
Abstract
Objective
The aim of this study was to compare the radiographic and functional outcomes of operative intervention in patients with both-bone forearm fractures treated by open reduction and internal fixation (ORIF) with plates or intramedullary (IM) nailing.
Methods
Studies published in PubMed, EMBASE, Web of Science, SinoMed (Chinese BioMedical Literature Service System, China), and CNKI (China National Knowledge Infrastructure, China) were systematically searched. The main outcomes included time to union, union rate, operation time, magnitude and location of radial bow, loss of forearm rotation, and complication rates. Results were expressed with weighted mean difference or risk ratio with 95 % confidence intervals. Pooled estimates were calculated using a fixed-effects or random-effects model according to the heterogeneity among studies.
Results
A total of 13 studies met the inclusion criteria and were included in this meta-analysis. Compared with ORIF, IM nailing significantly reduced the operation time and complication rate. However, no significant differences were observed between the two surgical techniques in several outcomes, including time to union, union rate, radial bow magnitude, and loss of forearm rotation. Except in complications, these findings were consistent across the subgroup analysis of children and adult patients.
Conclusion
IM nailing is associated with shorter operation time and lower complication rate compared with ORIF. It is an effective and safe treatment option for children and adults with both forearm fractures. However, considering the limitations in this study, large-scale, high-quality randomized controlled trials are needed to indentify these findings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Both-bone forearm fractures account for 3.4 % of all pediatric fractures and 26 % of pediatric upper extremity long-bone fractures [1, 2]. As one of the various types of forearm fractures, both-bone forearm fractures are frequently occurred in adults in clinical practice [3]. It has been demonstrated that open reduction and internal fixation (ORIF) with plates is the most commonly used technique for the treatment of operative stabilization of diaphyseal fractures of both forearm bones [4]. Several advantages of plate fixation have been proposed, including good fixation, adequate reduction, and satisfactory healing and functional recovery [5]. However, it also has several recognized complications, such as extensive soft tissue damage, radioulnarsynostosis, and neurovascular injury, nonunion, refracture and infection after plate removal [6–9]. Intramedullary (IM) nailing has been proposed as an alternative method to circumvent these above problems [10, 11]. Many reports showed several advantages of the IM nailing technique, including improved cosmesis, limited soft tissue dissection, reduced operative time, ease of implant removal, and early return to activity after implant removal [6, 12]. However, IM nailing may not be favored for both-bone forearm fractures because it might result in high rate of nonunion, neurovascular injuries, and the need for additional immobilization [13].
It was hypothesized that ORIF and IM nailing would achieve good fixation and functional outcome, minimal damage to soft tissues, and lower refracture. There have been several direct comparisons between ORIF and IM nailing in children or adults [7, 12, 14]. However, their results remained controversial. We therefore conducted this meta-analysis based on available studies to compare the efficacy and safety between ORIF and IM nailing in patients with both-bone forearm fractures.
Materials and methods
Search strategy
We conducted this meta-analysis in adherence to the methods of the Cochrane Handbook for Systematic Reviews of Interventions [15]. The findings were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [16]. PubMed, EMBASE, Web of Science, SinoMed (Chinese BioMedical Literature Service System, China), and CNKI (China National Knowledge Infrastructure, China) were systematically searched from inception through March 20, 2016, to identify relevant studies. The search items were listed as followings: (Both-bone[All Fields] AND (“forearm”[MeSH Terms] OR “forearm”[All Fields]) AND (“fractures, bone”[MeSH Terms] OR (“fractures”[All Fields] AND “bone”[All Fields]) OR “bone fractures”[All Fields] OR “fracture”[All Fields])) AND (open[All Fields] AND reduction[All Fields] AND (“fracture fixation, internal”[MeSH Terms] OR (“fracture”[All Fields] AND “fixation”[All Fields] AND “internal”[All Fields]) OR “internal fracture fixation”[All Fields] OR (“internal”[All Fields] AND “fixation”[All Fields]) OR “internal fixation”[All Fields]) AND plates[All Fields]) AND (“fracture fixation, intramedullary”[MeSH Terms] OR (“fracture”[All Fields] AND “fixation”[All Fields] AND “intramedullary”[All Fields]) OR “intramedullary fracture fixation”[All Fields] OR (“intramedullary”[All Fields] AND “nailing”[All Fields]) OR “intramedullary nailing”[All Fields]). Details of the search strategy are shown in “Appendix”. No language restriction was applied. We also manually searched the bibliographies of the previous reviews and of the included studies to identify other potentially eligible trials.
