
Abstract
Introduction
Chronic subdural hematoma (cSDH) is a common condition that causes significant morbidity and mortality. In rural sub-Saharan Africa, there are very few neurosurgeons. Yet, cSDH is treatable by relatively simple surgical intervention with potential for rapid clinical improvement.
Methods
We conducted a retrospective chart review of all patients with cSDH who underwent burr-hole trephination at Tenwek Hospital, Kenya, between July 2014 and July 2016. We extracted and compared the clinical presentation, risk factors, operative details, and outcomes.
Results
A total of 119 patients were identified with a mean age of 61.3 years. The majority were men (80%). The main predisposing factors were trauma (54.6%) and alcohol intake (34.4%). Patients were generally managed with two burr-holes, irrigation, and a subdural drain, remaining for a median of 2 days. Operations were assisted by general surgery residents under direct supervision of senior residents (46), general surgeons (65), and neurosurgeons (8). Complications included recurrence (5.2%), subdural empyema (2.5%), postoperative seizures (3.4%), and mortality (6.7%). Improvement of symptoms was noted in 91% of all patients.
Conclusion
Operative management of cSDH can be safely performed in rural facilities by general surgeons familiar with the procedure and with the institutional resources. The majority of patients had satisfactory outcomes.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Burr-hole craniostomy, trepanation or trephination, is perhaps one of the oldest known surgical procedures [1]. Prehistoric evidence exists that trepanation has been widely used by many societies, including communities within Kenya [2]. In more recent eras, surgical drainage of chronic subdural hematoma (cSDH) has been a preserve of the neurosurgeon with good results. In Kenya, the main neurosurgical referral centers, in Nairobi and Eldoret—far from rural areas, claim to manage 90% of the neurosurgical cases [3]. Yet, significant trauma occurs in rural areas [4]. To deal with this high burden of trauma, there is one neurosurgeon for every five million people in sub-Saharan Africa [5].
Subdural hematoma is a collection of blood between the inner layer of the dura but external to the brain and arachnoid membranes. The development of cSDH arises at the dural border cell layer and may be precipitated by an unresolved acute subdural hematoma or a subdural hygroma [6]. For cSDH, surgical evacuation is the mainstay of treatment for patients with symptoms or significant mass effect and burr-hole craniostomy is the gold standard with the best cure-to-complication ration [6], although there are some reports of spontaneous resolution [7, 8]. Treatment is commonly performed by a neurosurgeon with two-hole burr-hole craniostomy or twist-drill craniostomy [9, 10] with or without irrigation [10, 11] and drainage, all with favorable outcomes [12].
Despite the significant history of trepanation and the incidence of cSDH in places with limited options for treatment, few reports exist on general surgeons safely performing drainage of cSDH. One such study from Australia [13] reports successful outcomes from general surgeons located in rural areas. Additionally, Phang et al. [14] reported that cSDH can be managed effectively by neurosurgical trainees with similar outcomes as their seniors. There have been some recent efforts to improve neurosurgical education in low- and middle-income countries (LMICs) [15,16,17]. Yet, there is debate on whether general surgeons and medical officers should be involved in neurosurgical care [5, 18]. The aim of this study was to determine whether burr-hole craniostomy can be safely performed in a rural, resource-limited setting [19] with acceptable outcomes in the management of cSDH.
