
Abstract
Background
The correction of tear trough deformity poses a significant challenge in the context of facial rejuvenation. Our aim was to introduce a technique that corrects tear trough deformity during transconjunctival lower blepharoplasty using minced orbital fat grafts.
Methods
The medical records of patients who underwent lower blepharoplasty from January 2019 to December 2021 were reviewed. The study included patients with various grades of tear trough deformity, who underwent lower blepharoplasty using minced orbital fat grafts and followed up for at least 6 months. Modified Barton’s grading for tear trough depression, patient satisfaction, and postoperative complications were evaluated.
Results
A total of ninety-eight patients, with a mean age of 48.07 ± 9.72 years, consisting of 93 (94.9%) females were included in the study. The average duration of follow-up was 7.2 months, ranging from 6 to 13 months. Tear trough depression significantly improved after the operation (preoperative tear trough depression grade mean (SD): 3.11 (0.60); postoperative tear trough depression grade mean (SD): 0.87 (0.66); P < 0.001). 78.5% of the participants reported their outcome as excellent or good, 20.4% reported as fair, and 1.0% (only one patient) reported as no improvement. None of the participants rated their outcome as worsening. No major complication was observed during the follow-up period.
Conclusion
Minced orbital fat grafting during transconjunctival lower eyelid blepharoplasty has good effectiveness for correcting tear trough deformity without the risk of major complications.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The correction of tear trough deformity can significantly improve the overall appearance of the face and alter the way an individual is perceived by others. Therefore, it is essential to address this deformity as a crucial aspect of any procedure intended to rejuvenate the face [1].
The initial blepharoplasty surgeries only aimed to remove the excess fat pads. While these approaches could address bulging of the lower eyelid, they could not correct tear trough deformity [2]. Years later, lower blepharoplasty with fat repositioning was introduced to address tear trough deformity [3]. However, entrapment of the inferior oblique muscle between the transposed pedicles which causes diplopia, lumpiness over tear trough deformity, and limitation of the degree to which pedicled fat can be translocated, are some of the drawbacks of fat repositioning approaches [4, 5]. Another commonly employed technique for effacing tear trough deformity is autologous fat grafting from distant donor sites. The main problem with this method is the low survival rate of the grafted fat tissue [6]. Fat embolism, physiological incompatibility, and volume change of the grafted fat with body weight change, are other shortcomings of this technique [7, 8].
In the present study, we assessed the safety and effectiveness of a technique for obliterating tear trough deformity which comprises transconjunctival fat excision followed by minced orbital fat grafting.
Materials and Methods
Study Population and Selection Criteria
In this retrospective study, all patients who had transconjunctival fat excision followed by minced orbital fat grafting from January 2019 to December 2021 at a private oculoplastic office were included. Patients with various grades of tear trough deformity and a follow-up duration of at least 6 months met the inclusion criteria. Individuals who had a history of prior surgeries on the eyelids or periorbital area, patients who had received dermal filler injections to address tear trough deformity, patients who had undergone midface lifts, and those who lacked adequate quality photos were excluded. A single oculoplastic surgeon (A.H.) performed all the operations.
Our study followed the principles of the Declaration of Helsinki and received approval from the ethics committee of our institution (IR.ARI.MUI.REC.1402.136). All patients signed written informed consent forms.
Data Collection
After surgery, patients were followed at the intervals of one week, one month, and six months. Preoperative and postoperative frontal photos taken in a standard head position were utilized for measurements and comparisons. The preoperative photographs captured closest to the date of the surgery and postoperative photographs captured at the most recent follow-up visit were used to measure the depth of tear trough. Complications were evaluated at every follow-up appointment. From the first preoperative visit until the final postoperative visit, clinic notes and photographs were reviewed by an experienced oculoplastic surgeon (B.A.) who had not been involved in the surgery to assess outcomes and complications. Each eye was assessed separately due to the lack of complete symmetry between them. The depth of the tear trough was scored from 0-4, based on a modified version of Barton’s grading system [9, 10] and is summarized in Table 1. At the final visit, patients were requested to report their level of satisfaction regarding the results of the surgery using a scale that ranges from 1 to 5 (5, excellent; 4, good; 3, fair; 2, no improvement; 1, worsening).
Partial fat graft resorption was defined as partial volume loss from previous examinations. Complete fat graft resorption was characterized as complete volume loss and recurrence of the preoperative tear trough (through inspection and palpation).
