
Abstract
Background
Cryolipolysis is a non-invasive and efficacious procedure for body contouring. The effectiveness of cryolipolysis has been demonstrated on multiple areas of the body, but on a limited number of subjects. The aim of this study is to demonstrate the effectiveness and the safety of cryolipolysis in the lower abdomen adipose tissue thickness reduction.
Methods
A prospective study on 60 healthy women was carried out using CryoSlim Hybrid device. Each patient underwent two cryolipolysis sessions centered on the abdominal area. The primary endpoint was to decrease the thickness of the abdominal fat deposits. The change in the abdominal circumference and the thickness of the subcutaneous fat layer were assessed. Patient satisfaction and tolerance of the procedure were also taken into account.
Results
A significant reduction of the abdominal circumference and subcutaneous fat layer thickness was observed. The mean decrease in abdominal circumference was 2.10 cm (3.1%) 3 months after the procedure and 4.03 cm (5.8%) 6 months after the procedure. The mean decrease in fat layer thickness was 1.25 cm (43.81%) 3 months after the procedure and 1.61 cm (41.73%) 6 months after the procedure. No major adverse events were noted. All patients were very satisfied, and minimal pain was reported.
Conclusions
Cryolipolysis is an effective technique to treat abdominal localized fat deposits. No major adverse events have been described for this procedure. Our promising results should encourage further studies aimed at optimizing the efficacy of the procedure without a considerable increase in the risks.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors http://www.springer.com/00266.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In our contemporary society, a modern perception of the human body is accompanied by an increasing demand for body-shaping procedures. The ideal treatment should be effective, safe, fast and easily integrated into the daily working and routine schedule. Options available for a minimally invasive procedure are still limited [1,2,3,4,5,6,7]. Cryolipolysis is a minimally invasive technique of body reshaping which allows fat cell depots reduction through local application of low temperatures.
Cryolipolysis is FDA approved since 2010 and represents a minimally invasive alternative to liposuction aimed at debulking subcutaneous fat. The effects on the adjacent tissues are minimal [8, 9]. Cryolipolysis causes adipocytes apoptosis and loss of subcutaneous fat. Fatty tissue is electively sensitive to cold temperatures thanks to the popsicle panniculitis effect, a condition in which cytoplasmic lipids contained in fat cells crystalize at higher temperatures than tissular water [10]. It has been demonstrated that a single cycle of cryolipolysis results in considerable macrophage recruitment over the post-procedural 2 weeks. Then, macrophage recruitment peaks 4 weeks after cryolipolysis and subsides after the 12th week. The adipocytes apoptotic rate is increased due to panniculitis in the early and late post-procedural phase causing notable fat thickness decrease [11, 12]. The efficacy of cryolipolysis in humans has been only demonstrated through the accurate analysis of pre-procedural and post-procedural images. However, its efficacy on subcutaneous adipose tissue has not been demonstrated yet [13].
The study is aimed at demonstrating the effectiveness and reliability of cryolipolysis for abdominal fat thickness reduction.
Patients and Methods
The authors conducted a prospective study on healthy women to assess the efficacy and the reliability of cryolipolysis on lower abdominal fat deposits. Inclusion criteria were women ≥ 18 years of age with a BMI < 30 and abdominal fat deposits. Exclusion criteria were recent (< 18 months) liposuction and/or abdominoplasty and/or bariatric surgery, medical history of an eating disorder and patients with excess abdominal skin for whom abdominoplasty was indicated.
This study was carried out in accordance with the globally accepted standards of Good Clinical Practice (ICH-E6) (European Directive 2001/20/EC) and the revised version of the Declaration of Helsinki. Sixty healthy female patients presenting with abdominal fat volunteered to be included in the study. All patients taking part in the study signed a written informed consent.
Two cryolipolysis sessions (one-month interval) were carried out on every patient. Pre-procedural weight, body mass index (BMI), abdominal circumference measurements and ultrasonography scans were carried out. The same measurements were repeated 3 and 6 months after the procedure.