Study selection
Two investigators independently carried out the literature search, deleted duplicate records, reviewed the titles and abstracts, and identified the records as included, excluded or requiring further assessment. We included the studies that met the following inclusion criteria: (1) population: children or adult patients with simple or moderately comminuted diaphyseal fractures in both forearm bones; (2) intervention: IM nailing; (3) comparison: ORIF; (4) outcome: time to union, magnitude and location of radial bow, operation time, loss of forearm rotation, union rate, and complication rates; and (5) design: randomized controlled trials (RCTs) and observation studies (prospective or retrospective cohort studies). Disagreements between the investigators were resolved by discussion and consensus.
Data extraction and quality assessment
Data extraction was performed by independently. The following information was obtained from each study: first author, year of publication, country, study design, number of patients in each group, demographic characteristic, surgical procedure, and outcome data (time to union, magnitude and location of radial bow, operation time, loss of forearm rotation, union rate, and complication rates). When the same trial appeared in several publications, we retained only the latest, or most information study to avoid duplication of information. The Cochrane risk of bias tool was used to evaluate the risk of bias for each RCT [17], and the modified Newcastle–Ottawa scale was adopted to assess the risk of bias in observational studies [18].
Statistical analysis
We compared the effects of ORIF and IMN in patients with both-bone forearm fractures on the data from the included studies. For continuous variables (i.e., time to union, magnitude and location of radial bow, and operation time), the mean value and standard deviation (SD) were extracted from the included studies. Thereafter, the weighted mean difference (WMD) with 95 % confidence intervals (CIs) was calculated. For dichotomous variables (i.e., loss of forearm rotation, union rate, and complication rates), the number of events and total number of patients was extracted from the included studies. Thereafter, they were expressed as risk ratio (RR) with 95 % CIs. We used I 2 statistic to test the heterogeneity among the included studies, in which I 2 value of greater than 50 % was considered to be substantial heterogeneity [15]. We pooled the WMD and RR of each study by using a fixed-effects model (Mantel–Haenszel method) [19] or random-effects model (DerSimonian–Laird method) [20] according to the heterogeneity. When significant heterogeneity was identified, the random-effects model was used; otherwise, the fixed-effects model was used. Sensitivity analysis was conducted by omitting one study in each turn to explore the influence of a single study on the overall pooled estimate. We also conducted subgroup analysis according to the patients’ age (children vs. adult). The Begg’s [21] and Egger’s [22] tests were conducted to evaluate the presence of publication bias. We considered a P value of less than 0.05 to be statistically significant, except where otherwise specified. All statistical analyses were performed using STATA version 12.0 (StataCorporation, College Station, TX, USA).
Results
Study identification and selection
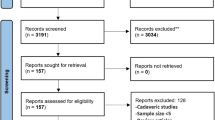
The initial search yielded 1217 relevant citations from PubMed, EMBASE, Web of Science, SinoMed, and CNKI. Of these, 536 were excluded as duplicate records, and 662 were excluded after review of title/abstract (Fig. 1). Therefore, 19 potential studies were identified for the final analysis; however, 6 studies were excluded because four were single-arm studies and two did not provide available data. Finally, 13 studies (involving 854 patients) [6, 23] were included in this meta-analysis.