Surgical Procedure
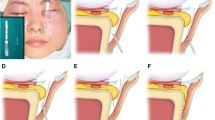
The operation was performed under conscious sedation or general anesthesia. Lidocaine 2% containing 1:200 000 epinephrine was injected into the conjunctiva, each lateral, medial, and central infraorbital fat pad. The lower lid was retracted caudally and a conjunctival incision was made 1–2 mm below the inferior margin of the tarsus. Through the conjunctival incision, a blunt dissection was performed between the orbicularis oculi muscle and the septum and extended to the level of the orbital rim. With careful attention to avoid harming the inferior oblique muscle (between the central and medial fat pads), the septum was incised beside the arcus marginalis, and medial, central, and lateral fat pads were resected (Supplemental Digital Content 1). The orbital retaining ligament was released either in the tear trough or throughout the entire orbital rim, depending on patient’s need. Then the dissection continued between the orbicularis oculi muscle and periosteum, medial to infraorbital nerve, in prezygomatic space, and in some cases in palpebromalar groove, lateral to the nerve. The dissection was narrow at the top point, near the orbital rim, and continued downwards in a fan shape (like a funnel) to create a wider pocket under the orbicularis muscle. Multiple small funnel-shaped dissections were created, depending on patient’s need, to prevent displacement of the fat grafts. This dissection technique has also the advantage of minimizing the orbicularis muscle injury (Supplemental Digital Content 2). The resected fat pads were minced into 4- to 5-mm grafts (Fig. 1) and based on the depth of the area of deformity, the appropriate amount of fat was positioned to the area of deformity (Fig. 2, Supplemental Digital Content 3). A 6.0 Vicryl suture was placed through the orbicularis muscle at the entrance point of the fat pads to prevent graft displacement. In cases where an excess of skin was present, it was excised in a conservative manner using the subciliary skin pinch technique. Canthopexy was done in the presence of lid laxity according to the distraction test. The conjunctival incision was closed with Vicryl 6.0.

The resected orbital fat pads are minced into 4- to 5-mm grafts using scissors

Placement of minced orbital fat grafts into tear trough deformity
Postoperative Care
We dressed the surgical site for 3 to 4 days and advised patients against massaging or applying pressure to the area to prevent the displacement of fat grafts. Additionally, we recommended that patients avoid intense physical activities for three weeks and bending for one week after the surgery. We also requested the patients to use cold packs on the surgical site for the initial 2–3 days following the procedure, with intervals of 20–30 minutes separated by 2 hours.
Statistical Analysis
Descriptive statistics were utilized to report tear trough depression grades, patient satisfaction, and postoperative complications. For categorical variables, numbers and percentages were reported, and for continuous variables, means and standard deviation were computed. To compare the tear trough depression grades before and after the operation, a paired sample t-test was used. A P value of < 0.05 was considered significant. Data analysis was performed using SPSS version 21.0 statistical package (SPSS Inc., Chicago, IL, USA).
Results
We enrolled a total of 98 patients (196 eyelids) with a mean (SD) age of 48.07 (9.72) years in our study. Ninety-three (94.9%) of the study population were female. The average duration of follow-up was 7.2 months (range, 6–13 months). The duration for the surgical procedure of both lower eyelids was approximately 45 minutes.
Comparison of grades for tear trough depression before and after surgery showed a significant improvement in the mean grade from preoperative to postoperative (mean tear trough depression grade before the operation was 3.11 ± 0.60 which improved to 0.87 ± 0.66 after the operation; P < 0.001) (Figs. 3, 4, 5, 6, 7). Preoperative and postoperative tear trough depression grades are listed in Table 2.

Tear trough depth before and after surgery

Preoperative view of a 54-year-old female patient presented with a tear trough deformity and herniated fat pads (left). Postoperative view after transconjunctival lower lid blepharoplasty with transposition of minced fat grafts (right)

Preoperative view of a 50-year-old female patient presented with a tear trough deformity and herniated fat pads (left). Postoperative view after transconjunctival lower lid blepharoplasty with transposition of minced fat grafts (right)

Preoperative view of a 40-year-old female patient presented with a tear trough deformity and herniated fat pads (left). Postoperative view after transconjunctival lower lid blepharoplasty with transposition of minced fat grafts (right)

Preoperative view of a 45-year-old female patient presented with a tear trough deformity and herniated fat pads (left). Postoperative view after transconjunctival lower lid blepharoplasty with transposition of minced fat grafts (right)
Fifty-one (52.0%) participants reported their outcome as “excellent”, 26 (26.5%) reported as “good”, 20 (20.4%) reported as “fair”, and only one (1.0%) reported as “no improvement”. None of the participants rated their outcome as “worsening”.