Methods
We conducted a retrospective review of patients diagnosed and treated for chronic subdural hematomas in Tenwek Hospital, Bomet County, Kenya, over a period of 2 years from July 2014 to July 2016. Approval for the study was obtained from the Tenwek Hospital Ethics Committee. Cases were identified by reviewing all patients who had a discharge diagnosis of chronic subdural hematoma. All patients who underwent burr-hole craniostomy during the time period were included for the analysis. Charts were reviewed in the institutional electronic medical record and surgical resident operative case log system. The diagnosis was confirmed on computerized tomography (CT) scan imaging after clinical diagnosis based on a variety of presenting signs and symptoms. Operative management is with two burr-holes on a given side with cSDH and irrigation with normal saline. To reduce postoperative recurrence, we also typically utilize postoperative drainage [10, 20, 21]. Data extracted from the individual case records and analyzed included the patient’s age, gender, comorbidities, presenting complaints, physical examination findings, investigation findings, operative procedure, operating surgeon and their details, complications, mortality, length of hospital stay, and clinical improvement at the time of follow-up. If any comorbidity was listed within the medical chart, it was recorded. Potential risk factors, including history of trauma or fall, alcohol use, history of epilepsy, chronic renal failure, liver cirrhosis, or hematologic diseases, and usage of anticoagulation or antiplatelet medications, were also searched for and recorded. Procedure duration was not available during the data collection period. Details about the supervising surgeons, including specialty, level of training, and duration of commitment, were recorded. Operations are performed with the assistance of surgical residents under the supervision of typically senior residents and always with supervision of a consultant surgeon of all residents. The measured level of resident supervision required by the supervisor was not implemented prior to the completion of the data collection. A supervisor whose commitment to the institution was for less than 6 months was considered short-term. Our nonprofit mission hospital often relies on short-term volunteers to help with the staffing of the hospital.
The primary outcomes were recurrence and mortality. A secondary outcome was symptom improvement. A patient was determined to have improved if their symptoms or neurological deficit had resolved or improved at the time of the last follow-up. If improvement of symptoms or neurological deficit was achieved, this was defined to be a favorable outcome. Recurrence was defined as a return or persistence of symptoms which prompted confirmation by CT scan imaging. Mortality was defined as any death within 30 days of the operation regardless of whether it was related to the procedure. Fourteen-day follow-up visits were typical since our standard procedure is to have a postoperative clinic visit at 2 weeks. In our setting, if a patient is doing well, he or she will not return due to the financial hardship of travel. When patients are found to be doing well, they are discharged from surgical clinic with instructions on signs and symptoms to return. Patients who experience complications or recurrence will almost universally return to our facility since there are limited options for treatment at nearby facilities. Routine postoperative imaging on asymptomatic patients is not performed. If problems do develop such as recurrence or mortality, it is very likely that the patient would return to our facility.
The data were collected using a standardized data collection sheet and the results entered into a Microsoft Excel spreadsheet and summarized using descriptive statistics. Epi Info Version 3.5.4 was utilized for data analysis. Sample size did not permit multivariate analysis for outcomes based on the clinical provider. Statistical tests include Chi-square analysis and Fisher’s exact test for low frequencies in addition to Mann–Whitney U test for outcomes between different nonparametric groups. A p value of 0.05 was considered for a statistically significant difference.
Results
There were 119 patients identified with male preponderance of 80%. The mean age was 61.3 years (range 19–94 years). The main presenting complaints are listed in Table 1.
The most common risk factors for cSDH were a history of trauma (54.6%), alcohol use (33.6%), and epilepsy (3.4%). The most frequent comorbidities included hypertension (25.4%) and diabetes mellitus (4.2%). There were no patients in this series with known coagulopathy or on anticoagulant medications.
The majority of patients had a Glasgow Coma Scale (GCS) of 15 (47%) and 14 (22%). The presenting GCS was a mean of 13.2, median of 14, and range of 3–15. On evaluation with a CT scan, the hematoma was found on the left side (45%), right side (35%), and bilateral (19%). Operations were typically performed under general anesthesia (95%) with two burr-holes and irrigation (100%). A subdural drain was left in situ in the majority of patients (98%). The drain, typically a Foley catheter, was left in place for median of 2 days and mean of 2.1 days (range 0–7 days) with a duration of hospital stay of a median 3 days, mean 3.8 days (range 2–14 days).
