
Abstract
Background
Narrowing of the distance between the eyes and eyebrows is commonly observed after subbrow blepharoplasty. The purpose of this study was to quantify the changes in brow-lid distance after subbrow blepharoplasty in Asian women.
Methods
We observed and standardized the pre- and postoperative photographs of 63 patients who underwent subbrow blepharoplasty from January 2020 to October 2022. We measured the distances from the medial and lateral eyebrow to the lower lid margin on the right side of the face and then analyzed the changes in postoperative brow-lid distance using the standard iris diameter for Asian women of 11.5 mm as a reference.
Results
Photographs of 63 patients were included in the study. All 63 patients were females. The average postoperative distance of the lateral eyebrow to the lower lid margin was 30.08 ± 2.74 mm, a significant decrease in comparison to the preoperative distance (31.84 ± 2.65 mm) (P < 0.001). The mean postoperative distance of the medial eyebrow to the lower lid margin was 25.84 ± 2.87 mm, compared with that of the preoperative distance (27.59 ± 2.94 mm), which was a significant decrease (P<0.001). All 63 patients (100%) had a decrease in the lateral eyebrow distance, while 59 (93.65%) had a decreased medial eyebrow distance.
Conclusions
There was a statistically significant change in brow position, consistent with our observations. Subbrow blepharoplasty can cause a decrease in the distance between the eyebrows and eyes.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the aging process, gravity and increasing laxity of the skin can cause slow descent of the lateral eyebrows [1]. In contrast to traditional blepharoplasty, which only removes supratarsal upper eyelid skin rather than subbrow skin, that does not address the redundant skin of lateral hooding, subbrow blepharoplasty (SBB) effectively addresses lateral brow hooding without causing the unnatural appearance and visible incisions seen with blepharoplasty [2]. A direct brow lift by suprabrow approach is a common method, but scarring after surgery is a limitation [3]. Subbrow blepharoplasty, which removes the thicker skin from zone 3 and could move the thin and thick junction of the upper eyelid skin upward according to the 3 skin zone concept from Choi [4], is a useful procedure to ensure an aesthetic result. A direct brow lift by supra-brow approach is a common method, as it is easy, effective, and minimally invasive, but scarring after surgery is a limitation. The SBB procedure has the advantages of hidden incisions and minimal changes in appearance [5]. It has become a commonly used periorbital rejuvenation procedure in Asian women for the upper eyelids [2].
However, postoperative descent of the eyebrows is noticeable in nearly all patients following SSB, which is a widely cited disadvantage [6]. Eyebrow plays a significant role as facial landmarks and in aesthetic appearance. Additionally, facial attractiveness can benefit from having an appropriate brow-lid distance [7]. Positioning of the eyebrows also impacts emotional expression [8]. Eyebrows located above the supraorbital rim are considered more aesthetically attractive in women.
Scholars have made attempts to improve the surgery, resulting in different approaches such as removing the orbicularis oculi muscle or other suspension methods, such as incorporation of supraorbital rim periosteal fixation [9] and using frontalis sling [10]. However, the effectiveness of these procedures relies heavily on subjective rating scales, with few objective measurements. Additionally, there are no objective data on the relationship between eyebrow position and surgery.
The precise extent of brow position changes associated with subbrow blepharoplasty remains uncertain. Further research is needed to determine this value. If universal data are available, we can better predict postoperative outcomes, contribute positively to preoperative counseling, and enhance patient satisfaction.
The purpose of this study is to quantify the changes in brow-lid distance after subbrow surgery, establish a simple quantitative assessment method, and guide the design of surgical protocols in the clinic.
Patients and Methods
Patients
Sixty-three female patients who underwent subbrow blepharoplasty surgery between January 2020 and October 2022 and had sufficient pre- and postoperative photographs were included in this retrospective evaluation. The follow-up period ranged from immediately postoperation to 3 months after surgery. The ages of the patients ranged from 28 to 66 years, with an average age of 47 years. All procedures were performed by two surgeons (TLW and LJX) by the same regulation. All patients provided informed consent, granting permission for the publication of their data.