The primary objective of the study was to observe a reduction in the thickness of the abdominal adipose deposits. To prove so, systematic abdominal circumference measurements and ultrasound scans of the subcutaneous fat were carried out on a 0, 3 and 6 months timeline. Abdominal circumference (in centimeters) was measured by the same operator (first author EC); the greater abdominal circumference was measured on the standing patient (feet brought together). A Vscan ultrasonography device (GE Healthcare, Vingmed Ultrasound AS, Horten, Norway) was used to appreciate the thickness of the subcutaneous fat layer (over the most projected areas of the fat deposit) on time 0 and 3 and 6 months post-procedurally. Thigh circumference (cm) and subcutaneous fat thickness were also measured on time 0 and 3 and 6 months post-procedurally and used as a control untreated area. Measurement was made on both thighs at the greater trochanter, with the patient standing (feet brought together).
A Visual Analog Scale (VAS), ranging from 0 (no pain) to 10 (severe pain), was used to evaluate patient’s tolerance to the procedure. Secondary effects were noted. Front, posterior, right profile and left profile images were collected before the first session and at 3 and 6 months after the last session for each patient. Six months after the last procedure, patients were requested to complete a satisfaction questionnaire.
Procedure
A CryoSlim Hybrid (BFP Electronique, Montrodat, France) device was used.
The CryoSlim Hybrid is a cryolipolysis device which uses the cold to generate the apoptosis effect to reduce the fat volume. Patented for its cooling system hermetical, the CryoSlim Hybrid is effective from 0 °C to – 5 °C of treatment temperature while most part of other Cryolipolysis devices must use lower temperatures (− 10 °C) to get results [12, 13]. CryoSlim uses a patented handpiece with 4 Peltier heat extractors to generate homogenous cold throughout the application area. The CryoSlim Hybrid software is able to recognize and treat the entire depth of the subcutaneous fat layer, excluding other tissues. Thanks to its hermetic cooling system, CryoSlim Hybrid concentrates the cold only on the patient adipocyte cell layer and avoids crystallization of adjacent tissues: blood, lymph, nerves, or muscles, which can cause side effects. The CryoSlim Hybrid uses its own interactive software called USER ASSIST to evaluate the volume and type of fat in treatment. USER ASSIST communicates in live with the user to confirm that the treatment is well done or advices on how optimize it. With this capacity to evaluate and communicate with the user, USER ASSIST avoids wrong treatments and optimizes the results.
The sessions were carried out by the same physician (first author EC) for each patient. The treatment protocol consisted of two 55 minutes sessions at a temperature of −5 Celsius degrees and a negative pressure of −450 mbar centered on the abdominal area, followed by 5 minutes of energetic massage. The hand-pieces were directly applied to the skin; straps were not required since the negative pressure of −300 mbar enhanced the hand-piece fixation to the skin. Soft cushions were placed around the hand-pieces to improve patient comfort and prevent tissues from being displaced by the weight of the hand-pieces. The oval hand-pieces (25 × 15 cm) adapted well to the size and shape of the abdomen. All patients were requested to lay supine during the procedure. Peri-procedural analgesia and sedation were not required. All studied patients were allowed to resume their daily activities immediately after the treatment sessions and were asked not to modify their usual lifestyle (diet and exercise) during the post-procedural 6 months.
Statistical Analysis
All data were presented as mean ± SD. The analysis of continuous variables was conducted through Student’s T test. A value of p < 0.05 was considered statistically significant.
Statistical analysis was conducted through the PRISM software, version 7 (Graph Pad, USA).
Results
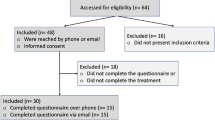
Sixty patients were included in the study, and six were lost to follow-up (two at the 3 months appointment and four at the 6 months appointment). The results for the remaining 54 patients were included in the final analysis. The follow-up time ranged from 12 to 18 months (15.32 ± 3.2). The mean age of the patients was 35 ± 13 years. The mean weight of the patients was 60.23 ± 8.3 Kg at time 0, 60.22 ± 8.3 Kg three months after the last procedure and 60.22 ± 7.8 Kg at six months follow-up (p = 0.47).