Postoperative Complications
Postoperative complications are shown in Table 3. Eyelid retraction was observed in 6 (3.1%) eyelids and was less than one millimeter in all of them. Complete fat graft resorption occurred in none of the eyelids and Partial fat graft resorption occurred in 16 (8.2%) eyelids. One (1.0%) patient experienced transient anesthesia near the nose. No cases of overcorrection and 10 (5.1%) cases of undercorrection were observed. Two (1.0%) eyelids required re-excision of the Lateral fat pad.
Discussion
Traditional lower blepharoplasties only involved removal of infraorbital fat through an external method. Complications like lower lid retraction led to proposing transconjunctival approach in 1924 which reduced the scleral show rate from 28 to 3% [2, 11, 12]. Prior to this point in time, the main focus of blepharoplasty was solely on the protrusion of the lower eyelid and did not target the tear trough defect [13]. In 1981, Loeb [14] introduced the transposition of the medial portion of lower lid fat to correct tear trough deformity. Hamra later described the arcus marginalis release technique, in which all the lower lid fat is moved across the orbital rim to correct both the tear trough deformity and the palpebromalar sulcus [15]. Autologous fat grafting from distant donor sites is another approach to correct tear trough deformity [16].
Fat repositioning has the potential downside of middle lamella violation, which can lead to contraction, shortening, and higher rates of eyelid retraction [17]. As described, our technique minimizes the risk of orbicularis muscle and middle lamella injury which results in lower rates of lid retraction. In fat relocation, failure to fully release the fat pedicles or fibrosis of the pedicles could lead to a recurrence of the deformity of the tear trough [3]. Eye motility disturbance due to the inferior oblique muscle entrapment is another disadvantage of fat repositioning which is omitted in our technique [4].
In fat transposition, the location to which pedicled fat can reach is limited due to the tethering of the pedicle. However, free fat grafts in our technique can be located more precisely in the deep medial part of the tear trough which is difficult in fat transposition. Our approach enables us to cover a wider surface area with multiple minced fat grafts. However, in fat repositioning, it is only possible to cover a surface area as wide as the width of repositioned fat.
Despite these disadvantages, transposed pedicled fat has better blood supply compared with free fat graft in our technique which theoretically results in better survival of pedicled fat (although, transposed pedicled fat is a random flap with poor vascularization, which may not actually offer much better blood flow than a free fat graft [18]). We tried to improve the blood supply of the free fat grafts by avoiding the use of large-sized fat grafts, not placing too much fat in each funnel-shaped dissection, and refraining from stacking the fat grafts. A recent study that compared the results of these two surgical techniques showed that the rate of complications and patient satisfaction do not significantly differ between these two approaches; however, it did not compare the survival rate of the fat particles between these two methods [19]. According to the results of the beforementioned study and the lack of human study supporting higher survival for transposed pedicled fat vs free fat graft, it’s reasonable to view free fat grafting as a viable alternative for restoring volume in the periocular area. The excellent outcome of our surgical approach in correcting tear trough deformity is not solely a result of minced fat grafting; part of it also arises from releasing the orbital retaining ligament. Releasing the orbital retaining ligament is also a step of surgery in transposing the pedicled fat grafts. As mentioned, autologous fat grafting from distant donor sites is another approach for effacing tear trough deformity. The primary issue in this technique is fat resorption. The survival rate of the injected fat over a year is estimated to be only about 30% [20]. In this procedure, fat is harvested from distant body locations through liposuction and then injected into tear trough [6]. Fat liposuction and centrifugation procedures rupture a large number of adipocytes [21]. Animal studies have shown that surgically excised fat grafts have better survival rate than the suctioned and centrifuged ones [22, 23]. Liposuction and centrifugation are eliminated in our method which can theoretically enhance the survival rate of the fat grafts. However, to the best of our knowledge, there is not any study on human subjects that have compared the survival rate of fat grafts from distant donor sites and lower eyelid and this should be assessed in future studies.