Outpatient follow-up was available for 109 patients (92%). Postoperative complications included recurrence 6 (5.2%), seizures 4 (3.4%), and subdural empyema 3 (2.5%). No cortical lacerations were identified in this series. In our setting, there was no statistical difference in the duration of subdural drain placement in patients with recurrence (mean 2.8 days, range 2–6 days) and those without recurrence (mean 2.2 days, range 1–7 days) (p = 0.20). Mortality occurred in 8 patients within 30 days (6.7%). Death occurred an average of 8.25 days after the operation (median 6 days; range 2–21 days). Causes of death were respiratory failure with pneumonia (4), atrial fibrillation with stroke (1), seizures (1), renal failure (1), and sepsis from decubitus ulcer (1). Mortality was associated with an increased average age, 73.4 versus 60.5 years (p = 0.04), a lower average presenting GCS, 10 versus 14 (p = 0.01), presence of diabetes (p = 0.002), and a higher ASA score, 2.8 versus 2.2 (p = 0.02). There was no correlation with duration of presentation (p = 0.27), alcohol use (p = 0.19), or sex (p = 0.72). The majority of the patients (90.8%) had a favorable outcome.
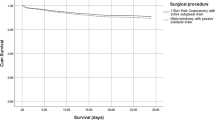
Cases were performed by surgical residents with the involvement of senior residents and consultants. Faculty are consulted for all patients that undergo an operation. Immediate supervision in the operating room was by senior residents (46), consultant general surgeons (65), and consultant neurosurgeons (8). Care was provided by 21 surgical residents, 11 long-term and 3 short-term general surgeons, and 2 short-term neurosurgeons. The neurosurgery group operated on patients with higher ASA scores (p = 0.02) and longer duration of symptoms (p = 0.03) (Table 2). There was no significant statistical difference in negative outcomes between general surgeons and neurosurgeons or between consultant and resident supervision (Table 3). The sicker patients in the neurosurgery group likely contribute to the finding that improvement of symptoms was more likely in the general surgery group (p = 0.01). Although the sample size is limited, the length of commitment from the supervising surgeon was statistically significant for mortality and improvement, but also for the higher ASA. Supervisors who were committed to less than 6 months, including general surgeons and neurosurgeons, were more likely to operate on patients with higher ASA scores (p = 0.02), and to have mortality (p < 0.001) and less likely to have improvement in symptoms (p = 0.01).
Discussion
Chronic subdural hematoma (cSDH) is one of the most common neurosurgical conditions. With an increasing global incidence, it is treatable by relatively simple surgical interventions in which the majority of patients experience improvement. Our results demonstrate that chronic subdural hematomas can be effectively managed with acceptable outcomes by general surgeons and general surgery residents in a low-resource setting. This review of patients with cSDH is to our knowledge among the first series to describe the operative management of cSDH by general surgeons in sub-Saharan Africa and other low-resource settings.
However, for years, general surgeons working in low-resource settings have managed neurosurgical conditions out of necessity [22]. The thought that emergency care is better than no care at all has driven surgeons and other providers to work outside of their comfort zones to provide life-altering therapy to patients in need. At Tenwek Hospital, missionary and national surgeons have provided this care for years. Visiting neurosurgeons have helped to refine techniques, improve the quality of care, and expand elective services [23, 24]. Since the implementation of a surgical training program in 2008 [25], general surgery residents have been capably performing essential surgery under the supervision of general surgeons and surgical specialists. The essential surgical skill of burr-hole craniostomy [26] has been effectively applied to the treatment of cSDH in our setting. The pressing need for more general surgeons capable of managing neurosurgical conditions should also be prioritized.
The need to further neurosurgical training and capacity are increasingly well-recognized priorities within sub-Saharan Africa [27, 28]. There are some reports of neurosurgery residents [14] and general surgeons [13, 29,30,31,32,33] performing burr-hole craniostomy outside of sub-Saharan Africa. Other examples exist within low- and middle-income countries (LMICs) with attempts to transfer specific neurosurgical skills to local health care workers [34, 35]. In Tanzania, visiting neurosurgeons instructed and then supervised procedures. Basic cranial and spinal neurosurgical procedures were taught [34]. Over time, through this organization, Madaktari Africa, complication rates decreased and trainees became trainers [35]. Although our sample size is small, our data suggest that long-term commitment of the supervising physician may be associated with improved patient selection and decreased mortality. If this holds to be true in further data collection, it would emphasize the need for a long-term presence, as suggested by others, when providing surgical care in LMICs [36]. Neurosurgery consultants were more likely to operate on patients who had a longer duration of symptoms and higher ASA scores (Table 2). This could reflect a patient selection bias that more difficult patients are selected for visiting neurosurgeons or that visiting supervisors are more aggressive with the limited resources available than those with long-term commitment. Since the conclusion of this study, our institution now has a long-term neurosurgeon and will have ongoing data collection.