Eligibility of studies for inclusion in meta-analysis
Study characteristics and quality assessment
The main characteristics of the included studies are shown in Table 1. These studies were published between 2005 and 2016. The sample size ranged from 30 to 200 (ORIF group, 416; IM nailing group 438). Among these studies, eight were published in international English journal [6, 23–29], and five were in Chinese core journal [30–34]. All these studies were prospective or retrospective cohort studies except four [26, 29, 31, 32], which was performed with a RCT design. Of these 13 studies, 2 were conducted in USA [6, 24, 25], 6 in China [29–34], 2 in Germany 6, 26, and 1 each in UK [27], Korea [23], and Turkey [28]. The subject populations in seven studies were adults [23, 26, 29, 31–34] and in six were children [6, 24, 25, 27, 28, 30].
Quality assessment
The risk of bias assessment of the included studies is presented in Table 2. One of the four RCTs was considered as low risk, while the remaining three were uncertain. Based on the Newcastle–Ottawa scale to evaluate the risk of bias of cohort studies, all these studies were scaled as a total score of >5 (Table 3), indicating a low risk of bias.
Time to union
Six of the included studies provided data for time to union [23, 24, 28, 29, 31, 32]. Compared with IM nailing, ORIF had no benefit on time to union (WMD = 0.98 weeks, 95 % CI −0.92, 2.87; P = 0.312) (Fig. 2), with significant heterogeneity (P < 0.001, I 2 = 88.0 %). The results also were consistent across all subgroup analyses (for adult: WMD = 1.23 weeks, 95 % CI −1.29, 3.76; P = 0.339; for children: WMD = 0.35 weeks, 95 % CI −1.48, 2.19; P = 0.705) (Fig. 2).

ORIF versus IM nailing on time to union
When we excluded the trial conducted by Lee et al. [23], the overall estimate changed substantially, which showed that ORIF had 2.01 weeks more of time to union than IM nailing (WMD = 2.01 weeks, 95 % CI 0.89, 3.14; P < 0.001); however, the heterogeneity was still present (P = 0.053, I 2 = 57.2 %). Further exclusion of any single study did not alter the overall estimate, and the evidence of heterogeneity was still observed among the remaining studies (data not shown).
Union rate
Five studies reported the data for union rate [23, 25, 30, 31, 34]. Compared with IM nailing, ORIF did not significantly increase union rate (RR = 0.95, 95 % CI 0.85, 1.05; P = 0.312) (Fig. 3). There was no evidence of heterogeneity (P = 0.224, I 2 = 29.6 %). These results of similar union rate were consistent in all subgroup analyses (for adult: RR = 0.92, 95 % CI 0.77, 1.09; P = 0.329; for children: RR = 0.98, 95 % CI 0.89, 1.09; P = 0.763) (Fig. 3).

ORIF versus IM nailing on union rate
Operation time
Eight studies reported the data for operation time [6, 23, 25, 26, 28, 29, 32, 34]. Compared with IM nailing, ORIF significantly increased the operation time (WMD = 20.43 min, 95 % CI 11.79, 29.07; P < 0.001) (Fig. 4). There was statistical heterogeneity between the individual studies (P < 0.001, I 2 = 99.8 %). The findings of longer operation time were consistent in all subgroup analyses (for adult: WMD = 13.92 min, 95 % CI 3.24, 24.6; P = 0.011; for children: WMD = 27.12 min, 95 % CI 20.98, 33.25; P < 0.001) (Fig. 4).However, the heterogeneity was still present in each subgroup analyses.

ORIF versus IM nailing on operation time
In the subgroup analysis for adult, when we excluded any single study, the pooled estimates did not change substantially, yet the heterogeneity was still present. When two trials of Lee et al. [23] and Zhang et al. [29] were excluded, the overall results altered slightly (WMD = 16.41 min, 95 % CI 15.45, 17.38; P < 0.001), but no evidence of heterogeneity was observed (P = 0.137, I 2 = 54.8 %).
