
Abstract
Background
Surgical resection in patients with extrahepatic cholangiocarcinoma (EHCC) with paraaortic lymph node metastasis (PALNM) remains controversial. The objective of this study was to investigate the prognostic impact of PALNM in resected EHCC.
Methods
The present retrospective study included 410 patients, including 16 patients with PALNM, who underwent surgical resection of EHCC between September 2002 and December 2018. These were compared to 9 patients in whom EHCC was not resected due to PALNM. The clinicopathological features and survival outcomes were investigated to identify the prognostic factors in resected EHCC.
Results
The overall survival in the resected patients with PALNM was significantly better than that in unresected patients (median survival time [MST] 33.7 vs. 16.7 months, p=0.009) and was not significantly worse than that of patients with regional lymph node metastasis (LNM) (MST 33.7 vs 36.0 months, p=0.278). The multivariate analysis identified age > 70 years, male sex, tumor location (perihilar), residual tumor status, histological grade, microscopic venous invasion, and regional LNM as independent prognostic factors.
Conclusions
There was no significant difference in survival between the resected patients with PALNM and patients with regional LNM, and PALNM was not a significant prognostic factor in the multivariate analysis. Surgical resection may be considered an acceptable approach for EHCC with PALNM in selected patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cholangiocarcinoma most commonly occurs in Asian countries, and the prevalence and number of deaths due to cholangiocarcinoma are increasing [1, 2]. Surgical resection for extrahepatic cholangiocarcinoma (EHCC, including perihilar and distal cholangiocarcinoma) only offers the chance of cure. However, the survival outcomes of patients with EHCC remains poor due to prognostic factors such as nodal metastasis [3,4,5,6] or positive resection margins [4,5,6]. The rate of regional lymph node metastasis (LNM) in EHCC was reported to be 40–53% [3,4,5, 7], and LNM has been established as a critical prognostic factor [3,4,5,6]. Although the relationships between the number of LNMs, site, metastasis rate, and prognosis have been reported, the best strategy for EHCC with LNM is still unclear [5] [8].
The paraaortic lymph nodes (PALNs) are the final nodes in the abdominal lymphatic system from the biliary duct [9, 10]. Paraaortic lymph node metastasis (PALNM) is associated with a poor prognosis [7] and corresponds to distant metastasis (M1) in the TNM classification [11]. However, some previous studies reported long-term survival, even in cholangiocarcinoma patients with PALNM [3] [7]. Intraoperative sampling of the PALNs in laparotomy becomes the last resort for the diagnosis of PALNM, because preoperative imaging studies are not sufficiently sensitive for the diagnosis of PALNM [12]. Although the feasibility of PALN sampling by laparoscopy was reported in recent study [13], the usefulness of staging laparoscopy in EHCC is unclear, and laparoscopic sampling of PALNs is not generally acceptable. The indication of surgical resection for the patients in whom PALNM is intraoperatively diagnosed in EHCC is controversial. Although the prognostic impact of PALNM was reported in some previous studies [3] [14] [15], they included other types of biliary tract cancer, which have different survival outcomes [16, 17]. There is little established evidence on surgical resection for patients with PALNM in pure EHCC.
The present study retrospectively evaluated the clinicopathological features and long-term outcomes in EHCC patients after resection in order to investigate the prognostic impact of PALNM.
Methods
Patients
A retrospective review was conducted using a prospectively collected database of 418 patients who underwent surgical resection for EHCC in Shizuoka Cancer Center between September 2002 and December 2018. Among these, 8 cases with data missing were excluded. The remaining 410 patients were included in the analyses. Nine patients in whom the tumor was unresected because laparotomy revealed PALNM were included in the unresectable (UR) group. The present study was approved by the institutional review board of the Shizuoka Cancer Center (Number J2019-179–2019-1–3), and the need for patient consent was waived because of its retrospective nature.