Inclusion criteria:
-
1)
Asian, over 25 years old
-
2)
Presence of dermatochalasis/lateral hooding
-
3)
At least 1 postoperative photograph with follow-up with in 3 months
-
4)
Signed informed consent for data disclosure
Exclusion criteria
-
1)
Severe facial asymmetries
-
2)
Previous use of fillers or botulinum toxin
-
3)
Accepted other periorbit operation
Surgical Technique
All preoperative design markings are done in the sitting position. An upper incision line was drawn along the inferior margin of the eyebrow. Determine the lowest point of lower incision line by pinching the loose skin, marking two incisions preoperatively. The upper incision is made along the lower edge of the eyebrow. The excised skin was spindle-shaped and measured approximately 8 mm to 12 mm at its greatest width.
The procedure was performed under local anesthesia using 1% lidocaine with epinephrine. The skin and subcutaneous tissue were excised en bloc. The lower incision is determined according to necessary amount of skin excision. The superior and inferior flaps were fixed separately [5, 9]. Subcutaneous sutures were placed with 6-0 monocryl, and the skin repaired with interrupted and continuous sutures. Skin sutures were removed on the fifth postoperative day.
Photograph Measurements and Standardization
Full-face, front-view photographs were taken according to a standard protocol. All patients were seated with relaxed eyebrows and eyes that were naturally open and looking straight ahead, equal exposure of both ears, with the camera positioned at the same level of the patient’s head and at a distance of 2 meters from the patient. If the distance is far enough, the image shape will not be distorted, and mild angular changes have no significant effect on facial distance. In addition, the case photographs with large angle difference were excluded during statistics.
All photographs were analyzed using Photoshop CS4 (Adobe, San Jose, CA). We first briefly processed the patient’s facial photographs so that the pixel sizes were homogeneous in the pre- and postoperative periods, and we excluded cases in which there was a significant angular difference between the pre- and postoperative periods. The pictures were adjusted to be horizontal, i.e., the pupils were located at the same level bilaterally.
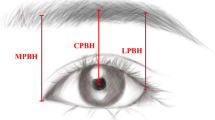
We measured the vertical distance (A) between the horizontal line of the lateral brow (a) to the lower lid margin (c); the vertical distance (B) between the horizontal line of the medial brow (b) to the lid margin (c); and the patients’ iris diameter (d) (Fig. 1). All data were measured three times by two researchers, and then the results were averaged. All patients were observed on the right side of the face; mild asymmetry between left and right face is negligible.

Brow-to-eye spacing measurements. a: The line of the lateral brow; b: the line of the medial brow; c: the line of the lower lid margin; d: the patients’ iris diameter; A the vertical distance between the horizontal line of the lateral brow (a) to the lower lid margin (c); B the vertical distance between the horizontal line of the medial brow (b) to the lower lid margin (c)
In our opinion, the positions of the patients’ lower lid margins will hardly change in the short period of time after the operation. Therefore, the differences in A and B before and after surgery reflected a change in the position of eyebrows. Positive values indicated a decrease in brow position postoperatively, while negative values indicated an increase. Due to variability in facial height and dimensions in the patients, the brow-to-eye spacing was scaled to the iris diameter (11.5 mm in Asian women) for normalization [11].
Statistical Analysis
The IBM SPSS Statistics 29.0.1.0 software (IBM Corporation) was used for all analyses and carried out using complete case. A homogeneity test for variance and paired samples t test were used to analyze the differences between the ratio of pre- and postoperative eyebrow distance. All statistical tests were based on one-tailed probability, and the criterion for significance was set at P < 0.05.
Results
Characteristics of the 63 patients are shown in Table 1. A total of 63 patients were included; all 63 patients were females and had preoperative and postoperative photographs within 3 months. Age range was 28 to 66 years, with a median age of 47 years. All patients underwent SBB and experienced varying degrees of drop of the eyebrow position. A majority had a reduction in brow-to-eye spacing immediately after surgery. The results of the study (Table 2) showed that reduced eyebrow position after subbrow blepharoplasty was prevalent in all patients who underwent surgery.