In contrast to our approach, tear trough ligament which plays an important role in tear trough deformity, is not released during autologous fat grafting which decreases the effectiveness of this method for correcting the tear trough deformity [24]. Subcutaneous induration which causes contour irregularities is another shortcoming of autologous fat grafting [25]. Compared with distant donor sites fat graft, another benefit of lower lid fat graft is its physiological and biocompatible nature. It is noteworthy that orbital fat is the only type of fat in the body that its volume remains unchanged, even with an increase in body weight [7]. Furthermore, our procedure does not have the risk of intravascular lipoinjection which can result in serious complications like blindness and stroke [8]. Our approach also eliminates the inconvenience of two-step surgery and distant donor sites morbidity.
We observed a relatively high incidence of about 10% skin irregularity following our surgical procedure. However, most of the skin irregularities were reported by the surgeon, including even the minor ones, and only a few of them were our patients’ complaints. Upon further investigation, we found that the high incidence of skin irregularities can be attributed to the creation of a few number of funnel-shaped dissections and placing excessive fat grafts in each tunnel. In the subsequent cases, we created more funnel-shaped dissections and used a smaller number of fat grafts in each tunnel which allowed us to distribute the fat grafts more evenly in the area of deformity and considerably reduced the skin irregularities. Consequently, the skin irregularities were predominantly observed in our initial cases and were rarely detected in the subsequent cases. Although we suggested corticosteroids injection for prominent areas and filler injection for depressed areas for the affected cases, our patients declined the treatment.
Previous studies have also employed minced orbital fat grafting with some variations to the technique used in our study and all reported good safety and efficacy [6, 17, 26]. However, it is important to be aware of the potential risks when utilizing a new technique for the first time, as incorrect application or inappropriate patient selection can result in unsatisfactory results and complications for any surgeon.
It is widely agreed that in order to correct tear trough deformity, one must not only address the herniation of orbital fat, but also add volume to the tear trough deformity [4]. There are many factors to consider, and as a result, there are numerous treatment options available, each with its pros and cons. The surgeon must determine the safest and most effective approach that produces the desired aesthetic result without compromising the functionality of the lower eyelid. The ultimate goal is to provide a personalized aesthetic result for each patient.
Limitations
Our study has the inherent limitations of the retrospective design. The rather short period of follow-up restricted assessing the long-term effectiveness and complications of our new method. Lack of a comparison group prevented us from comparing the outcomes of our procedure with other techniques. Similar to previous studies, assessing the results of periorbital surgery mainly depends on the subjective feedback from surgeons and patients regarding their satisfaction and is hampered due to the absence of universally recognized objective criteria [3]. The modified version of Barton’s grading system has grades ranging from 0 to 4, which makes it challenging to detect subtle differences. A more homogeneous approach to our surgical method would be preferable. For instance, canthopexy and releasing the orbital retaining ligament throughout the entire orbital rim were not performed for all the patients. Finally, we acknowledge that our study does not possess the advantage of evaluating signs of periocular aging beyond the tear trough deformity.
Conclusions
Our study demonstrated that the use of minced orbital fat grafts for correcting the tear trough deformity during transconjunctival lower blepharoplasty is a satisfactory procedure, without the risk of major complications. Future studies with longer follow-up time and a comparison group are needed to assess its efficacy.