The preoperative evaluation and surgical procedures
The preoperative assessment to determine the tumor status, resectability, and surgical planning was performed using multidetector-row computed tomography (MDCT), ultrasonography, and cholangiography via either an endoscopic or percutaneous transhepatic procedure. Other imaging approaches, including magnetic resonance imaging and positron emission tomography, were performed in selected patients when needed [18]. Patients with obviously swollen or bed-shaped PALN on preoperative imaging were diagnosed with massive PALNM and were not considered candidates for surgical resection.
On laparotomy, PALNs were routinely sampled from the aortocaval lymphatic tissue located below the left renal vein and intraoperatively examined by frozen section. In our institution, a positive result of frozen PALN was not a contraindication for surgical resection. Surgeons made the decision to perform surgical resection with consideration of tumor extension and patients’ general condition. Systematic dissection of PALN was not usually performed. Our standard surgical procedures for EHCC, which include hepatobiliary resection, pancreatoduodenectomy (PD), and hepato-pancreatoduodenectomy (HPD), were reported in our previous reports [18,19,20]. Combined vascular resection and reconstruction were performed depending on the tumor extension [18]. When frozen sections of bile duct margin were positive, additional resection, including bile duct resection, hepatectomy, or PD, was considered.
The histopathological evaluation
All specimens were prepared in the usual manner for a microscopic examination with hematoxylin–eosin staining. The pathological findings were reported by an experienced pathologist (K.S) according to the Japanese standardized rules for biliary tract cancers [21], and TNM classifications were relabeled according to the UICC TNM classification (8th edition) [11]. Histological grade, lymphatic invasion, microscopic venous invasion (MVI), perineural invasion, arterial invasion, portal vein invasion, regional LNM, and PALNM were reported. N Category was classified according to the UICC grading system [11]: pN0, no regional LNM; pN1, metastasis in 1–3 regional lymph nodes; and pN2, metastasis in 4 or more regional lymph nodes. The residual tumor status (R) at the surgical margins was defined as follows: R0, no residual tumor cell or carcinoma in situ at the ductal margin; R1, invasive carcinoma at the ductal stump or exfoliation margin.
Follow-up and definition of recurrence
In principle, adjuvant chemotherapy was not performed for patients who received R0 resection, with the exception of patients who participated in some clinical trials [22, 23]. Patients who underwent with R1 resection or resection with PALNM generally received adjuvant therapy. Unresected patients with PALNM received systemic chemotherapy, if appropriate. Follow-up examinations, including laboratory tests, measurement of tumor markers, and CT, were conducted at 3–6-month intervals. Tumor recurrence was confirmed based on radiological findings or histological evidence. Patients with recurrent disease underwent systemic chemotherapy, if appropriate.
Statistical analyses
All continuous variables were expressed as the median and range. Fisher’s exact test was used for comparisons between the categorical variables. The Mann–Whitney U-test was used for comparisons between continuous variables. Overall survival (OS) rates were analyzed using the Kaplan–Meier method, and the log-rank test was used to evaluate statistical significance. The cutoff value for age was determined based on the minimum p value approach. The cutoff values for the carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19–9 levels were decided by the upper limit of the institutional standard levels (CEA > 5.0 ng/mL, CA19–9 > 37 U/mL). Variables with a p value of <0.05 in a univariate analysis were included in a multivariate Cox proportional hazards regression analysis to identify prognostic factors for OS. P values of <0.05 were considered to indicate statistical significance. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [24].
Results
The clinicopathological features of the resected patients
Table 1 shows the clinicopathological features of the 410 resected patients with EHCC.
