
Abstract
Introduction
Trauma is a leading cause of morbidity and mortality worldwide, and patients in low- and middle-income countries are disproportionately affected. Organized trauma systems, including appropriate transfer to a higher level of care, improve trauma outcomes. We sought to evaluate the relationship between transfer status and trauma mortality in Malawi.
Methods
We performed a retrospective analysis of trauma patients admitted to Kamuzu Central Hospital (KCH), a trauma center in Lilongwe, Malawi, between January 1, 2013, and May 30, 2018. Transfer status was categorized as direct if a patient arrives at KCH from the injury scene and indirect if a patient comes to KCH from another health care facility. We used logistic regression modeling to evaluate the relationship between transfer status and in-hospital mortality.
Results
A total of 8369 patients were included in the study. The mean age was 34.6 years (SD 15.8), and 81% of patients were male. The most common mechanism of injury was motor vehicle collision. Injury severity did not significantly differ between the two groups. Crude mortality was 4.8% for indirect and 2.6% for direct transfers. After adjusting for relevant covariates, odds ratio of mortality was 2.12 (1.49–3.02, p < 0.001) for indirect versus direct transfers.
Conclusion
Trauma patients indirectly transferred to a trauma center have nearly double the risk of mortality compared to direct transfers. Trauma outcome improvement efforts must focus on strengthening prehospital care, improving district hospital capacity, and developing protocols for early assessment, treatment, and transfer of trauma patients to a trauma center.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to the Lancet Global Burden of Disease study, 4.3 million deaths worldwide in 2019 are directly attributable to injury [1]. Low- and middle-income countries (LMICs) are disproportionately burdened by trauma, and 90% of injury-related deaths occur in LMICs [2]. It is estimated that nearly 2 million lives could be saved every year in LMICs in the presence of trauma systems [3].
Prior studies have shown that transfer status (direct transfer from injury scene to a trauma center versus indirect transfer from another health facility) affects patient outcomes. Direct transfer from the injury scene to a trauma center may reduce time to definitive management. Still, indirect transfer, particularly in countries with little prehospital care, may reduce time to initial resuscitation. The association between transfer status and outcomes for trauma patients was evaluated in two systematic reviews and meta-analyses in the last 10 years [4, 5]. Neither found a significant association between transfer status and mortality, but most studies included in these reviews were from high-income countries (HICs). It is unclear whether these findings apply to low-resource settings.
Malawi is a low-income country in Sub-Saharan Africa. It has over 18 million people and only 0.43 specialist surgical providers per 100,000 [6]. As in many LMICs, Malawi does not have an organized prehospital system, and the capacity of district hospitals to provide trauma care is limited [7]. In addition, there are no established protocols for patient triage and transfer. Understanding the relationship between transfer status and patient outcomes is crucial for trauma system design and protocol development in LMICs. This study aims to compare mortality rates between directly transferred (DT) and indirectly transferred (IT) trauma patients treated at a tertiary care hospital in Lilongwe, Malawi. We hypothesize that IT patients have higher mortality rates than DT patients.
Methods
Setting
Kamuzu Central Hospital (KCH), located in Malawi’s capital city of Lilongwe, is one of four referral hospitals in the country [8]. Over 15,000 trauma patients are seen in the KCH emergency department every year, and about 15% of these are admitted for further management [9, 10]. KCH is a 1000-bed tertiary referral center with a 6-bed intensive care unit, 6 operating theaters, a blood bank, and a dialysis unit. In 2008, the University of North Carolina established a trauma registry at KCH. Data clerks record patient and injury characteristics 24 h per day in the emergency department. Patients are followed until discharge, and treatments and outcomes are captured.
Data collection
Using the KCH trauma registry, we performed a retrospective cohort study of trauma patients admitted to KCH between January 1, 2013, and May 30, 2018. Patients were eligible for inclusion if they were ≥ 12 years old and admitted for management of traumatic injuries. We use this cutoff age because in this setting all patients 12 years of age or older are managed by the adult trauma surgery service. We chose this date range because of improvements in data collection that began in 2013. We excluded patients who were discharged from the ED, died before admission (either arrived dead or died in the ED), or were missing transfer status.