In the subgroup analysis for children, exclusion of one trial conducted by Qu et al. [34] changed the overall estimate little (WMD = 30.09 min, 95 % CI 28.31, 31.87; P < 0.001), and no evidence of heterogeneity was found among the remaining studies (P = 0.618, I 2 = 0.0 %).
Magnitude and location of radial bow
Four studies reported the data for radial bow magnitude and location [23–25, 27]. Compared with IM nailing, ORIF had similar radial bow magnitude (WMD = −0.05 mm, 95 % CI −0.75, 0.65; P = 0.889), but different locations of radial bow (WMD = −5.78 %, 95 % CI −7.76 %, −3.80 %; P < 0.001) (Fig. 5). The test for heterogeneity was not significant (for radial bow magnitude: P = 0.376, I 2 = 3.4 %; for radial bow location: P = 0.255, I 2 = 26.1 %). Since only one study reported data for radial bow magnitude and location in adults, subgroup analysis was not performed.

ORIF versus IM nailing on radial bow magnitude and location
Loss of forearm rotation
Three studies reported the data for loss of forearm rotation [24, 25, 27]. Compared with IM nailing, ORIF had a similar loss of forearm rotation rate (RR = 1.27, 95 % CI 0.62, 2.61; P = 0.508). There was no significant heterogeneity between the included studies (P = 0.387, I 2 = 0.0 %).
Complication rate
Twelve studies reported the data for complications [6, 23–30, 32–34]. These postoperative complications included refractures, ulna nonunion, delayed union, superficial wound infections, superficial radial nerve palsy, and hypertrophic scars. The complication rates were 21.6 and 13.7 % in the ORIF and IM nailing groups, respectively. Compared with IM nailing, ORIF resulted in a significant higher complication rate (RR = 1.63, 95 % CI 1.19, 2.22; P = 0.002) (Fig. 6), with no significant heterogeneity (P = 0.545, I 2 = 0.0 %). These findings were also found in the adult patients (RR = 2.26, 95 % CI 1.42, 3.60; P = 0.001), but not in children patients (RR = 1.14, 95 % CI 0.74, 1.73; P = 0.557).

ORIF versus IM nailing on complication rate
Publication bias
The assessment of publication bias showed that there was no evidence of significant publication bias by the formal statistical tests (Egger’s test, P = 0.822; Begg’s test, P = 0.304) (Fig. 7).

Funnel plot for assessment of publication bias
Discussion
The present meta-analysis identified 13 studies comparing the radiographic and functional results of operative intervention in patients with both-bone forearm fractures treated by ORIF or IM nailing. The analysis showed that IM nailing significantly decreased operation time and complication rate compared with ORIF. However, IM nailing had similar effects with ORIF in time to union, union rate, and loss of forearm rotation. Moreover, all these findings except complications were consistent across the subgroup analyses based on children and adult.
ORIF is the treatment of choice for the majority of both-bone forearm fractures in adults. However, for pediatric patients, approximately 90 % of both-bone forearm fractures are effectively managed with closed reduction and casting [7]. Operative treatment has been used for the fixation of pediatric both-bone forearm fractures when the following indications are presented: open fracture, failure to obtain or maintain adequate closed reduction, and displaced fractures in children approaching skeletal maturity [24]. Among the operative treatments, ORIF and IM nailing are the principal surgical alternatives for children.