The mean body mass index was 23.62 ± 2.1 kg/m2 on time 0, 23.32 ± 3.41 kg/m2 3 months post-procedurally, and 23.21 ± 2.8 kg/m2 6 months post-procedurally (p = 0.55). The mean abdominal circumference was 95.6 ± 9.5 cm on time 0, 93.61 ± 5.65 cm 3 months post-procedurally (p = 0.005), and 91.57 ± 8.21 cm 6 months post-procedurally (p = 0.0004) (Table 1). The mean decrease in the abdominal circumference was 2.10 cm (3.1%) 3 months post-procedurally and 4.03 cm (5.8%) 6 months post-procedurally (Figures 1, 2). The mean subcutaneous fat layer thickness was recorded as 3.7 ± 2.51 cm on day 0, 2.45 ± 2.35 cm 3 months post-procedurally (p = 0.0003), and 2.1±0.27 cm at 6 months post-procedurally (p < 0.001) (Table 1). The mean decrease in fat layer thickness was 1.25 cm (43.81%) 3 months post-procedurally and 1.61 cm (41.73%) 6 months post-procedurally (Figure 3). No significant differences were observed in thigh circumference and subcutaneous fat thickness after the cryolipolysis sessions (Table 2). No major complications were observed. All patients experienced erythema after the session, which subsided after a mean of 15 hours. Temporary skin hyperpigmentation or discoloration (in black patients) of the treated area was observed on day 45 in three patients (5.55%). This event usually spontaneously resolved within one week after the treatment. For one patient, dyschromia persisted up to 6 months after the procedure but was significantly reduced (Figure 4). One year after the procedure, pigmentation subsided completely. Delayed adverse events were not observed in any patient. Patient satisfaction was assessed [6 months after the second treatment session] through a questionnaire. Most of the patients were satisfied with the results of the procedure. Fifty of the treated patients (92.59%) stated that they would recommend cryolipolysis of the abdomen to their friends (Table 3). The mean visual analog scale score was 1.66 ± 0.33 of 10 after the first session and 1.45 ± 0.41 of 10 after the second session.

Photographs of a 38-year-old patient with abdominal fat deposits on day 0 (a, b) and 6 months after the second treatment (c, d)

Photographs of a 41-year-old patient on day 0 (a, b) and 6 months after 2 cryolipolysis sessions (c, d)

US Scans of a 37-year-old patient included in the study. The abdominal subcutaneous fat layer thickness was recorded as 3.5 cm before the procedure (a), and 2.6 cm 6 months after (b). The white arrow indicates the fascia, and the red line is the thickness of the subcutaneous tissue. A significant reduction in fat layer thickness was observed

Example of cryolipolysis-induced hyperpigmentation. The photograph was taken 15 days after treatment (a). A significant decrease in hyperpigmentation was observed 6 months after the last treatment session (b)
Discussion
Authors assessed the efficacy of cryolipolysis on subcutaneous abdominal fat reduction. A new device (CryoSlim Hybrid, BFP Electronique, Montrodat, France) was tested. The effectiveness of the procedure was demonstrated thanks to a significant decrease in the subcutaneous fat and abdominal circumference (p < 0.001). In this prospective study, the treated area was compared to a control untreated area in order to investigate whether the results were influenced by other factors. Since no changes in the control area were detected, the authors assumed that no other factors (such as diet, exercise, drugs, and diseases) had interfered with the outcomes, so the observed results were exclusively due to cryolipolysis.
Furthermore, no significant change was observed in the average weight and average BMI of the patients before and after treatment, so we can exclude that the reduction in subcutaneous adipose tissue and abdominal circumference was due to weight loss and assume that the favorable results are only related to the treatment.
Few minor and transient side effects were observed. One case of persistent hyperpigmentation was reported. Overall patient satisfaction was high. Minor complications such as erythema, bruising, edema, impaired sensitivity and pain (usually subsiding few weeks after the treatment) were reported in previous studies [14,15,16,17,18,19].
Garibyan et al. demonstrated the integrity of the adjacent tissues after the application of low temperatures and the efficacious reduction of the subcutaneous fat. Tissue rearrangements were observed after exposure to low temperatures. Moreover, cold saline injections were carried out in the subcutaneous tissue: No muscular, nervous, cutaneous or systemic side effect were noted. Also, no scarring or damage to the adjacent tissues was noted [15].