PALNs in 63 patients were not examined pathologically, because no PALNs were found intraoperatively or the sampled specimen contained no lymph nodes. PALNM was identified in 16 (3.9%) patients (7 with perihilar cholangiocarcinoma and 9 with distal cholangiocarcinoma). The median number of PALNM lesions was 1 (range 1–11). Among them, 12 patients were diagnosed based on the intraoperative frozen section examinations, and 4 patients were diagnosed based on the postoperative re-examinations of paraffinized specimens, despite the negative results of frozen specimens. Four patients with PALNM underwent systemic PALN dissection at the surgeons’ discretion, and no patient without PALNM underwent systemic PALN dissection. All 16 patients with PALNM had regional LNM: pN1 (n=5), pN2 (n=11). Regarding the rate of postoperative complications (Clavien–Dindo > grade IIIa [25]), there was no significant difference between the resected patients without PALNM and those with PALNM (62% vs. 56%, p=0.794). All 10 patients with postoperative mortality were included among the patients without PALNM.
Postoperative (adjuvant) therapy and treatment after recurrence
Among the 16 resected patients with PALNM, 11 (69%) underwent adjuvant therapy as follows: gemcitabine-based chemotherapy (n=8), S-1-based chemotherapy (n=2), or fluorouracil with radiotherapy (n=1). Among the remaining 394 patients, 54 (14%) patients underwent adjuvant chemotherapy as follows: chemoradiotherapy (n=24), S-1 (n=15), gemcitabine (n=6), or others (n=9).
Recurrence was found in 207 (50%) patients. Chemotherapy or radiotherapy after recurrence was performed for 117 patients, whereas 15 underwent resection for recurrent disease, 62 received no anticancer treatment, and 13 were lost to follow-up. In the 9 UR patients, 6 patients underwent gemcitabine-based chemotherapy, 1 patient underwent S-1, and 2 patients did not receive chemotherapy.
The survival outcomes and prognostic factors
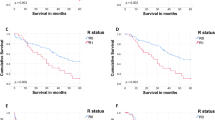
The median follow-up period was 50.7 (1.9–195.3) months for the censored cases. Figure 1a shows the OS rates of 394 resected patients without PALNM, 16 resected patients with PALNM, and 9 patients in the UR group. The OS in the resected patients with PALNM was significantly worse than that in patients without PALNM (median survival time [MST] 33.7 vs. 56.0 months, p=0.010) and was significantly better than that in the UR group (MST 33.7 vs. 16.7 months, p=0.009). Two patients with PALNM survived for 5 years after resection, whereas no patient in the UR group survived for more than 3 years after surgery. Figure 1b shows the OS rates according to pN classification. The OS in the patients with pN1 (MST 39.8 months) or pN2 (MST 27.9 months) was not significantly different to that in patients with PALNM (pN1 vs. PALNM, p=0.168, pN2 vs. PALNM, p=0.895).

a Kaplan–Meier curves for overall survival in 384 resected patients without paraaortic lymph node metastasis (PALNM), 16 resected patients with PALNM, and 9 unresected patients. b Kaplan–Meier curves for overall survival according to pN classification. PALNM, paraaortic lymph node metastasis, R-LNM regional lymph node metastasis.
Table 2 shows the results of univariate and multivariate analyses to identify the prognostic factors for OS in 410 resected patients. The multivariate analysis identified an age > 70 years, male sex, tumor location (perihilar), residual tumor status (R1), histological grade (other than well-differentiated adenocarcinoma), MVI, and regional LNM as independent prognostic factors. In the multivariate analysis, PALNM was not an independent prognostic factor for OS in patients with EHCC.
The association between recurrence patterns
Table 3 shows the clinicopathological features and patterns of recurrence between resected patients with pN0, regional LNM, and PALNM. The rate of MVI in patients with PALNM (75%) was significantly higher than that in patients with pN0 (33%, p=0.002) and tended to be higher than that in patients with regional LNM (51%, p=0.071). The rate of lymph node recurrence in the patients with PALNM (56%) was significantly higher than that in patients with pN0 (4.2%, p<0.001), and that in patients with regional LNM (19%, p=0.003).