Despite increasing interest in global surgery, cost-effectiveness analyses often neglect neurosurgical interventions in their calculations [37]. Simple burr-hole craniostomy has the ability to drastically improve the quality of life and functional status with a relatively low-cost intervention. Furthermore, patients who benefit from intervention are often the breadwinners for their family and their disability or death can result in catastrophic consequences for family members. This aspect warrants further study.
To ensure our institution is providing quality surgical care, we intended to determine outcomes to compare to other institutions. The mortality rate in our review was 6.7% which is comparable to other studies that report a range of between 1.2 and 16.7% among patients with cSDH [38,39,40]. Similar to other studies, factors associated with the increased mortality in our series include older age, lower average presenting GCS, and higher mean American Society of Anesthesiologist (ASA) physical status classification. Our recurrence rate of 5.2% is consistent with previous studies which range between 5.5 and 25% [41,42,43,44]. In our setting, there was no difference in the duration of subdural drain placement in patients with recurrence.
One limitation to our study is the lack of some important data points at our hospital including the procedure duration, level of resident supervision, and patient follow-up, a problem common to institutions in sub-Saharan Africa [45]. An additional limitation is our intentional follow-up period of 2 weeks. Patient follow-up can be difficult in our setting and other low-resource settings [46, 47]. Due to cost constraints and the burden of follow-up to patients who have recovered and are otherwise well, we do not prioritize routine follow-up care after 2 weeks. Despite this, we were able to obtain outpatient follow-up on over 90% of patients. While it is possible that patients with recurrence or complications present to a different institution, there are very few hospitals within Kenya capable and willing to manage such patients. Accordingly, patients with complications from surgical procedures will typically return to our institution for further care. A further limitation to the analysis on comparing outcomes based on provider is a lack of sample size inhibiting our ability to perform multivariate analysis. We urge caution in interpreting the results; however, the findings are of interest and will be further evaluated in future studies.
Overall, our results show that favorable outcomes can be achieved by general surgeons performing burr-hole craniostomy. We contend that burr-hole trephination can be safely taught to general surgeons and should be an essential part of surgical training in low-resource settings. This series demonstrates the importance of training general surgeons to have burr-hole craniostomy within their repertoire. Thus, patients suffering from cSDH should be able to access appropriate care even in rural areas of sub-Saharan Africa.