The primary exposure variable was transfer status, categorized as direct transfer (DT) if the patient arrived at KCH from the injury scene, and indirect transfer (IT) if the patient was initially evaluated at another facility and then transferred to KCH. The primary outcome was in-hospital mortality. The following demographic and injury-related data were also collected: sex, age, mechanism of injury, location of primary injury, mode of transport to KCH, time from injury to presentation at KCH, initial Glasgow Coma Score (GCS), Malawi Trauma Score (MTS), operative intervention, chest tube placement, and discharge disposition.
The Malawi Trauma Score (MTS) is a tool for assessing injury severity and predicting injury-associated mortality [9]. The score ranges from 2 to 32 and includes the following five components: AVPU score, anatomic location of injury, presence or absence of radial pulse on examination, age, and sex. A score of 25 is associated with a 50% probability of mortality [9]. Mechanism of injury was characterized as motor vehicle collision (MVC), pedestrian struck by a vehicle, gunshot wound (GSW), fall, assault, burn or electrical shock, or other. Location of primary injury was categorized as head, face, spine, chest, abdomen or pelvis, extremity, or other. Mode of transport was characterized as an emergency vehicle (ambulance or police vehicle), non-emergency motorized vehicle (private vehicle, company car, bus, minibus, or lorry), or non-motorized transport (walking or bicycle).
Statistical analysis
Bivariate analysis was used to compare the direct transfer (DT) and indirect transfer (IT) cohorts. We used Pearson’s chi-square test to assess differences in proportions and Student’s t-test to evaluate differences in means. We used logistic regression modeling to compare mortality in DT and IT patients. All variables that were significantly associated with mortality in bivariate analysis were initially eligible for inclusion in the model. In order to create a more parsimonious final model, we then excluded variables that did not significantly contribute.
To evaluate how the relationship between transfer status and mortality varies with age, we calculated adjusted predicted probabilities of mortality by age and transfer status. For this calculation, we used a modified MTS which excluded age so that we would not account for age twice (once in the MTS and once as its own variable). Otherwise, we used the same variables that were in the final logistic regression model. Lastly, we used the final model to perform a sensitivity analysis in which we included patients who arrived alive but died prior to admission.
We performed all data analysis using STATA (release 16, College Station, TX: StataCorp LLC). The Malawi National Health Research Committee and the University of North Carolina approved this study.
Results
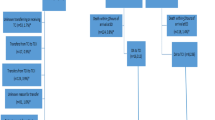
A total of 76,251 trauma patients presented to the KCH emergency department between January 1, 2013, and May 30, 2018. We excluded patients discharged from the emergency department (ED, n = 45,836), patients under 12 years of age (n = 20,534), patients who were brought in dead (876), patients who died in the ED (277), and patients who were missing primary exposure or outcome data (n = 359). The final study cohort, therefore, included 8,369 patients (Fig. 1). Of these, 4,196 (50.1%) were direct transfers (DT) and 4173 (49.9%) were indirect transfers (IT).

Flow diagram of patients included in study
Patient and injury characteristics are provided in Table 1. The majority of patients (81%) were male, and the average age was 34.6 years (SD 15.8). Patients in the DT group were more likely to be male (82.7% vs. 79.4%, p < 0.001) and were younger than patients in the IT group (mean age 33.5 (SD 14.1) vs. 35.6 (SD 17.3) years, p < 0.001). The most common mechanism of injury in the IT group and the overall cohort was motor vehicle collision (MVC); the most common mechanism in the DT group was assault. The most common injury locations in both groups were extremities followed by head injuries. Patients in the IT group were significantly more likely to be transported by emergency vehicles than were patients in the DT group (73.53% vs. 16.97%, p < 0.001). Patients in the IT group also took significantly longer to arrive at KCH than patients in the DT group (mean 3.57 days vs. 0.88 days, p < 0.001).
