mentioned, patients presenting with hematological malignancies were at higher risk of PICC-related infections, and, particularly in patients necessitating an autologous or allogeneic stem cell transplantation (OR 6, 95 % CI [1.2–29.3]) whose PICC-related infection rate was 2.93 per 1000 catheter-days. This rate was pretty close to the one that Bellesi et al. found in their cohort of 60 autologous peripheral stem cell transplantation procedures (2.3 per 1000 catheter-days) [18]. Worth et al. also considered that the indication of hematopoietic stem cell transplantation as a potential PICC-related infection risk factor but did not obtained significant results [15]. Once again, this risk factor could be explained by the important immunosuppression and general fragility presented by this type of patients.
Our multivariate analysis pointed out a third risk factor of PICC-related infections: anti-coagulant therapy. Indeed, 5 of the 31 patients who presented with PICC-related infections had an anti-coagulant therapy and three of those five patients had a history of CVC-related deep vein thrombosis, two of those CVCs being PICCs. That is why we assumed that the anti-coagulant therapy might be an artificial risk factor of PICC-related infections: the treatment could cover the history of PICC-related thrombosis which is a well-know risk factor of catheter-related infection.
A few other risk factors of PICC-related infections have been observed in the literature but were not found in our study, even though we considered them as potential risk factors. For instance, Advani et al. found that PICCs in place for more than 21 days were 1.5 times more likely to be complicated by central line-associated bloodstream infection (CLABSI) compared with PICC placed for a lesser duration [19], whereas device dwell time does not influence PICC-related infection outbreak. They also demonstrated that administration of parenteral nutrition was an indication for PICC insertion is an independent risk factor for CLABSI. However, our two cohorts were not comparable since theirs was exclusively composed of pediatric patients. Furthermore, only very few of our PICCs were placed to administrate parenteral nutrition. ICU status turned out to be a significant risk factor of infection in three different studies [6, 7, 19]. We did not find this statement in our paper, probably because, as pointed out above, our recruitment of ICU patients was low.
In our review of literature, we found two studies pointing out a significant difference in the incidence of PICC-related infections between clamped and valved devices. Hoffer et al. showed that the incidence of infection was 50 % greater in the clamped catheter group (p = 0.02) than in the valved catheter group [20], whereas Ong et al. noted a significantly higher incidence of catheter-related infection (6.2 vs. 2 %, p = 0.04) in the distal valve PICCs than in the proximal valve ones [21]. In these studies, there were as many valved as clamped devices, whereas we inserted mostly (60 %) clamped PICCs, which could explain that we did not find a significant difference between the devices. However, the antagonism of the results of the two studies mentioned above suggested that these device characteristics might not be relevant in the outbreak of catheter-related infections. The number of lumen was found to play a part in the incidence of PICC-related infections. Indeed, Chopra et al. found that double and triple lumens were associated with greater risk of infection than single lumen ones (Hazard ratios: 4.08 (p = 0.006) and 8.52 (p = 0.0003) for double and triple lumen PICCs, respectively) [7], corroborating what Pongruangporn et al. showed one year before (OR for double lumen, 1.89; p = 0.01; OR for triple lumen, 2.87; p = 0.004) [22]. The large majority of the PICCs we placed in our patients were single lumen (80.6 %), this is probably why the number of lumen did not turn out to be a significant risk factor of infection in our statistical analysis.
Our study presented several limitations, the major one being its retrospective character exposing us to bias and to lack of data concerning some of the PICC characteristics even if we believe that the important size of the cohort and the relative mild number of missing data lowered the probability of missing outcomes. However, no patients were lost to follow-up. Indeed, only 38 (4 %) patients left our hospital with the device, all of them were onco-hematologic patients. 22 of those 38 patients had their device removed during hospital day care in our facility. The 16 others left our establishment for a long-term care institution and were transferred to our facility if a PICC-related complication occurred.
Another limitation of our study could be that all of our devices were placed by radiologists. Indeed, in our country, we do not have nursing-based venous access team because of forensic barriers: PICC insertion is considered as a medical procedure that cannot be delegated to nurses. This could constitute a bias since, in a recent study, Chopra proved that the rate of PICC-related infection is much higher when the device is placed by a radiologist in a comparison with the nurse team (OR 2.57, 95 % CI [1.41–4.68]) [7], although it is specified in this article that radiologists handled the difficult or technically unfeasible PICC placements [7], which could also be a significant bias.
Other limitations were the fact that the study was conducted in a single center and that almost half of our patients presented with hematological malignancy (46.3 %), which could limit generalizability to other hospitalized adult patients populations. Finally, we might underestimate the incidence of PICC-related infections in non-oncologic patients. Indeed, non-oncologic patients being less vulnerable to infection, PICC were probably easily removed in case of minor dysfunction (or infection suspicion) without systematic blood cultures. Therefore, in case of suspected CR-BSI, treating clinicians should be encouraged to perform more blood samples from PICCs in order to avoid unnecessary systematic removals of those devices. In contrast, we probably overestimate the role of chemotherapy, autologous, and allogeneic stem cell transplantations and neutropenia in the occurrence of PICC-related infections because catheter-related infections were systematically suspected in immunosuppressed patients in the absence of clinically identified source of possible infection. This procedure was justified by the higher morbidity and mortality of those fragile patients and was reflected by the rate of suspected PICC-related infection (2.12 per 1000 catheter-days).
