
Abstract
Background
This study was performed to identify a safe method for filler injection to prevent blood vessel damage, by means of checking the location and depth of the blood vessels on the midline of the nose using Doppler ultrasonographic imaging.
Methods
Ultrasonographic images of the nasal areas of patients for filler injection rhinoplasty were reviewed. The location and depth of the dorsal nasal arteries and the intercanthal vein in each part on the midline of the nose were checked.
Results
The intercanthal vein was detected in the midline of the radix in 22 patients and the midline of the rhinion region in two patients. There were no patients in whom the intercanthal vein was observed in the midline of the supratip region. The dorsal nasal artery was detected in the rhinion region in six patients and in the supratip region in two patients. There were no patients in whom the dorsal nasal artery was observed in the midline of the radix. The dorsal nasal artery was located within 1.2 mm from the perichondrium or periosteum in three patients in whom it was detected in the rhinion.
Conclusions
When performing dorsal augmentation, the injection of filler into the preperiosteal layer in the rhinion region should be avoided for the prevention of vascular embolism. During dorsal augmentation in patients with a nasal hump, the filler can be injected into the preperiosteal space in the radix by introducing a needle perpendicular to the periosteum from the skin.
Level of Evidence V
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rhinoplasty is one of the most commonly performed operations in the field of cosmetic surgery in Asia, because Asians generally have a flat nasal bridge and underprojected nasal tip. However, rhinoplasty using implants and autologous grafts involves a long recovery time, is expensive, and is associated with morbidity and many complications. Therefore, many patients hesitate to undergo this surgery; they would prefer a simpler and cheaper procedure with fewer side effects and a shorter recovery period [1]. Rhinoplasty using filler is a procedure that meets these demands [2].
Filler injection into the nose is performed by either dorsal injection or nasal tip injection. The nasal dorsum is supported by relatively solid and firm structures, such as the nasal bone and upper lateral cartilage; thus, it is easier to shape the nose with filler injection [3, 4]. Nasal dorsum augmentation with filler is performed by direct injection perpendicular to the skin using a sharp needle; alternatively, it is performed by indirect injection entering from both the glabella and the infratip region, using a long blunt cannula to create a straight dorsum [5].
Direct sharp needle injection typically requires multiple injections to cover the length of the nasal dorsum; the filler is placed more precisely with minimal shape distortion or deviation. Blunt cannula injection requires greater skill and experience to palpate the position of the cannula tip and estimate the amount of filler that has been injected into the target area. Although excellent results persuade patients to seek regular filler treatment, some minor complications usually occur (e.g., erythema, swelling, and ecchymosis). Although these complications are generally acceptable to patients, two rare serious complications of injection rhinoplasty may occur: blindness and skin infraction [6,7,8,9]. Moreover, nasal augmentation using soft tissue filler, which can damage the dorsal nasal artery, can cause serious ocular complications (e.g., blindness) [10].
The major blood vessels of the external nose lie in the superficial muscular aponeurotic system or superficial fatty layers [11]. To minimize vascular injuries, placement of deeply into the preperiosteal layer of the nasal bone and preperichondrial layer of the upper lateral cartilage in the midline is therefore recommended, using both the sharp needle and blunt cannula methods [5, 12, 13]. This study was performed to identify a safe injection method to prevent blood vessel damage during filler injection, by means of checking the location and depth of the blood vessels on the midline of the nose using Doppler ultrasonographic imaging, at the point where the filler is injected for nasal dorsum augmentation.
Materials and Methods
The Institutional Review Board of our institute (KC20REDI0126) approved this study, which was conducted in accordance with the Declaration of Helsinki. Our institute waived informed consent for this retrospective study. Ultrasonographic images of the nasal areas of patients who visited our clinic for filler injection rhinoplasty between January 1, 2019, and June 31, 2019, were reviewed in this study. The results in patients with severe humps in whom ultrasonography was difficult were excluded from the analysis. In addition, patients who had undergone previous nose filler injection or rhinoplasty using implants and autologous grafts were excluded, because accurate measurements could not be obtained in such patients. The initial study population consisted of 43 patients. Four patients with a severe hump and five patients with prior nasal filler injection were excluded. Therefore, a total of 34 patients were included in this study.
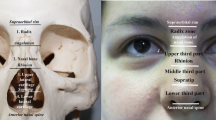
The nasal dorsum was divided into the radix, the rhinion, and the supratip region; ultrasonography was performed at each of the three sites. A hockey stick probe was used to evaluate the course and location of the dorsal nasal artery in each patient. The radix was defined as the point where the nasal bone meets the upper nasal cartilage, 5 mm in width caudally and cephalically. The rhinion was defined as the area between the line connecting both medial ends of the eyelids and the cephalic end of the radix; the supratip region was set at 1 cm from the caudal end of the radix.
On the radix, the midpoint of the probe was positioned at the point where the midline of the nose and the intercanthal line met; ultrasound examination was performed transversely along the intercanthal line and at right angles to the intercanthal line. On the rhinion, the midpoint of the probe was positioned at the point where the nasal bone and upper lateral cartilage met at the midline of the nose; ultrasound examination was then performed in the horizontal direction on the facial plane, as well as perpendicular to the facial plane. On the supratip region, the midpoint of the probe was positioned at a point 1 cm caudally from the nasal bone and the point where the upper lateral cartilage meets the midline of the nose; ultrasound examination was then performed in the horizontal direction on the facial plane, as well as perpendicular to the facial plane.
The intercanthal vein and dorsal nasal artery are mostly observed in the dorsal midline of the nose. The presence of the intercanthal vein and dorsal nasal artery was investigated in each region. The number of patients in whom blood vessels were located within 1.2 mm from the periosteum was counted because the bevel of the needle used to inject the filler into the nose is 1.2 mm. This study was approved by the institutional review board of our institution and was performed in accordance with the tenets of the Declaration of Helsinki.
Results
The 34 patients consisted of 27 women and seven men, with a mean age of 32.6 years. No intercanthal vein was found on the midline of the nose in 10 patients (29.4%). The intercanthal vein was detected on the midline of the radix in 22 patients (64.7%) and in the midline of the rhinion in two patients (5.9%). There were no patients in whom the intercanthal vein was observed in the midline of the supratip region (Fig. 1).