Mortality was higher in the IT group than in the DT group (4.8% vs. 2.6%). Factors significantly associated with mortality on the bivariate analysis included older age, head injury, lower GCS on arrival, shorter time from injury to arrival, higher MTS, surgical intervention, chest tube placement, emergency vehicle transport, and mechanism of injury (pedestrian struck by a vehicle, GSW, and burns) (Table 2). The unadjusted odds ratio of mortality in the IT group compared to the DT group was 1.86 (1.47–2.36, p < 0.001). We included the following variables in the final adjusted logistic regression model: mechanism of injury, location of primary injury, MTS, and operative intervention (Table 3). We did not include age separately in the model as it is a component of the MTS. Time from injury to arrival, initial GCS, and chest tube placement were excluded because they did not significantly contribute to the model. We also excluded transport mode from the final model as it was found to be an effect measure modifier rather than a confounder. The adjusted odds ratio of mortality in the IT versus the DT group was 2.12 (1.49–3.02, p < 0.001). Predicted probabilities of mortality by age and transfer status demonstrate that the survival benefit associated with DT remained relatively stable regardless of age (Fig. 2). However, unsurprisingly, probability of mortality increased with older age for both cohorts.

Predicted probability of mortality by transfer status and age *adjusted for modified mts, mechanism of injury, location of injury, and operative intervention
The sensitivity analysis included the original cohort as well as patients who arrived at the emergency department alive but died prior to admission. In this analysis, the unadjusted OR of mortality among IT versus DT patients was 1.08 (0.91–1.29, p = 0.370). When the final model described above was used, OR was 1.51 (1.14–2.01, p = 0.004).
Discussion
The defined purpose of organized trauma systems is to ensure the expeditious transfer of seriously injured patients to the facility best equipped to care for their injuries. In this study, we evaluated the relationship between transfer status and in-hospital mortality in a resource-limited setting. Our results showed that IT patients had significantly higher crude mortality than DT patients and over twice the adjusted odds of mortality. When patients who arrived alive but died prior to admission were included in the cohort, the adjusted OR fell to 1.51 but remained statistically significant. Though IT patients arrived at KCH an average of 2.69 days later than DT patients, a longer time from injury to arrival was not associated with a higher risk of mortality.
The higher mortality rate among IT patients confirms our hypothesis but conflicts with two previous meta-analyses on this topic. Hill et al. found that IT patients had significantly longer times to definitive care and longer hospital and ICU length of stay, but mortality rates did not significantly differ from those of DT patients (pooled OR 1.1, 95% CI 0.9–1.3) [4]. Williams et al. found a nonsignificantly reduced mortality risk in the IT group compared to the DT group (pooled OR 0.9, 95% CI 0.7–1.1) [5]. However, both of these reviews included almost exclusively studies performed in HICs.
Conversely, several studies performed in LMICs reported results similar to ours. For example, Dharap et al. found that the adjusted odds ratio of mortality in IT versus DT trauma patients in India was 1.87 (95% CI 1.2–2.6, p = 0.005) [11]. Studies from South Africa and Nigeria have reported a significant survival advantage among DT patients as well [12, 13]. The relationship between transfer status and trauma mortality has also been previously evaluated using the KCH trauma registry. Boschini et al. performed a logistic regression to assess mortality rates by transfer status among patients admitted to KCH between 2008 and 2012 [14]. Adjusted odds ratio of mortality in IT versus DT patients was 2.09.