Only few studies about the effects of cryolipolysis on subcutaneous fat have been recently carried out. Accurate metabolic analyses confirmed that, after exposure to low temperatures, the metabolism of adipose cells changes, and the observed alterations persist up to 75 days after the session. Also, the histopathological analysis reports described substantial modifications of adipose tissue architecture. Considerable inflammation due to the adipose cell apoptosis was observed 72 hours after the procedure. One month after the procedure, inflammation began to subside. Two months after the procedure, significant fibrosis of the interlobular septa was observed. Adipocytes were not found in the treated areas [16, 17].
The authors have recently carried out a study about the outcomes of cryolipolysis on the saddlebag area. A considerable reduction of the thigh circumference (in centimeters) and subcutaneous fat layer was noted [17]. A recent review reported an average decrease of 19.6% in the subcutaneous fat layer in the submental area after cryolipolysis [20]. These recently published results led to a rise in popularity of cryolipolysis since it is a minimally invasive and efficacious technique.
Hwang et al. performed a study on 19 patients who had undergone cryolipolysis of the abdomen. A decrease in the visceral fat layer was observed after a single session of cryolipolysis of the abdominal area, 1 week after the procedure. The CT scan showed a reduction of 6.8 cm2 after the procedure (15.6%; p = 0.003) compared to the contralateral untreated side and a decrease of 1.2 cm2 (3.6%). No effects were noted on the abdominal fat [21].
Falster et al. carried out a similar study on 34 patients undergoing a single cryolipolysis session. No reduction in the abdominal fat layer was noted 30, 60 and 90 days after the procedure [22]. Regarding long-term effects, Bernstein showed that the outcomes of cryolipolysis persisted up to 5 years after the procedure and adipose tissue did not regenerate in the adjacent areas [23].
Post-procedural dyschromia (hypopigmentation or hyperpigmentation) has also been described [17,18,19,20,21,22,23,24]. Most frequently, dyschromia occurred in patients presenting with a dark skin phototype (Fitzpatrick type III/IV) and subsided few months later [25]. Burns and hemosiderin deposits in the dermis would be responsible for hyperpigmentation [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44]. The use of an interposed layer may decrease the likelihood of this complication. Before undergoing cryolipolysis, patients should be informed of the risk of complications (such as hyperpigmentation or erythema, usually occurring 15 hr after cryolipolysis). The risk of skin lesions is minimal compared to liposuction, which systematically causes significant post-operative bruising and pain due to thin subcutaneous hematomas. Patients should also be consented and informed of the risk of paradoxical adipose hyperplasia, which occurs in one in 20,000 treated patients (an incidence rate of 0.0051%). However, the risk of developing skin lesions in the long term is still unknown [14]. Cryolipolysis is not indicated in patients suffering from Raynaud's Syndrome or cryoglobulinemia, cold urticaria, severe varicose veins (aggravated by low temperatures).
Our study included a larger number of patients (54 patients) compared to other studies on cryolipolysis. Also, the mean follow-up time was longer (15.32 ± 3.2 months on average).
The treatment protocol promoted a considerable reduction of the abdominal circumference and (subcutaneous) fat layer. The outcomes were noted 6 months after completion of the procedure.
However, we would like to emphasize the fact that cryolipolysis cannot replace a complete abdominoplasty when this is necessary. Furthermore, to date, we do not know the real risk of developing skin lesions (persistent hyperpigmentation or erythema) in the long term.
We must also emphasize that, in the case of an indication for abdominoplasty, this treatment should not be performed, since as plastic surgeons we know that abdominoplasty is considerably more difficult to perform after this type of treatment due to the extent of post-treatment fibrosis (Figure 5) [22].

Tissue sample (400× HE longitudinal micrograph) of a patient included in our study, who underwent abdominoplasty, one year after the second session of cryolipolysis (a, b). Fibrosis, amidst the adipose tissue, can be observed in red in the treated area, in contrast to the preserved surrounding tissue
The dedicated program of the CryoSlim, used for our study, named USER ASSIST tests at the beginning of each session the elasticity and the size of the fat to treat and then gives a percentage of expected success. According to the manufacturers of CryoSlim, their preliminary data indicate an elimination of 30–40% of treated fat per area. These data were confirmed by our results, which showed a fat layer reduction of 43.81% at 3 months and 41.73% at 6 months follow-up.