References
Innocenti A, Melita D, Ghezzi S, Innocenti M (2018) Refinements in tear trough deformity correction: intraoral release of tear trough ligaments: anatomical consideration and clinical approach. Aesthet Plast Surg 42:1576–1581
Maffi TR, Chang S, Friedland JA (2011) Traditional lower blepharoplasty: is additional support necessary? A 30-year review. Plast Reconstr Surg 128(1):265–273
Atiyeh B, Hakim CR, Oneisi A, Ghieh F, Chahine F (2023) Surgical correction of tear trough deformity (TTD) with orbicularis retaining ligament release and volume augmentation for periorbital rejuvenation: review of the literature. Aesthet Plast Surg 47(1):199–214
Goldberg RA (2000) Transconjunctival orbital fat repositioning: transposition of orbital fat pedicles into a subperiosteal pocket. Plast Reconstr Surg 105(2):743–748
Liao SL, Wei YH (2011) Fat repositioning via supraperiosteal dissection with internal fixation for tear trough deformity in an Asian population. Graefes Arch Clin Exp Ophthalmol 249:1735–1741
Miranda SG, Codner MA (2017) Micro free orbital fat grafts to the tear trough deformity during lower blepharoplasty. Plast Reconstr Surg 139(6):1335–1343
Pascali M, Quarato D, Pagnoni M, Carinci F (2017) Tear trough deformity: study of filling procedures for its correction. J Craniofac Surg 28(8):2012–2015
Lee CM, Hong IH, Park SP (2011) Ophthalmic artery obstruction and cerebral infarction following periocular injection of autologous fat. Korean J Ophthalmol 25(5):358–361
Barton FE Jr, Ha R, Awada M (2004) Fat extrusion and septal reset in patients with the tear trough triad: a critical appraisal. Plast Reconstr Surg 113(7):2115–2121
Ramesh S, Goldberg RA, Wulc AE, Brackup AB (2019) Objective comparison of nasojugal fold depth and lower eyelid length after fat excision versus fat transpositional lower blepharoplasty. Aesthet Surg J 39(10):1048–1054
Bourguet J (1924) Les hernies graisseuses de l’orbite: notre traitement chirurgical. Bull Acad Med (Paris) 92(3):1270
Schwarz F, Randall P (1980) Conjunctival incision for herniated orbital fat. Ophthalmic Surg 11(4):276–279
Loeb R (1993) Naso-jugal groove leveling with fat tissue. Clin Plast Surg 20(2):393–400
Loeb R (1981) Fat pad sliding and fat grafting for leveling lid depressions. Clin Plast Surg 8(4):757–776
Hamra ST (1995) Arcus marginalis release and orbital fat preservation in midface rejuvenation. Plast Reconstr Surg 96(2):354–362
Chiu C-Y, Shen Y-C, Zhao Q-F, Hong F-L, Xu J-H (2017) Treatment of tear trough deformity: fat repositioning versus autologous fat grafting. Aesthet Plast Surg 41:73–80
Kim HS, Choi CW, Kim BR, Youn SW (2019) Effectiveness of transconjunctival fat removal and resected fat grafting for lower eye bag and tear trough deformity. JAMA Facial Plast Surg 21(2):118–124
Goldberg RA (2017) Discussion: micro free orbital fat grafts to the tear trough deformity during lower blepharoplasty. Plast Reconstr Surg 139(6):1344–1345
Karimi N, Kashkouli MB, Enayatollahi S, Ghahvehchian H, Abdolalizadeh P, Ramadan M (2023) Minced free fat graft versus pedicle fat flap to efface orbital rim hollow in lower blepharoplasty. Aesthet Surg J 44(1):12–19
ASPRS Ad-Hoc Committee (1987) Report on autologous fat transplantation. ASPRS Ad-Hoc Committee on new procedures. Plast Surg Nurs 7:140–141
Choo PH, Carter SR, Seiff SR (1998) Lower eyelid volume augmentation with fat pearl grafting. Plast Reconstr Surg 102(5):1716–1719
Fagrell D, Eneström S, Berggren A, Kniola B (1996) Fat cylinder transplantation: an experimental comparative study of three different kinds of fat transplants. Plast Reconstr Surg 98(1):90–96
Kononas TC, Bucky LP, Hurley C, May JW Jr (1993) The fate of suctioned and surgically removed fat after reimplantation for soft-tissue augmentation: a volumetric and histologic study in the rabbit. Plast Reconstr Surg 91(5):763–768
Wong C-H, Hsieh MK, Mendelson B (2012) The tear trough ligament: anatomical basis for the tear trough deformity. Plast Reconstr Surg 129(6):1392–1402
Coleman SR (2008) Lower lid deformity secondary to autogenous fat transfer: a cautionary tale. Aesthet Plast Surg 32:415–417
Lee W, Cho J-K, Koh I-S, Kim HM, Yang E-J (2020) Infraorbital groove correction by microfat injection after lower blepharoplasty. J Plast Reconstr Aesthet Surg 73(4):777–782
Acknowledgement
We would like to acknowledge that Dr. Iman Mohammadbeigy and Dr. Abtin Heirati have contributed equally to this work and should be considered co-first authors of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from all of the participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (WMV 63886 KB)
Supplementary file2 (WMV 70854 KB)
Supplementary file3 (WMV 58667 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Heirati, A., Mohammadbeigy, I., Pourazizi, M. et al. Correction of Tear Trough Deformity with Minced Orbital Fat Grafts During Transconjunctival Lower Blepharoplasty. Aesth Plast Surg 48, 2778–2785 (2024). https://doi.org/10.1007/s00266-024-04086-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-024-04086-y