In conclusion, chemotherapy and auto/allograft as an indication for PICC placement appeared to be strong and independent risk factors of developing PICC-related infections and need to be carefully assessed for future success in preventing this complication.
References
Ugas MA, Cho H, Trilling GM, Tahir Z, Raja HF, Ramadan S, Jerjes W, Giannoudis PV. Central and peripheral venous lines-associated blood stream infections in the critically ill surgical patients. Ann Surg Innov Res. 2012;6(1):8.
Ng PK, Ault MJ, Ellrodt AG, Maldonado L. Peripherally inserted central catheters in general medicine. Mayo Clin Proc. 1997;72(3):225–33.
Chopra V, Flanders SA, Saint S. The problem with peripherally inserted central catheters. J Am Med Assoc. 2012;308(15):1527–8.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clin Proc. 2006;81(9):1159–71.
Chopra V, O’Horo JC, Rogers MA, Maki DG, Safdar N. The risk of bloodstream infection associated with peripherally inserted central catheters compared with central venous catheters in adults: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2013;34(9):908–18.
Ajenjo MC, Morley JC, Russo AJ, McMullen KM, Robinson C, Williams RC, Warren DK. Peripherally inserted central venous catheter-associated bloodstream infections in hospitalized adult patients. Infect Control Hosp Epidemiol. 2011;32(2):125–30.
Chopra V, Ratz D, Kuhn L, Lopus T, Chenoweth C, Krein S. PICC-associated bloodstream infections: prevalence, patterns, and predictors. Am J Med. 2014;127(4):319–28.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128(2):489–95.
O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, Lipsett PA, Masur H, Mermel LA, Pearson ML, et al. Guidelines for the prevention of intravascular catheter-related infections. Am J Infect Control. 2011;39(4 Suppl 1):S1–34.
Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP, Raad II, Rijnders BJ, Sherertz RJ, Warren DK. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;49(1):1–45.
Horan TC, Emori TG. Definitions of key terms used in the NNIS System. Am J Infect Control. 1997;25(2):112–6.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–32.
Gunst M, Matsushima K, Vanek S, Gunst R, Shafi S, Frankel H. Peripherally inserted central catheters may lower the incidence of catheter-related blood stream infections in patients in surgical intensive care units. Surg Infect. 2011;12(4):279–82.
Cheong K, Perry D, Karapetis C, Koczwara B. High rate of complications associated with peripherally inserted central venous catheters in patients with solid tumours. Intern Med J. 2004;34(5):234–8.
Worth LJ, Seymour JF, Slavin MA. Infective and thrombotic complications of central venous catheters in patients with hematological malignancy: prospective evaluation of nontunneled devices. Support Care Cancer. 2009;17(7):811–8.
Walshe LJ, Malak SF, Eagan J, Sepkowitz KA. Complication rates among cancer patients with peripherally inserted central catheters. J Clin Oncol. 2002;20(15):3276–81.
Baumgarten K, Hale Y, Messonnier M, McCabe M, Albright M, Bergeron E. Bridging the gap: a collaborative to reduce peripherally inserted central catheter infections in the home care environment. Ochsner J. 2013;13(3):352–8.
Bellesi S, Chiusolo P, De Pascale G, Pittiruti M, Scoppettuolo G, Metafuni E, Giammarco S, Sora F, Laurenti L, Leone G, et al. Peripherally inserted central catheters (PICCs) in the management of oncohematological patients submitted to autologous stem cell transplantation. Support Care Cancer. 2013;21(2):531–5.
Advani S, Reich NG, Sengupta A, Gosey L, Milstone AM. Central line-associated bloodstream infection in hospitalized children with peripherally inserted central venous catheters: extending risk analyses outside the intensive care unit. Clin Infect Dis. 2011;52(9):1108–15.
Hoffer EK, Borsa J, Santulli P, Bloch R, Fontaine AB. Prospective randomized comparison of valved versus nonvalved peripherally inserted central vein catheters. Am J Roentgenol. 1999;173(5):1393–8.
Ong CK, Venkatesh SK, Lau GB, Wang SC. Prospective randomized comparative evaluation of proximal valve polyurethane and distal valve silicone peripherally inserted central catheters. J Vasc Interv Radiol. 2010;21(8):1191–6.
Pongruangporn M, Ajenjo MC, Russo AJ, McMullen KM, Robinson C, Williams RC, Warren DK. Patient- and device-specific risk factors for peripherally inserted central venous catheter-related bloodstream infections. Infect Control Hosp Epidemiol. 2013;34(2):184–9.
Acknowledgments
All the authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article and state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
I, Dr. Caroline Bouzad, declare that I have no conflict of interest to disclose.
Ethical Approval
Institutional Review Board approval was obtained. This study is a retrospective one.
Informed Consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Bouzad, C., Duron, S., Bousquet, A. et al. Peripherally Inserted Central Catheter-Related Infections in a Cohort of Hospitalized Adult Patients. Cardiovasc Intervent Radiol 39, 385–393 (2016). https://doi.org/10.1007/s00270-015-1182-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-015-1182-4