The difference between CryoSlim and other methods (such as high-intensity focused ultrasound—HIFU) is mainly due to the very low price of a session, the absence of necessary consumables and the totally pain-free effect during the session. In fact, one of the side effects of cold is the local anesthesia produced, so the main difference with HIFU is that patients undergoing a CryoSlim session do not complain of pain and experience no discomfort during the session.
Another advantage is the 'No Hand' treatment and also the fact that a CryoSlim treatment can be combined with other associated treatments immediately afterward.
Of course, the effectiveness of CryoSlim cannot be compared to that of liposuction, which is able to remove a much larger amount of fatty tissue, has the advantage of being able to treat several areas at the same time, and above all, in most cases, a single surgical procedure is sufficient to guarantee satisfactory results.
However, the promising results of this study should encourage further investigation. It would be interesting to determine whether the use of an interposed layer between the hand-piece and the skin, such as a transparent, adhesive polyurethane dressing (Opsite by Smith & Nephew, London, UK) could help reduce or avoid skin sequelae. It would also be interesting to determine the duration and stability of the results after a two-session treatment protocol. Also, the ideal temperatures for each body area should be studied in order to optimize the efficacy of the procedure without increasing the risks.
Conclusions
Cryolipolysis is an effective technique for treating abdominal localized fat deposits in selected patients. No major adverse events have been described for this procedure. Our promising results should encourage further studies to optimize the effectiveness of the procedure without a significant increase in risk.
Change history
12 August 2024
A Correction to this paper has been published: https://doi.org/10.1007/s00266-024-04292-8
29 August 2024
A Correction to this paper has been published: https://doi.org/10.1007/s00266-024-04321-6
References
Avram MM, Harry RS (2009) Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med 41:703–708
McLaughlin T, Lamendola C, Liu A, Abbasi F (2011) Preferential fat deposition in subcutaneous versus visceral depots is associated with insulin sensitivity. J Clin Endocrinol Metab 96:E1756-1760
Abraham TM, Pedley A, Massaro JM, Hoffmann U, Fox CS (2015) Association between visceral and subcutaneous adipose depots and incident cardiovascular disease risk factors. Circulation 132:1639–1647
Rosenquist KJ, Pedley A, Massaro JM et al (2013) Visceral and subcutaneous fat quality and cardiometabolic risk. JACC Cardiovasc Imaging 6:762–771
Bellini E, Grieco MP, Raposio E (2017) A journey through liposuction and liposculture: review. Ann Med Surg (Lond) 24:53–60
Mohammed BS, Cohen S, Reeds D, Young VL, Klein S (2008) Long-term effects of large-volume liposuction on metabolic risk factors for coronary heart disease. Obesity (Silver Spring) 16:2648–2651
Berry MG, Davies D (2011) Liposuction: a review of principles and techniques. J Plast Reconstr Aesthet Surg 64:985–992
Karow AM Jr, Webb WR (1965) Tissue freezing. A theory for injury and survival. Cryobiology 2:99–108
Beacham BE, Cooper PH, Buchanan CS, Weary PE (1980) Equestrian cold panniculitis in women. Arch Dermatol 116:1025–1027
Epstein EH Jr, Oren ME (1970) Popsicle panniculitis. N Engl J Med 282:966–967
Manstein D, Laubach H, Watanabe K, Farinelli W, Zurakowski D, Anderson RR (2008) Selective cryolysis: a novel method of non-invasive fat removal. Lasers Surg Med 40:595–604
Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J (2009) Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg 33:482–488
Kim J, Kim DH, Ryu HJ (2014) Clinical effectiveness of non-invasive selective cryolipolysis. J Cosmet Laser Ther 16:209–213