There has been one published systematic review of plate fixation and IM nailing for children [4]. In that study, the authors selected 8 retrospective comparative studies to compare functional outcomes and complications of plate fixation versus IM nailing for both-bone diaphyseal forearm fractures requiring fixation in children aged 0–18 years [4]. They found that there was no significant difference in time to fracture union between the two groups, but operation duration was significantly shorter in the IM nailing group [4]. Their results are consistent with the findings of ours, in which the IM nailing achieved shorter operation duration but similar time to union than ORIF in children. In terms of location of the radical bow, the authors found that it was significantly different in two studies, but no difference in forearm rotation, which was also identified in our study. For the complication rate, they demonstrated that there was no statistical difference between the two groups [4]. This result was accordance with the finding in our study, in which IM nailing had similar complication rate with ORIF for children, but lower complication rate for adults. In addition to these above outcomes, we also explored effect of union rate, as well as compared the radiographic and functional outcomes in the subpopulation of adult patients, which was not investigated in that systematic review. Furthermore, this study is a meta-analysis using the methodology of a random-effects or fixed-effects model to pool the estimates, whereas the previous study is a systematic review, which only presented the eligible studies, and did not synthesize the estimates for the outcomes of interest.
Several advantages of IM nailing have been reported in the previous studies, including shorter operation time, smaller incisions, limited soft tissue dissection, and ease of implant removal [6, 12, 35]. In this study, we found that operation time in the IM nailing group was significantly shorter than that in the ORIF group. Our results are supported by other comparison studies, which also demonstrated a shorter operation time of IM nailing [6, 23, 25, 26, 28]. Reinhardt et al. [25] compared the radiographic and functional outcomes of IM nailing to ORIF of forearm fractures in children between 10 and 16 years of age. Their results showed that the surgical time was significantly shorter for the IM nailing group (103.4 min) than that for the ORIF group (132.6 min) (P = 0.037) [25]. However, compared with ORIF, IM nailing method requires a second operation for the removal of IM fixation, which would result in a second anesthetic. This is one disadvantage of IM nailing [24].
Although IM nailing has the merit of limited soft tissue dissection, some authors suggest that ORIF could more correctly restore the anatomical bow of the radius [12, 36]. In the included studies, the location of radius bow was measured as a percentage of radial length as described by Schemitsch and Richards [36] in adults and adapted by Firl and Wunsch [37] to children. Our results showed that the location of radial bow was significantly improved in ORIF group relative to IM nailing group (WMD = −5.78 %, 95 % CI −7.76 %, −3.80 %; P < 0.001). Results from the studies of Schemitsch and Richards indicated that restoration of the radial bow is critically important in reconstituting the normal forearm architecture, and restoring forearm rotation and grip strength [36, 38]. Changes in either the magnitude or location of radial bow would result in the loss of forearm rotation [36, 39, 40]. In this study, the ORIF had better anatomical correction of location of the radial bow than IM nailing; however, the percentage of patients with a loss of rotation in the ORIF group was not reduced. One possible reason for this may be due to limited sample size, which decreased the statistical power to detect the difference in loss of rotation between the two groups. Thus, a larger-scale prospective study is needed to identify the correlation between restoration of radial bow location and loss of forearm rotation.
Most importantly, it was found in our study that ORIF was associated with a higher complication rate than IM nailing. This result was observed in most of the included studies. However, in two studies of Fernandez et al. [6] and Qu et al. [34], they found a lower complication rate in the ORIF group, although the trend did not reach statistical significance. In the study of Fernandez et al. [6], three of 19 (15.8 %) children in the ORIF group developed complications, including two refracture and one hypesthesia of thumb [6]. In contrast, in the IM nailing group, nine of 45 (20.0 %) children developed complications. These complications included three hypesthesia of thumb, two skin infections, two delayed fracture healing, one refracture, and one pseudarthrosis [6]. In another study conducted by Zhang et al. [29], it was found that the two surgical methods had similar complication rate. In that study, 3 delayed unions and 3 infections occurred in the ORIF group (28.6 %), and 3 malunion and 3 radial nerve injuries occurred in the IM nailing group (27.3 %) [29]. The authors explained these complications with the followings reasons: first, the plate fixation requires large incision [27], and attaching a rigid plate blocks the blood supply of periosteum [27]; second, the rotational alignment may be difficult with IM nailing, and this method may increase the risk of neurovascular injury [13].