A reduction in the distance from the peak of the brow to the lower lid margin was observed in 63 patients (100%) postoperatively. The mean postoperative distance of the lateral eyebrow to the lower lid margin was 30.08 ± 2.74 mm, which was significantly decreased compared to the preoperative distance (30.08 ± 2.74 mm) (t = 11.86, P < 0.001; Table 3). The absolute decrease was 1.76 ± 1.17 mm.
In total, 59 patients (93.65%) had a decreased distance from the medial eyebrow to the lower lid margin. The average postoperative distance of the medial eyebrow to the lower lid margin was also decreased compared to the preoperative distance, with a mean value of 25.84 ± 2.87 mm. Compared to preoperatively (27.59 ± 2.94 mm), the decrease was significant (1.75 ± 1.30, t = 10.74; P < 0.001) (Table 4).
The line graphs reflect the change in preoperative and postoperative brow peak height for each patient, with the green representing precount brow peak height, the yellow line representing postoperative brow peak height, and the horizontal axis sorting the patients by age from youngest to oldest (Fig. 2A). Figure 2B reflects the change in brow height of each patient pre- and postoperation, with the blue line representing the precount brow height and the yellow line representing the postoperative brow height. It can be visually seen the change in the position of the eyebrows.

The line graphs reflect the change in preoperative and postoperative brow peak height for each patient, with the green representing precount brow peak height, the yellow line representing postoperative brow peak height, and the horizontal axis sorting the patients by age from youngest to oldest (Fig. 2A). Figure 2B reflects the change in brow height of each patient pre- and postoperation, with the blue line representing the precount brow height and the yellow line representing the postoperative brow height. The horizontal axis sorting the patients by age from youngest to oldest
Subgroup analyses were performed based on the follow-up time of the included patients’ postoperative photographs, with the highest number of patients whose follow-up time was the immediate postoperative period, the lateral brow had a drop of 1.94 ± 1.40 mm, and the medial brow had a drop of 1.84 ± 0.97 mm (Table 5).
Patient 1 is a 43-year-old female who underwent subbrow blepharoplasty. Preoperative and 7-day postoperative photographs are shown. Photographic measurements confirm a slight decrease in brow position after surgery. The height of the peak of the brow decreased by 1.78 mm and the height of the head of the brow decreased by 1.07 mm. A slight brow ptosis was observed after the procedure (Fig. 3). Patient 2 is a 52-year-old female who underwent subbrow blepharoplasty, shown here before and 1 month after surgery. The height of the lateral brow decreased by 4.10 mm and the height of the medial brow decreased by 2.44 mm. Although the subbrow blepharoplasty allowed for the exposure of the original skin fold, the height of the brow peak decreased dramatically and was significantly lower than the height of the head of the brow, which resulted in a change in the angle of the brow and an unsatisfactory cosmetic result (Fig. 4).

Patient 1. A 43-year-old patient who underwent subbrow blepharoplasty shown pre- and 7-day postop. Analysis of the picture confirms a slight drop in the position of the eyebrows. In this patient, the height of the lateral eyebrow has dropped by 1.78mm, and the height of the medial eyebrow has dropped by 1.07 mm

Patient 2. A 52-year-old patient who underwent subbrow blepharoplasty shown pre- and 1-month postop. In this patient, the height of the lateral eyebrow has dropped by 4.10 mm, and the height of the medial eyebrow has dropped by 2.44 mm. Analysis of the picture confirms a slight drop in the position of the eyebrows. SBB can expose the original skin fold, but there is a huge drop in the lateral brow, which is significantly lower than the medial brow, resulting in a change in the angle of the brow and a poor cosmetic result
All 63 patients had a good postoperative recovery with no complications or re-operations. The postoperative scarring was inconspicuous.