Details of resected and UR patients with PALNM
Table 4 shows the clinical features and survival outcome in patients with PALNM. Among the 16 resected patients, 3 underwent HPD, and 2 underwent left or right trisectionectomy with caudate lobectomy. All resected patients were < 80 years old, and there were no cases of combined vascular resection. Among the 9 unresected patients, 4 were planned to receive HPD, and 3 were planned to receive left trisectionectomy with combined vascular resection. Two unresected patients who were planned to receive PD were over 80 years old. The rate of comorbidities (including hypertension, diabetes mellitus, and heart disease) in the resected patients with PALNM was not significantly different from that in the UR patients (38% vs. 33%, p=1.000). The indocyanine green retention rates at 15 min in the resected patients with PALNM were not significantly different from that in the UR patients (10.9% [7.0–16.0] vs. 16.5% [8.7–23.0], p=0.175), and the future liver remnant volume in the resected patients with PALNM was also not significantly different from that in the UR patients (445 [371–918] ml vs. 515 [253–857] ml, p=0.852).
Discussion
The present study aimed to investigate the prognostic impact of PALNM in patients with resected EHCC. The results showed that the OS in resected patients with PALNM was significantly better than that in the UR group, and 2 patients with PALNM survived for 5 years after resection. There was no significant difference between the OS in resected patients with PALNM and the OS in patients with regional LNM. PALNM was not a significant prognostic factor in the multivariate analysis. Surgical resection may therefore be considered acceptable for EHCC patients with PALNM in selected cases.
Surgical resection for patients with PALNM has been controversial in other carcinomas, and there have been reports of a relatively good survival with surgical resection [26,27,28]. In biliary carcinoma, some previous studies showed that survival of the patients with PALNM was comparable to that of the patients with regional LNM [3] [14], which is indicated for surgical resection. PALNM was not reported as an independent prognostic factor in previous reports [3] [29], as with the current study. In addition, Kitagawa et al. [7] reported that 2 cases with PALNM survived for more than 5 years and the 5-year survival rate of patients with PALNM was 12.3%. The 5-year survival rate in resected patients with PALNM was 16.2% in the present study, and their OS was significantly better than that in the UR group. There have been no reports comparing the survival outcomes of resected and unresected patients with PALNM in EHCC. This study may suggest the efficacy of surgical resection for EHCC with PALNM, except for cases of tumor with massive PALNM that are preoperatively diagnosed.
Although the OS in patients with PALNM was not significantly worse than that in patients with regional LNM, the survival outcome was unsatisfactory as with that in pN2 patients. The current study showed that the rates of lymph node recurrence and MVI, which was identified as an independent prognostic factor, were extremely high in patients with regional LNM and PALNM. These results may suggest the difficulty in controlling micrometastasis via lymphovascular system only by surgery. Although 2 of 4 patients with systemic PALN dissection survived for 5 years after resection in the current study, the survival benefit of systemic PALN dissection in EHCC remains unclear [7]. It is thus necessary to develop effective perioperative chemotherapy to improve the survival of EHCC patients with extensive LNM. However, the evidence to support adjuvant chemotherapy for biliary duct carcinoma is poor. All 4 randomized controlled trials on adjuvant chemotherapy failed to show a survival benefit [22, 30,31,32], and an optimal regimen remains to be unestablished. Two ongoing randomized phase III trials of adjuvant chemotherapy for patients with biliary tract cancer are expected to improve survival outcomes [23] [33].
In the present study, the resected patients with PALNM underwent postoperative chemotherapy in principle. The indication for surgical resection should be determined based on whether or not patients with PALNM would have good chance of receiving chemotherapy after surgery. Elderly patients or those with serious comorbidities were thus considered ineligible for resection. Patients who had needed highly invasive surgery such as extended hepatectomy with vascular resection and reconstruction were also considered ineligible for surgical resection. Sampling of PALN may be useful for determining surgical indications for fragile patients who are unable to receive postoperative chemotherapy.