References
Panourias IG, Skiadas PK, Sakas DE et al (2005) Hippocrates: a pioneer in the treatment of head injuries. Neurosurgery 57:181–189
Margetts EL (1967) Trepanation of the skull by the medicine-men of primitive cultures, with particular reference to present-day native East African practice. In: Brothwell D, Sandison AT (eds) Diseases in antiquity: a survey of diseases, injuries and surgery of early populations. Charles C Thomas, Springfield, pp 637–701
Qureshi MM, Olunya DO (2010) History of neurosurgery in Kenya, East Africa. World Neurosurg 73(4):261–263
Otieno T, Woodfield JC, Bird P et al (2004) Trauma in rural Kenya. Injury 35(12):1228–1233
Albright AL, Ferson SS (2012) Developing pediatric neurosurgery in a developing country. J Child Neurol 27(12):1559–1564
Kolias AG, Chari A, Santarius T et al (2014) Chronic subdural haematoma: modern management and emerging therapies. Nat Rev Neurol 10(10):570–578
Parlato C, Garracino A, Moraci A (2000) Spontaneous resolution of chronic subdural hematoma. Surg Neurol 53(4):312–317
Ethem G, Mahmut A, Tanju U et al (2009) Spontaneous resolution of large chronic subdural hematoma: a case report and review of literature. Turk J Emerg Surg 15(1):95–98
Gökmen M, Sucu HK, Ergin A et al (2008) Randomized comparative study of burr-hole craniostomy versus twist drill craniostomy; surgical management of unilateral hemispheric chronic subdural hematomas. Cent Eur Neurosurg Zentralblatt für Neurochir 69(03):129–133
Liu W, Bakker NA, Groen RJ (2014) Chronic subdural hematoma: a systematic review and meta-analysis of surgical procedures: a systematic review. J Neurosurg 121(3):665–673
Ishibashi A, Yokokura Y, Adachi H (2011) A comparative study of treatments for chronic subdural hematoma: burr hole drainage versus burr hole drainage with irrigation. Kurume Med J 58(1):35–39
Mondorf Y, Abu-Owaimer M, Gaab MR et al (2009) Chronic subdural hematoma—craniotomy versus burr hole trepanation. Br J Neurosurg 23(6):612–616
Treacy PJ, Reilly P, Brophy B (2005) Emergency neurosurgery by general surgeons at a remote major hospital. ANZ J Surg 75(10):852–857
Phang I, Sivakumaran R, Papadopoulus MC (2015) No association between seniority of surgeon and postoperative recurrence of chronic subdural hematoma. Ann R Coll Surg Engl 97(8):584–588
Liang KE, Bernstein I, Yoko KA et al (2016) Enhancing neurosurgical education in low- and middle-income countries: current methods and new advances. Neurol Med Chir 56(11):709–715
Ellegala DB, Simpson L, Mayegga E et al (2014) Neurosurgical capacity building in the developing world through focused training: clinical article. J Neurosurg 121(6):1526–1532
Wilson DA, Garrett MP, Wait SD et al (2012) Expanding neurosurgical care in northwest Tanzania: the early experience of an initiative to teach neurosurgery at bugando medical centre. World Neurosurg 77(1):32–38
Fuller A, Tran T, Muhumuza M et al (2016) Building neurosurgical capacity in low and middle income countries. eNeurologicalSci 3:1–6
Park BE (2010) The African experience: a proposal to address the lack of access to neurosurgery in rural sub-Saharan Africa. World Neurosurg 73(4):276–279
Santarius T, Kirkpatrick PJ, Ganesan D et al (2009) Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet 374(9695):1067–1073
Peng D, Zhu Y (2016) External drains versus no drains after burr-hole evacuation for the treatment of chronic subdural haematoma in adults. Cochrane Database Syst Rev. Issue 8. Art. No.: CD011402. doi:10.1002/14651858.CD011402.pub2
Kaptigau WM, Rosenfeld JV, Kevau I et al (2016) The establishment and development of neurosurgery services in Papua New Guinea. World J Surg 40(2):251–257. doi:10.1007/s00268-015-3268-1
Park BE (2016) Surgical treatment of degenerative lumbar spine disease in rural sub-Saharan Africa: a retrospective study of 450 cases and its future implications. World Neurosurg 87:417–421
Cheatham ML (2013) Bringing neurosurgical and neurological care to the world. Surg Neurol Int. doi:10.4103/2152-7806.120221