Discussion
This study highlights the phenomenon of reduced brow position after subbrow blepharoplasty; an observation identified in all patients who underwent the procedure. Lowering of the lateral eyebrow was observed in nearly 100% of the patients, while 93.65% of the patients also exhibited lowering of the medial eyebrow. No elevation of eyebrows was detected.
The idea of subbrow blepharoplasty was first described in 1976 for dermatochalasis in White patients [12]; has become a common surgical procedure for the rejuvenation of upper eyelids in Asians, particularly when lateral hooding is the primary concern [5]. Periorbital aging in middle-aged and older women is typically characterized by laxity of the upper eyelid skin, accompanied by brow ptosis and periorbital wrinkles [13]. Asians have more pretarsal and suborbicular fat than Caucasians; thus, the distance between the eyebrows and eyes is greater in Asians than in Caucasians, corresponding to a higher position of the eyebrow [14]. SBB procedure is therefore more popular in Asian communities, especially in older patients. In our data, the average age of the patients was 47 years, concentrated between 40 and 60 years of age.
Most middle-aged and elderly patients presenting for rejuvenation of the periorbital area want to look a little more like they did in their youth and usually do not want a significant change in appearance after surgery. Subbrow blepharoplasty is performed through a subbrow incision with appropriate removal of excess skin under the brow, able to show the original double eyelid fold, improve the appearance of "triangle eyes" without new double eyelid incisions. Based on the 3 skin zone concept [4], the removal of the excess skin below the brow prevents the blepharoplasty crease from bloating and sagging compared to removing the thinner skin above the eyelid. For patients with thick eyelid skin, classic upper blepharoplasty may not meet the requirements for cosmetic improvement needed to remove excess skin under the brow. Therefore, excision of the subbrow skin is an excellent option to improve lateral orbital hooding [15].
However, there is a common problem with lowered eyebrow position after subbrow surgery. A common side effect of subbrow blepharoplasty is a drop in eyebrow level postoperative. We have analyzed the possible causes of postoperative eyebrow drop as follows. In the first place, removing a certain width of skin will inevitably result in a change in eyebrow position; the tension created by the incision after the skin is sutured may slightly pull down the eyebrow. Secondly, the redistribution of skin tension during the healing process may lead to certain changes in eyebrow position. The position of the eyebrow is determined by the frontalis muscle that raises the eyebrow and several sets of descending eyebrow muscles together. The frontalis tone may attenuate visual field obscuration due to ptosis by compensatory contraction; surgery has improved the visual field defects and resulted in postoperative relaxation of frontalis tone and a drop in eyebrow level. Finally, Asian eyebrow levels decline with age because of skin laxity, decreased support of the orbital bone due to resorption of aged bone tissue and volumetric atrophy of the periorbital fat room.
The brow is considered the “frame” of the eye and is a critical reference point by which the attractiveness of the eye is judged [16]. With aging, there is little change in the height of the brow at the vertical plane of the midpupil, but that there is descent laterally [17]. Some scholars have found that eyebrows may rise with age; some women chronically elevate their brows to clear their visual field from redundant upper lid skin [18]. An alternative explanation is that aging causes rupture of the levator palpebrae superioris muscle, resulting in ptosis. The elevated brow position observed in some aging patients is due to clinical or subclinical weakness of the levator muscle system [19].
For people with high eyebrow position, a certain degree of eyebrow descent after surgery may instead make the proportion of eyebrows and eyes in the face closer to the golden ratio 0.618, bringing better cosmetic results. For patients with a wide eyebrow-lid spacing, the descent of the eyebrows after surgery not only solves the problem of loose skin on the upper eyelid, but also brings better eyebrow-eye proportions. The angle of the eyebrows also affects the expression of emotions, with the inner side low and the outer side high expressing anger or disgust, and the inner side high and the outer side low expressing tiredness and sadness.