There are several potential limitations in this study. First, this meta-analysis was performed on 13 studies, and most of the included studies had a relatively small sample size. Although these studies were of high quality, or with low risk, caution should be taken when interpreting our findings because studies with small sample size are more likely to result in an overestimation of the treatment effects compared with large-scale trials. Second, among the 13 included studies, only four were RCTs, and the remaining nine were cohort studies. Although the cohort studies can reflect the “real world” and further support the conclusion, cohort data are of course highly subject to confounding. Third, although no significant heterogeneity was found for most of the outcomes, population characteristics, fracture type, and injury mechanism varied across the included studies. To explore whether these factors have a potential impact on the overall pooled results, we conducted subgroup analysis and the results were consistent across the subgroup, which added robustness of our findings. Fourth, we were unable to assess the impact of fracture type on the clinically meaningful outcomes, such as time to union, duration of operation, and complication rate, due to sparse data among the included studies.
In conclusion, the current meta-analysis suggests that IM nailing is associated with shorter operation time and lower complication rate compared with ORIF. IM nailing is an effective and safe treatment option for children and adults with both forearm fractures. However, our results are largely obtained from data of cohort studies, which is inclined to selection bias. Thus, our findings should be interpreted with caution. And large-scale, high-quality RCTs are needed to indentify these findings.
References
Mann DC, Rajmaira S (1990) Distribution of physeal and nonphyseal fractures in 2,650 long-bone fractures in children aged 0–16 years. J Pediatr Orthop 10:713–716
Landin LA (1983) Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand Suppl 202:1–109
Truntzer J, Vopat ML, Kane PM et al (2015) Forearm diaphyseal fractures in the adolescent population: treatment and management. Eur J Orthop Surg Traumatol 25:201–209
Patel A, Li L, Anand A (2014) Systematic review: functional outcomes and complications of intramedullary nailing versus plate fixation for both-bone diaphyseal forearm fractures in children. Injury 45:1135–1143
Droll KP, Perna P, Potter J et al (2007) Outcomes following plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 89:2619–2624
Fernandez FF, Egenolf M, Carsten C et al (2005) Unstable diaphyseal fractures of both bones of the forearm in children: plate fixation versus intramedullary nailing. Injury 36:1210–1216
Smith VA, Goodman HJ, Strongwater A et al (2005) Treatment of pediatric both-bone forearm fractures: a comparison of operative techniques. J Pediatr Orthop 25:309–313
Rodriguez-Merchan EC, Gomez-Castresana F (2004) Internal fixation of nonunions. Clin Orthop Relat Res 419:13–20
Henle P, Ortlieb K, Kuminack K et al (2011) Problems of bridging plate fixation for the treatment of forearm shaft fractures with the locking compression plate. Arch Orthop Trauma Surg 131:85–91
Sage FP (1959) Medullary fixation of fractures of the forearm. A study of the medullary canal of the radius and a report of fifty fractures of the radius treated with a prebent triangular nail. J Bone Joint Surg Am 41-a:1489–1516
Rush LV, Rush HL (1949) The technique of longitudinal pin fixation of fractures of the forearm. Miss Doct 27:284–288
Van der Reis WL, Otsuka NY, Moroz P et al (1998) Intramedullary nailing versus plate fixation for unstable forearm fractures in children. J Pediatr Orthop 18:9–13
Visna P, Vlcek M, Valcha M et al (2009) Management of diaphyseal forearm fractures using LCP angle- stable fixation devices and intramedullary nailing. Rozhl Chir 88:708–715
Carmichael KD, English C (2007) Outcomes assessment of pediatric both-bone forearm fractures treated operatively. Orthopedics 30:379–383