Pollock JD, Love TP, Steffes BC (2011) Is it possible to train surgeons for rural Africa? A report of a successful international program. World J Surg 35(3):493–499. doi:10.1007/s00268-010-0936-z
Mock CN, Donkor P, Gawande A et al (2015) Essential surgery: key messages from disease control priorities. Lancet 385(9983):2209–2219
El Khamlichi A (2001) African neurosurgery: current situation, priorities, and needs. Neurosurgery 48:1344–1347
El-Fiki M (2010) African neurosurgery, the 21st-century challenge. World Neurosurg 73(4):254–258
Schecter WP, Peper E, Tuatoo V (1985) Can general surgery improve the outcome of the head-injury victim in rural America? A review of the experience in American Samoa. Arch Surg 120:1163–1166
Rinker CF, McMurry FG, Groeneweg VR et al (1998) Emergency craniotomy in a rural Level III trauma center. J Trauma 44(6):984–989
Wester K (1999) Decompressive surgery for “pure” epidural hematomas: does neurosurgical expertise improve the outcome? Neurosurgery 44(3):495–500
Bishop CV, Drummond KJ (2006) Rural neurotrauma in Australia: implications for surgical training. ANZ J Surg 76(1–2):53–59
Luck T, Treacy PJ, Mathieson M et al (2015) Emergency neurosurgery in Darwin: still the generalist surgeons’ responsibility. ANZ J Surg 85(9):610–614
Coburger J, Leng LZ, Rubin DG et al (2014) Multi-institutional neurosurgical training initiative at a tertiary referral center in Mwanza, Tanzania: where we are after 2 years. World Neurosurg 82(1):e1–e8
Ellegala DB, Simpson L, Mayegga E et al (2014) Neurosurgical capacity building in the developing world through focused training: clinical article. J Neurosurg 121(6):1526–1532
Ibrahim GM, Bernstein M (2015) Models of neurosurgery international aid and their potential ethical pitfalls. Virtual Mentor 17(1):49
Prinja S, Nandi A, Horton S et al (2015) Costs, effectiveness, and cost-effectiveness of selected surgical procedures and platforms. In: Debas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN (eds) Essential surgery: disease control priorities, 3rd edn (vol 1). The International Bank for Reconstruction and Development/The World Bank, Washington; 2015 Apr 2. Chapter 18. PubMed PMID: 26741010
Sambasivan M (1997) An overview of chronic subdural hematoma: experience with 2300 cases. Surg Neurol 47(5):418–422
Mori K, Maeda M (2001) Surgical treatment of chronic subdural hematoma in 500 consecutive cases: clinical characteristics, surgical outcome, complications, and recurrence rate. Neurol Med Chir (Tokyo) 41(8):371–381
Miranda LB, Braxton E, Hobbs J et al (2011) Chronic subdural hematoma in the elderly: not a benign disease. J Neurosurg 114:72–76
Weigel R, Schmiedek P, Krauss JK (2003) Outcome of contemporary surgery for chronic subdural haematoma: evidence based review. J Neurol Neurosurg Psychiatry 74(7):937–943
Horn EM, Feiz-Erfan I, Bristol RE et al (2006) Bedside twist drill craniostomy for chronic subdural hematoma: a comparative study. Surg Neurol 65:150–153
Neils DM, Singanallur PS, Wang H et al (2011) Recurrence-free chronic subdural hematomas: a retrospective analysis of the instillation of tissue plasminogen activator in addition to twist drill or burr hole drainage in the treatment of chronic subdural hematomas. World Neurosurg 78:145–149
Nayil K, Ramzan A, Sajad A et al (2012) Subdural hematomas: an analysis of 1181 Kashmiri patients. World Neurosurg 77:103–110
Tumusiime G, Was A, Preston MA et al (2016) The quality and utility of surgical and anesthetic data at a Ugandan Regional Referral Hospital. World J Surg 41:1–10. doi:10.1007/s00268-016-3714-8
White RE, Parker RK, Fitzwater JW et al (2009) Stents as sole therapy for oesophageal cancer: a prospective analysis of outcomes after placement. Lancet Oncol 10(3):240–246
Ologunde R, Rufai SR (2013) Surgical follow-up in low-income and middle-income countries. Lancet Glob Health 1(3):e132
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kanyi, J.K., Ogada, T.V., Oloo, M.J. et al. Burr-Hole Craniostomy for Chronic Subdural Hematomas by General Surgeons in Rural Kenya. World J Surg 42, 40–45 (2018). https://doi.org/10.1007/s00268-017-4143-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-017-4143-z