Ingargiola MJ, Motakef S, Chung MT, Vasconez HC, Sasaki GH (2015) Cryolipolysis for fat reduction and body contouring: safety and efficacy of current treatment paradigms. Plast Reconstr Surg 135:1581–1590
Garibyan L, Moradi Tuchayi S, Javorsky E et al (2020) Subcutaneous fat reduction with injected ice slurry. Plast Reconstr Surg 145:725e–733e
Juhasz M, Leproux A, Durkin A, Tromberg B, Mesinkovska NA (2020) Use of a novel, noninvasive imaging system to characterize metabolic changes in subcutaneous adipose tissue after cryolipolysis. Dermatol Surg 46:1461–1464
Adjadj L, SidAhmed-Mezi M, Mondoloni M, Meningaud JP, Hersant B (2017) Assessment of the efficacy of cryolipolysis on saddlebags: a prospective study of 53 patients. Plast Reconstr Surg 140:50–57
Langin D (2010) Recruitment of brown fat and conversion of white into brown adipocytes: strategies to fight the metabolic complications of obesity? Biochim Biophys Acta 1801(3):372–376
Choe SS, Huh JY, Hwang IJ, Kim JI, Kim JB (2016) Adipose tissue remodeling: its role in energy metabolism and metabolic disorders. Front Endocrinol (Lausanne). 13(7):30
Lipner SR (2018) Cryolipolysis for the treatment of submental fat: Review of the literature. J Cosmet Dermatol 17:145–151
Hwang IC, Kim KK, Lee KR (2020) Cryolipolysis-induced abdominal fat change: split-body trials. PLoS ONE 15:e0242782
Falster M, Schardong J, Santos DPD et al (2020) Effects of cryolipolysis on lower abdomen fat thickness of healthy women and patient satisfaction: a randomized controlled trial. Braz J Phys Ther 24:441–448
Bernstein EF, Bloom JD, Basilavecchio LD, Plugis JM (2014) Non-invasive fat reduction of the flanks using a new cryolipolysis applicator and overlapping, two-cycle treatments. Lasers Surg Med 46:731–735
Hamilton HK, Dover JS, Arndt KA (2014) Successful treatment of disfiguring hemosiderin-containing hyperpigmentation with the Q-switched 650-nm wavelength laser. JAMA Dermatol 150:1221–1222
Meyer PF, Davi Costa ESJ, Santos de Vasconcellos L, de Morais Carreiro E, Valentim da Silva RM (2018) Cryolipolysis: patient selection and special considerations. Clin Cosmet Investig Dermatol 11:499–503
Meningaud JP, SidAhmed-Mezi M, Billon R, Rem K, La Padula S, Hersant B (2019) Clinical benefit of using a multifractional Er:YAG laser combined with a spatially modulated ablative (SMA) module for the treatment of striae distensae: a prospective pilot study in 20 patients. Lasers Surg Med 51(3):230–238
Hersant B, La Padula S, SidAhmed-Mezi M, Rodriguez AM, Meningaud JP (2017) Use of platelet-rich plasma (PRP) in microsurgery. J Stomatol, Oral Maxillofac Surg 118(4):236–237
La Padula S, Hersant B, Bompy L, Meningaud JP (2019) In search of a universal and objective method to assess facial aging: The new face objective photo-numerical assessment scale. J Craniomaxillofac Surg 47(8):1209–1215
Ruiz R, Hersant B, La Padula S, Meningaud JP (2018) Facelifts: Improving the long-term outcomes of lower face and neck rejuvenation surgery: The lower face and neck rejuvenation combined method. J Craniomaxillofac Surg 46(4):697–704
La Padula S, Hersant B, Meningaud JP (2018) Intraoperative use of indocyanine green angiography for selecting the more reliable perforator of the anterolateral thigh flap: a comparison study. Microsurgery 38(7):738–744. https://doi.org/10.1002/micr.30326
La Padula S, Hersant B, Pizza C, Chesné C, Jamin A, Ben Mosbah I, Errico C, DAndrea F, Rega U, Persichetti P, Meningaud JP (2021) Striae distensae: in vitro study and assessment of combined treatment with sodium ascorbate and platelet-rich plasma on fibroblasts. Aesthet Plast Surg 45(3):1282–1293
La Padula S, Hersant B, Chatel H, Aguilar P, Bosc R, Roccaro G, Ruiz R, Meningaud JP (2019) One-step facial feminization surgery: the importance of a custom-made preoperative planning and patient satisfaction assessment. J Plast Reconstr Aesthet Surg 72(10):1694–1699
Hersant B, SidAhmed-Mezi M, La Padula S, Niddam J, Bouhassira J, Meningaud JP (2016) Efficacy of autologous platelet-rich plasma glue in weight loss sequelae surgery and breast reduction: a prospective study. Plast Reconstr Surg Glob Open 4(11):e871