To prevent the inherent problem that eye and brow from moving closer together, the fixation method was used. Various methods for suspension have emerged to improve the surgical approaches, aiming to prevent sagging eyebrows such as browpexy or frontalis sling. Kim YS et al [9], Fang et al [1] used browpexy technique where the lower edge of the orbicularis oculi muscle was fixed to the periosteum, and Kim HS et al [15] attached the orbicularis oculi muscle to the frontalis muscle to avoid postoperative brow position changes. In Kim’s research, which uses a fixation to the periosteum technique, patients showed a narrowing of the brow-lid distance. In fact, almost all the photographs in the related paper have eyebrows closer to the eyes, with or without removal of the orbicularis oculi and with or without suspension. While definitive data are lacking, the images in those papers showed dropped eyebrows in almost all the pre- and postoperative comparison photographs.
Plastic surgeons are aware that eyebrows will drop after surgery, but few take the trouble to estimate the exact amount of drop. Most researchers use subjective rating scales to assess surgical outcomes, such as the Likert scale, which uses the patients’ subjective impressions [10, 20,21,22]. There are few publications that quantitatively measure the amount of brow descent after SBB and compare it between different surgical approaches. In reviewing other papers, we found that ptosis of the brows was present almost in all methods, regardless of whether the orbicularis oculi was treated and irrespective of the use of suspension [9].
Several methods for measuring brow position have been reported [23, 24]. For example, using the ratio between the dimensions of the variable part and the unchanged part to demonstrate the reduction in brow-eye spacing does not yield a specific distance value [8, 25]. Other scholars have confirmed changes in the position of the eyebrow by measuring the distance of the eyebrow from the midline of the pupil [26, 27]. Since eyebrows are curved, we believe that drawing a horizontal straight line at the top of the brow to measure the vertical distance gives a better approximation of the brow position. This method is also very simple and easy to perform, requiring only drawing 3 parallel lines with the help of a software. Measurement includes determining the distance between the parallel lines and the pixel distance of the pupil, as reported by others [20, 28].
A simple measurement is used to quantify how much the eyebrow moves. Using the lower lid margin as the fixed point of origin, the pixel distance is converted to actual distance using a standardized pupil diameter for Asian women. It serves as a good reference in Asian populations and should continue to be used to analyze individuals, accounting for individual differences. Although previous studies have reported an elevation of the palpebrale inferioris with aging[29], the postoperative photographs involved in this study were taken within three months after surgery, so this issue can be ignored. The reason behind selecting a recent photograph less than 3 months old is that it is easy to follow up with a recent photograph. A recent photograph is deemed sufficient for illustrating the problem because the distance between the eyes and brows will be closer in the distant future, not further apart, under the effects of aging and gravity.
Measurement bias may occur due to the limited resolution of the images and precision of the measurement tools. Our results were measured three times by two researchers, and then the results were averaged. Measurements with large differences were further reviewed by a third authoritative expert to minimize potential measurement bias to the greatest extent.
This study has several limitations. The study was a retrospective study of only the simple subbrow blepharoplasty procedure without further comparison of the changes in brow position with different modifications of the procedure, in which only the skin and subcutaneous tissues were excised. Further studies with larger sample sizes should be conducted to further compare the effects of different modifications on brow position, to assess the effectiveness of different techniques in preventing brow descent, and to guide surgeons in the selection of surgical options.
The relatively small sample size included in this study, and the small number of patients included in certain groups when analyzed by subgroups according to follow-up time, make them susceptible to individual differences and make it difficult to draw more general conclusions. Due to the difficulty of postoperative follow-up of cosmetic patients, this study did not set up multiple follow-up time points for surgical outcomes, and the patients’ postoperative follow-up time ranged from the immediate postoperative period to 3 months postoperatively. A larger proportion of patients were followed up immediately after surgery. The results of the study showed that there was a decrease in the position of the eyebrows after surgery; however, the immediate postoperative period may have an impact on the results due to swelling and edema (Table 5). Therefore, in the future, multiple follow-up time points should be further set up to obtain data on changes in eyebrow position over time in the same patient for further analysis.