The present study was associated with some limitations, including its retrospective nature and single-institution setting with a limited number of patients with PALNM. Another limitation was that the frequency of PALNM might have been underestimated, as PALNM was only assessed by sampling and not lymph node dissection. Patients with locally advanced EHCC who needed to undergo HPD or combined vascular resection might have been deemed unresectable when the intraoperative sampled PALNs were positive for cancer. This might have led to selection bias concerning surgical resection in patients with PALNM. The subjects in the present study were only patients who had been diagnosed intraoperatively, as the patients with massive PALNM detected on preoperative imaging were excluded.
In conclusion, the survival of patients with resected PALNM was significantly better than that of the UR group. There was no significant difference in OS between resected patients with PALNM and patients with regional LNM. Although established adjuvant chemotherapy is expected to develop, surgical resection may be acceptable for selected patients with PALNM.
References
Randi G, Malvezzi M, Levi F et al (2009) Epidemiology of biliary tract cancers: an update. Ann Oncol 20:146–159
Florio AA, Ferlay J, Znaor A et al (2020) Global trends in intrahepatic and extrahepatic cholangiocarcinoma incidence from 1993 to 2012. Cancer 126(11):2666–2678
Murakami Y, Uemura K, Sudo T et al (2011) Is para-aortic lymph node metastasis a contraindication for radical resection in biliary carcinoma? World J Surg 35:1085–1093. https://doi.org/10.1007/s00268-011-1036-4
Nagino M, Ebata T, Yokoyama Y et al (2013) Evolution of surgical treatment for perihilar cholangiocarcinoma: a single-center 34-year review of 574 consecutive resections. Ann Surg 258:129–140
Kiriyama M, Ebata T, Aoba T et al (2015) Prognostic impact of lymph node metastasis in distal cholangiocarcinoma. Br J Surg 102:399–406
DeOliveira ML, Cunningham SC, Cameron JL et al (2007) Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 245:755–762
Kitagawa Y, Nagino M, Kamiya J et al (2001) Lymph node metastasis from hilar cholangiocarcinoma: audit of 110 patients who underwent regional and paraaortic node dissection. Ann Surg 233:385–392
Aoba T, Ebata T, Yokoyama Y et al (2013) Assessment of nodal status for perihilar cholangiocarcinoma: location, number, or ratio of involved nodes. Ann Surg 257:718–725
Hirono S, Tani M, Kawai M et al (2012) Identification of the lymphatic drainage pathways from the pancreatic head guided by indocyanine green fluorescence imaging during pancreaticoduodenectomy. Dig Surg 29:132–139
Uesaka K, Yasui K, Morimoto T et al (1996) Visualization of routes of lymphatic drainage of the gallbladder with a carbon particle suspension. J Am Coll Surg 183:345–350
Brierley JD, Gospodarowicz M, Wittekind C (2016) UICC TNM classification of malignant tumours, 8th edn. Wiley Black-well, New York
Noji T, Kondo S, Hirano S et al (2005) CT evaluation of paraaortic lymph node metastasis in patients with biliary cancer. J Gastroenterol 40:739–743
Schwarz L, Tortajada P, Pittau G et al (2019) “Laparoscopic para-aortic lymph node sampling” first approach for pancreatic adenocarcinoma as an oncological practice. J Laparoendosc Adv Surg Tech A 29(7):900–904
Gu J, Xia L, Xu B et al (2016) Clinical prognostic significance of regional and extended lymphadenectomy for biliary cancer with para-aortic lymph node metastasis: a systematic review and meta-analysis. Dig Liver Dis 48:717–725
Yonemori A, Kondo S, Matsuno Y et al (2009) Prognostic impact of para-aortic lymph node micrometastasis in patients with regional node-positive biliary cancer. Br J Surg 96:509–516