The discrepancy between our results and those of studies conducted in HICs reflects the relative immaturity of Malawi’s trauma system. Malawi does not have formal prehospital care, and most trauma patients seek care at the facility nearest to them. Often this will be a primary or a district hospital that lacks the infrastructure, workforce, and equipment to manage traumatic injuries. Strengthening the prehospital system will allow for resuscitation before arrival at a healthcare facility and direct transfer to a trauma center when appropriate. A systematic review and meta-analysis in developing countries found that the presence of prehospital systems reduced the risk of trauma mortality by 25% [15]. In addition, assessing and building capacity for initial trauma management at district hospitals will allow for stabilization of life-threatening injuries and more efficient transfer. Provider education alone has been found to improve the utilization of initial trauma management procedures, including airway maneuvers and chest tube insertion [16].
Malawi also currently lacks trauma transfer protocols, and many of the patients transferred from district hospitals to KCH are overtriaged [17]. Maine et al. found that over 50% of patients transferred from a district hospital to KCH for trauma care were discharged within 48 h without undergoing a procedure [17]. Moreover, nearly 90% of these overtriaged patients were discharged from the ED [17]. The development of transfer protocols can reduce rates of overtriage and undertriage, thereby improving care without overburdening busy referral hospitals.
To inform the development of trauma transfer protocols and monitor their effectiveness, we must also understand the characteristics and outcomes of potential transfers. These are patients who reached a primary or district hospital but died before transfer. They are termed potential transfers as they likely would have been transferred to a trauma center had they survived long enough. However, these patients never reach a referral hospital and are therefore generally not included in IT cohorts. Not including potential transfers when comparing IT and DT patients introduce a survival bias in favor of IT patients. This survival bias has been described by studies from Canada [18] and South Africa [19] and is likely also demonstrated by the results of our sensitivity analysis. Including potential transfers in future studies will lead to a more comprehensive understanding of trauma systems and may be accomplished through the development of regional or even country-wide rather than hospital-specific trauma registries.
This study has several limitations. The primary data analysis of the KCH trauma registry is limited by its retrospective observational design. It is possible that additional confounders which were unmeasured and therefore not studied affected our findings. For example, we were unable to account for patients who may have left the ED against medical advice as these patients are included with discharged patients in the trauma registry. These patients may be at higher risk for adverse outcomes as compared to those who are formally discharged. Lastly, as is the case with most studies on this topic, we could not account for patients initially seen at district hospitals and never transferred to KCH. Studying this non-transferred cohort in the future would provide meaningful information about the characteristics of patients who initially present to district hospitals. Combining this with knowledge about patients treated at KCH would also allow for the calculation of overtriage and undertriage rates.
Conclusion
This study suggests that direct transfer of trauma patients to a referral hospital in Malawi is associated with a survival benefit compared to indirect transfer. This finding is attributed to multiple factors, including limited prehospital care, inadequate treatment at non-referral hospitals, lack of coordination between emergency medical services and health care facilities, and lack of transfer protocols. Improving outcomes for trauma patients in Malawi will best be accomplished by addressing all of the contributing factors and strengthening the trauma system as a whole. Future research should focus on including non-transferred patients to fully understand the state of trauma care in LMICs and make informed recommendations for transfer protocols.