Higgins JP, Thompson SG, Deeks JJ et al (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Higgins JP, Altman DG, Gotzsche PC et al (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Wells G, Shea B, O’connell D, et al (2000) The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. In: 3rd symposium on systematic reviews: beyond the basics, pp 3–5
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22:719–748
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101
Egger M, Davey Smith G, Schneider M et al (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Lee SK, Kim KJ, Lee JW et al (2014) Plate osteosynthesis versus intramedullary nailing for both forearm bones fractures. Eur J Orthop Surg Traumatol 24:769–776
Shah AS, Lesniak BP, Wolter TD et al (2010) Stabilization of adolescent both-bone forearm fractures: a comparison of intramedullary nailing versus open reduction and internal fixation. J Orthop Trauma 24:440–447
Reinhardt KR, Feldman DS, Green DW et al (2008) Comparison of intramedullary nailing to plating for both-bone forearm fractures in older children. J Pediatr Orthop 28:403–409
Gradl G, Mielsch N, Wendt M et al (2014) Intramedullary nail versus volar plate fixation of extra-articular distal radius fractures. Two year results of a prospective randomized trial. Injury 45(Suppl 1):S3–S8
Teoh KH, Chee YH, Shortt N et al (2009) An age- and sex-matched comparative study on both-bone diaphyseal paediatric forearm fracture. J Child Orthop 3:367–373
Kose O, Deniz G, Yanik S et al (2008) Open intramedullary Kirschner wire versus screw and plate fixation for unstable forearm fractures in children. J Orthop Surg (Hong Kong) 16:165–169
Zhang XF, Huang JW, Mao HX et al (2016) Adult diaphyseal both-bone forearm fractures: a clinical and biomechanical comparison of four different fixations. Orthop Traumatol Surg Res 102:319–325
Zhen Y, Wang X, Zhang F (2015) The effect of plate fixation versus intramedullary nailing for both forearm bones fractures in older children. In: The fourth Yangtze River delta area trauma annual conference, pp 210–211
Liu X, Zhen X (2011) The treatment comparison between open reduction and internal fixation and Intramedullary nailing for both forearm bone fracture. Pract J Cardiac Cerebral Pneumal Vasc Dis 19:1762–1763
Dong D (2012) The effect comparison between open reduction and internal fixation and Intramedullary nailing for both forearm bone fracture. China J Clin Ration Drug Use 5:45–46
Xia H, Li J, Lv D (2009) Open reduction and internal fixation versus Intramedullary nailing in the treatment of both forearm bone fracture. Chin J Bone Joint Inj 24:1036–1037
Qu X, Zhao Y, Liu S et al (2011) Comparative study of AO dynamic compression plating and Sanatmetal intramedullary nailing for both-bone forearm fracture. Chin J Bone Joint Surg 4:460–463
Ortega R, Loder RT, Louis DS (1996) Open reduction and internal fixation of forearm fractures in children. J Pediatr Orthop 16:651–654
Schemitsch EH, Richards RR (1992) The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 74:1068–1078
Firl M, Wunsch L (2004) Measurement of bowing of the radius. J Bone Joint Surg Br 86:1047–1049
Blau J, Calo JM, Dozor D et al (2011) Transfusion-related acute gut injury: necrotizing enterocolitis in very low birth weight neonates after packed red blood cell transfusion. J Pediatr 158:403–409
Matthews LS, Kaufer H, Garver DF et al (1982) The effect on supination-pronation of angular malalignment of fractures of both bones of the forearm. J Bone Joint Surg Am 64:14–17
Tarr RR, Garfinkel AI, Sarmiento A (1984) The effects of angular and rotational deformities of both bones of the forearm. An in vitro study. J Bone Joint Surg Am 66:65–70
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Appendix
Rights and permissions
About this article

Cite this article
Zhao, L., Wang, B., Bai, X. et al. Plate Fixation Versus Intramedullary Nailing for Both-Bone Forearm Fractures: A Meta-analysis of Randomized Controlled Trials and Cohort Studies. World J Surg 41, 722–733 (2017). https://doi.org/10.1007/s00268-016-3753-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3753-1