Our study suggests that the SBB is suitable for people with a wide distance between the eyes and brows, yielding better cosmetic results in those patients. Better clinical results are achieved in patients with high lateral brow and distant eyebrow spacing with inferior brow incisions. Blindly performing SBB without proper patient selection may result in postoperative proximity between the eyes and brows, potentially leading to a more severe and serious facial expression. Furthermore, it may exacerbate eye sagging, and the combined effect could cause a more aggressive expression.
Conclusions
We confirmed that there are changes in brow position after subbrow blepharoplasty. Significant brow descent can be observed after operation with the lateral eyebrow descending to a greater extent than the medial eyebrow. Some patients have improved facial proportions. Use of the lower lid margin as a fixed reference and pupil diameter for converting pixel distances to actual distances is an easy and feasible method for measuring and quantifying facial distances.
Reference
Fang YH, Liao WC, Ma H (2013) Infraeyebrow blepharoplasty incorporated browpexy in an Asian population. Ann Plast Surg 71(Suppl 1):S20–S24. https://doi.org/10.1097/SAP.0000000000000037
Lee D, Law V (2009) Subbrow blepharoplasty for upper eyelid rejuvenation in Asians. Aesthet Surg J 29(4):284–288. https://doi.org/10.1016/j.asj.2009.02.008
Shu M, He L, Su Y et al (2016) A novel supra-brow combined with infra-brow lift approach for Asian women. Aesthet Plast Surg 40(3):343–348. https://doi.org/10.1007/s00266-016-0632-y
Choi Y, Kang HG, Nam YS (2017) Three skin zones in the Asian upper eyelid pertaining to the Asian blepharoplasty. J Craniofac Surg 28(4):892–897. https://doi.org/10.1097/scs.0000000000003511
Kim YS, Roh TS, Yoo WM, Tark KC, Kim J (2008) Infrabrow excision blepharoplasty: applications and outcomes in upper blepharoplasty in Asian women. Plast Reconstr Surg 122(4):1199–1205. https://doi.org/10.1097/PRS.0b013e3181858fc0
Fagien S (1992) Eyebrow analysis after blepharoplasty in patients with brow ptosis. Ophthalmic Plast Reconstr Surg 8(3):210–214. https://doi.org/10.1097/00002341-199209000-00009
Alghoul MS, Vaca EE (2022) Creating harmonious arcs: the importance of brow shape in determining upper lid aesthetics. Clin Plast Surg 49(3):389–397. https://doi.org/10.1016/j.cps.2022.01.006
Xu L, Lee EI, Ma T, Zhang J, Han X, Ahn TJ (2022) Aesthetic analysis of alteration of eyebrow and forehead position after endoscopic eyebrow lift. Aesthet Plast Surg 46(5):2258–2265. https://doi.org/10.1007/s00266-021-02740-3
Kim YS (2014) Subbrow blepharoplasty using supraorbital rim periosteal fixation. Aesthet Plast Surg 38(1):27–31. https://doi.org/10.1007/s00266-013-0189-y
Jung GS (2020) Modified infrabrow excision blepharoplasty for severity of medial blepharochalasia. Plast Surg (Oakv). 28(3):167–171. https://doi.org/10.1177/2292550320928555
Yuezu L, Jun L, Jieying Z, Gang L (2022) Correlation between corneal biomechanical parameters and corneal diameter. Rec Adv Ophthalmol. 42(7):534–537. https://doi.org/10.13389/j.cnki.rao.2022.0109
Parkes ML, Kamer FM, Merrin ML (1976) Infrabrow lift. Laryngoscope 86(12):1869–1872. https://doi.org/10.1002/lary.5540861213
Branham G, Holds JB (2015) Brow/upper lid anatomy, aging and aesthetic analysis. Facial Plast Surg Clin North Am 23(2):117–127. https://doi.org/10.1016/j.fsc.2015.01.001
Gunter JP, Antrobus SD (1997) Aesthetic analysis of the eyebrows. Plast Reconstr Surg 99(7):1808–1816. https://doi.org/10.1097/00006534-199706000-00002