Hersant B, SidAhmed-Mezi M, Aboud C, Niddam J, Levy S, Mernier T, LaPadula S, Meningaud JP (2021) Synergistic effects of autologous platelet-rich plasma and hyaluronic acid injections on facial skin rejuvenation. Aesthet Surg J 41(7):NP854–NP865
La Padula S, Hersant B, Noel W, Niddam J, Hermeziu O, Bouhassira J, Bosc R, Meningaud JP (2016) Use of the retrograde limb of the internal mammary vein to avoid venous congestion in DIEP flap breast reconstruction: Further evidences of a reliable and timesparing procedure. Microsurgery 36(6):447–452
Hersant B, Werkoff G, Sawan D, Sidahmed-Mezi M, Bosc R, La Padula S, Kalsoum S, Ouidir N, Meningaud JP, Belkacemi Y (2020) Carbon dioxide laser treatment for vulvovaginal atrophy in women treated for breast cancer: Preliminary results of the feasibility EPIONE trial. Ann Chir Plast Esthet 65(4):e23–e31. https://doi.org/10.1016/j.anplas.2020.05.002. (Epub 2020 Jun 5)
La Padula S, Hersant B, Helynck P, Mezi SidAhmed M, Meningaud JP (2020) Proposal of a noninvasive method to reduce injection-related bruising in aesthetic medicine: transillumination. Aesthet Plast Surg 44(2):530–534. https://doi.org/10.1007/s00266-019-01447-w
Giroux PA, Hersant B, SidAhmed-Mezi M, Pizza C, La Padula S, Meningaud JP (2019) The outcomes assessment of the plasma blade technology in upper blepharoplasties: a prospective study on a series of 25 patients. Aesthet Plast Surg 43(4):948–955. https://doi.org/10.1007/s00266-019-01360-2. (Epub 2019 Mar 29)
La Padula S, Hersant B, Meningaud JP, D’Andrea F (2018) Use of autologous fat graft and fractiononal co2 laser to optimize the aesthetic and functional results in patients with severe burn outcomes of the face. J Stomatol Oral Maxillofac Surg. 119(4):279–283
Hersant B, Jabbour S, Noel W, Benadiba L, La Padula S, SidAhmed-Mezi M, Meningaud JP (2018) Labia majora augmentation combined with minimal labia minora resection: a safe and global approach to the external female genitalia. Ann Plast Surg 80(4):323–327
Hersant B, Niddam J, Picard F, Bouhassira J, La Padula S, Bosc R, Meningaud JP (2016) Platelet-rich plasma with basic fibroblast growth factor for treatment of wrinkles and depressed areas of the skin. Plast Reconstr Surg 137(6):1048–1049
Eyraud Q, La Padula S, Pizza C, Hersant B, Meningaud JP (2021) Carboxytherapy, subcutaneous injections of carbon dioxide in the management of infraorbital dark circles: a reliable and effective procedure. J Craniomaxillofac Surg 49(8):670–674. https://doi.org/10.1016/j.jcms.2021.01.028. (Epub 2021 Feb 5 PMID: 33612408)
Azuelos A, SidAhmed-Mezi M, La Padula S, Aboud C, Meningaud JP, Hersant B (2019) High-intensity focused ultrasound: a satisfactory noninvasive procedure for neck rejuvenation. Aesthet Surg J 39(8):NP343–NP351. https://doi.org/10.1093/asj/sjz093. (PMID: 30923813)
La Padula S, Hersant B, Noel W, Meningaud JP (2018) Liposuction-assisted four pedicle-based breast reduction (LAFPBR): a new safer technique of breast reduction for elderly patients. J Plast Reconstr Aesthet Surg 71(5):691–698. https://doi.org/10.1016/j.bjps.2018.01.006. (Epub 2018 Jan 31 PMID: 29433957)
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to disclose
Ethical Approval
Not required.
Human Participants
All procedures in the study involving human participants have been performed in accordance with the ethical standards of institutional and/or national research committees and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
All patients taking part in the study signed a written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Coiante, E., Pensato, R., Hadji, I. et al. Assessment of the Efficacy of Cryolipolysis on Abdominal Fat Deposits: A Prospective Study. Aesth Plast Surg 47, 2679–2686 (2023). https://doi.org/10.1007/s00266-023-03369-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-023-03369-0