References
GBD 2019 Diseases and Injuries Collaborators (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396(10258):1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
World Health Organization. Injuries and violence: the facts. WHO. Published online 2014:20. http://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/
Mock C, Joshipura M, Arreola-Risa C, Quansah R (2012) An estimate of the number of lives that could be saved through improvements in trauma care globally. World J Surg 36(5):959–963. https://doi.org/10.1007/s00268-012-1459-6
Hill AD, Fowler RA, Nathens AB (2011) Impact of interhospital transfer on outcomes for trauma patients: a systematic review. J Trauma - Inj Infect Crit Care 71(6):1885–1900. https://doi.org/10.1097/TA.0b013e31823ac642
Williams T, Finn J, Fatovich D, Jacobs I (2013) Outcomes of different health care contexts for direct transport to a trauma center versus initial secondary center care: a systematic review and meta-analysis. Prehospital Emerg Care 17(4):442–457. https://doi.org/10.3109/10903127.2013.804137
World Bank. World development indicators. Published 2021. https://data.worldbank.org/country/MW
Mulwafu W, Chokotho L, Mkandawire N et al (2017) Trauma care in Malawi: a call to action. Malawi Med J 29(2):198–202. https://doi.org/10.4314/mmj.v29i2.23
Lavy C, Tindall A, Steinlechner C, Mkandawire N, Chimangeni S (2007) Surgery in Malawi - a national survey of activity in rural and urban hospitals. Ann R Coll Surg Engl 89(7):722–724. https://doi.org/10.1308/003588407X209329
Gallaher J, Jefferson M, Varela C, Maine R, Cairns B, Charles A (2019) The Malawi trauma score: a model for predicting trauma-associated mortality in a resource-poor setting. Injury 50(9):1552–1557. https://doi.org/10.1016/j.injury.2019.07.004
Grudziak J, Gallaher J, Banza L et al (2017) The effect of a surgery residency program and enhanced educational activities on trauma mortality in Sub-Saharan Africa. World J Surg 41(12):3031–3037. https://doi.org/10.1007/s00268-017-4272-4
Dharap SB, Kamath S, Kumar V (2017) Does prehospital time affect survival of major trauma patients where there is no prehospital care? J Postgrad Med 63(3):169–175. https://doi.org/10.4103/0022-3859.201417
Kong VY, Bruce JL, Sartorius B et al (2019) Civilian cerebral gunshot wounds in rural South African patients are associated with significantly higher mortality rates than in urban patients. Eur J Trauma Emerg Surg Off Publ Eur Trauma Soc 45(1):145–150. https://doi.org/10.1007/s00068-017-0800-z
Ahidjo KA, Olayinka SA, Ayokunle O, Mustapha AF, Sulaiman GAA, Gbolahan AT (2011) Prehospital transport of patients with spinal cord injury in Nigeria. J Spinal Cord Med 34(3):308–311. https://doi.org/10.1179/107902610X12883422813624
Boschini LP, Lu-Myers Y, Msiska N, Cairns B, Charles AG (2016) Effect of direct and indirect transfer status on trauma mortality in sub Saharan Africa. Injury 47(5):1118–1122. https://doi.org/10.1016/j.injury.2016.01.015
Henry JA, Reingold AL (2012) Prehospital trauma systems reduce mortality in developing countries: a systematic review and meta-analysis. J Trauma Acute Care Surg 73(1):261–268. https://doi.org/10.1097/TA.0b013e31824bde1e
Mock CN, Quansah R, Addae-Mensah L, Donkor P (2005) The development of continuing education for trauma care in an African nation. Injury 36(6):725–732. https://doi.org/10.1016/j.injury.2004.12.044
Maine RG, Kajombo C, Mulima G et al (2020) Secondary overtriage of trauma patients to a central hospital in Malawi. World J Surg 44(6):1727–1735. https://doi.org/10.1007/s00268-020-05426-0
Haas B, Gomez D, Zagorski B, Stukel TA, Rubenfeld GD, Nathens AB (2010) Survival of the fittest: the hidden cost of undertriage of major trauma. J Am Coll Surg 211(6):804–811. https://doi.org/10.1016/j.jamcollsurg.2010.08.014
Cheddie S, Muckart DJJ, Hardcastle TC, den Hollander D, Cassimjee H, Moodley S (2011) Direct admission versus inter-hospital transfer to a level I trauma unit improves survival: an audit of the new Inkosi Albert Luthuli central hospital trauma unit. South African Med J 101(3):176–178. https://doi.org/10.7196/samj.4170
Acknowledgments
We would like to thank Dr. Gift Mulima and Dr. Chifundo Kajombo for their assistance with this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yohann, A., Kayange, L., Purcell, L.N. et al. Direct Transfer to a Tertiary Care Hospital After Traumatic Injury is Associated with a Survival Benefit in a Resource-Limited Setting. World J Surg 46, 504–511 (2022). https://doi.org/10.1007/s00268-021-06415-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-021-06415-7