Flemming JA, Zhang-Salomons J, Nanji S et al (2016) Increased incidence but improved median overall survival for biliary tract cancers diagnosed in Ontario from 1994 through 2012: a population-based study. Cancer 122:2534–2543
Kim BW, Oh CM, Choi HY et al (2019) Incidence and overall survival of biliary tract cancers in South Korea from 2006 to 2015: using the national health information database. Gut Liver 13:104–113
Sugiura T, Okamura Y, Ito T et al (2019) Left hepatectomy with combined resection and reconstruction of right hepatic artery for bismuth type I and II perihilar cholangiocarcinoma. World J Surg 43:894–901. https://doi.org/10.1007/s00268-018-4833-1
Uesaka K (2012) Left hepatectomy or left trisectionectomy with resection of the caudate lobe and extrahepatic bile duct for hilar cholangiocarcinoma (with video). J Hepatobiliary Pancreat Sci 19:195–202
Ohgi K, Sugiura T, Yamamoto Y et al (2016) Bacterobilia may trigger the development and severity of pancreatic fistula after pancreatoduodenectomy. Surgery 160:725–730
Miyazaki M, Ohtsuka M, Miyakawa S et al (2015) Classification of biliary tract cancers established by the Japanese society of hepato-biliary-pancreatic surgery: 3rd english edition. J Hepatobiliary Pancreat Sci 22:181–196
Ebata T, Hirano S, Konishi M et al (2018) Randomized clinical trial of adjuvant gemcitabine chemotherapy versus observation in resected bile duct cancer. Br J Surg 105:192–202
Nakachi K, Konishi M, Ikeda M et al (2018) A randomized phase III trial of adjuvant S-1 therapy vs. observation alone in resected biliary tract cancer: Japan clinical oncology group study (JCOG1202, ASCOT). Jpn J Clin Oncol 48:392–395
Kanda Y (2013) Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl 48:452–458
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Schwarz L, Lupinacci RM, Svrcek M et al (2014) Para-aortic lymph node sampling in pancreatic head adenocarcinoma. Br J Surg 101:530–538
Paiella S, Sandini M, Gianotti L et al (2016) The prognostic impact of para-aortic lymph node metastasis in pancreatic cancer: a systematic review and meta-analysis. Eur J Surg Oncol 42:616–624
Nakai N, Yamaguchi T, Kinugasa Y et al (2017) Long-term outcomes after resection of para-aortic lymph node metastasis from left-sided colon and rectal cancer. Int J Colorectal Dis 32:999–1007
Nomura T, Tsuchiya Y, Nashimoto A et al (2009) Prognostic factors for radical resection of middle and distal bile duct cancer. Hepatogastroenterology 56:294–298
Neoptolemos JP, Moore MJ, Cox TF et al (2012) Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: the ESPAC-3 periampullary cancer randomized trial. JAMA 308:147–156
Primrose JN, Fox RP, Palmer DH et al (2019) Capecitabine compared with observation in resected biliary tract cancer (BILCAP): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol 20:663–673
Edeline J, Benabdelghani M, Bertaut A et al (2019) Gemcitabine and oxaliplatin chemotherapy or surveillance in resected biliary tract cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): a randomized phase III study. J Clin Oncol 37:658–667
Stein A, Arnold D, Bridgewater J et al (2015) Adjuvant chemotherapy with gemcitabine and cisplatin compared to observation after curative intent resection of cholangiocarcinoma and muscle invasive gallbladder carcinoma (ACTICCA-1 trial) - a randomized, multidisciplinary, multinational phase III trial. BMC Cancer 15:564
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
The study was approved by the Institutional Research ethics committee.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nitta, N., Ohgi, K., Sugiura, T. et al. Prognostic Impact of Paraaortic Lymph Node Metastasis in Extrahepatic Cholangiocarcinoma. World J Surg 45, 581–589 (2021). https://doi.org/10.1007/s00268-020-05834-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05834-2