Kim HS, Kim KK (2020) Subbrow lift using frontalis sling to correct lateral orbital laxity. Aesthet Plast Surg 44(6):2119–2126. https://doi.org/10.1007/s00266-020-01879-9
Salinas CA, Liu A, Sharaf BA (2023) Analysis of hairline and forehead sexual dimorphic aesthetics in 60 celebrities using artificial intelligence. Plast Reconstr Surg Glob Open 11(7):e5107. https://doi.org/10.1097/gox.0000000000005107
Yaremchuk MJ, O’Sullivan N, Benslimane F (2007) Reversing brow lifts. Aesthet Surg J 27(4):367–375. https://doi.org/10.1016/j.asj.2007.05.008
Troilius C (1999) A comparison between subgaleal and subperiosteal brow lifts. Plast Reconstr Surg 104(4):1079–1090
Troilius C (2004) Subperiosteal brow lifts without fixation. Plast Reconstr Surg 114(6):1595–1603
Lee YJ, Kim S, Lee J, Chung JG, Jun YJ (2020) Parallel-excision infrabrow blepharoplasty with extensive excision of the orbicularis oculi muscle in an Asian population. Arch Plast Surg 47(2):171–177. https://doi.org/10.5999/aps.2019.01102
Wang J, Su Y, Zhang J, Guo P, Song B (2019) Subbrow blepharoplasty combined with periorbital muscle manipulation for periorbital rejuvenation in Asian women. Plast Reconstr Surg 144(5):760e–769e. https://doi.org/10.1097/PRS.0000000000006144
Kim SY, Ahn MR, Suh YC, Kim YJ, Lee JH (2019) Feasibility of a de-epithelialized orbicularis oculi musculocutaneous flap for subbrow blepharoplasty. Arch Aesthet Plast Surg 25(3):89–94. https://doi.org/10.14730/aaps.2019.01760
Wu XS, Jian XC, He ZJ, Gao X, Li Y, Zhong X (2010) Investigation of anthropometric measurements of anatomic structures of orbital soft tissue in 102 young han chinese adults. Ophthalmic Plast Reconstr Surg 26(5):339–343. https://doi.org/10.1097/IOP.0b013e3181c94e97
Rhee SC, Lee SH (2010) Attractive composite faces of different races. Aesthetic Plast Surg 34(6):800–801. https://doi.org/10.1007/s00266-010-9606-7
Xu L, Lee EI, Ma T, Zhang J, Han X, Ahn TJ (2020) Aesthetic analysis of alteration of eyebrow position after double eyelidplasty. Aesthet Plast Surg 44(2):373–378. https://doi.org/10.1007/s00266-019-01590-4
Rhee SC, Woo KS, Kwon B (2012) Biometric study of eyelid shape and dimensions of different races with references to beauty. Aesthet Plast Surg 36(5):1236–1245. https://doi.org/10.1007/s00266-012-9937-7
Lee TY, Kim HK, Choi DI (2023) Reducing the volume of upper eyelids in east asians increases vertical palpebral height. Aesthet Plast Surg 47(5):1835–1842. https://doi.org/10.1007/s00266-023-03333-y
Hadlock TA, Urban LS (2012) Toward a universal, automated facial measurement tool in facial reanimation. Arch Facial Plast Surg 14(4):277–282. https://doi.org/10.1001/archfacial.2012.111
Park DH, Choi WS, Yoon SH, Song CH (2008) Anthropometry of asian eyelids by age. Plast Reconstr Surg 121(4):1405–1413. https://doi.org/10.1097/01.prs.0000304608.33432.67
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This article does not contain any studies with human participants or animals performed by any of the author.
Human or Animal Rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
The participants have given written informed consent for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xu, L., Zhong, X. & Wang, T. Quantitative and Aesthetic Analysis of Changes in Eyebrow Position After Subbrow Blepharoplasty. Aesth Plast Surg (2024). https://doi.org/10.1007/s00266-024-04255-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00266-024-04255-z