Among the total of 34 patients, no intercanthal vein was found on the midline of the nose in 10 patients (29.4%). The intercanthal vein was detected on the midline of the radix in 22 patients (64.7%) and on the midline of the rhinion region in two patients (5.9%). The dorsal nasal artery was found in the rhinion region in six patients (17.7%) and in the supratip region in two patients (5.9%). However, there were no patients in whom the dorsal nasal artery was found in the midline of the radix
The dorsal nasal artery was found in the rhinion in six patients (17.7%) (Fig. 2) and in the supratip region in two patients (5.9%); there were no patients in whom the dorsal nasal artery was found in the midline of the radix (Fig. 1). In three patients (8.8%) with the dorsal nasal artery in the rhinion region, it was located within 1.2 mm from the perichondrium or periosteum (Fig. 3).

The dorsal nasal artery was found in the subcutaneous layer of the rhinion region

In the rhinion, the dorsal nasal artery was found 1.2 mm from the perichondrium or periosteum
Discussion
Because injection rhinoplasty using fillers is increasingly common, the incidences of related side effects, such as skin necrosis and blindness due to vascular compromise, are also increasing. To avoid these adverse effects, physicians should be aware of the relevant vascular anatomy of the nose and injectable anatomical layers.
Previous studies have shown that the dorsal nasal artery may be responsible for the transmission of emboli after filler injection into the root of the nose, which can result in vision changes and skin necrosis [14,15,16]. Injection of filler into the dorsal nasal artery can lead to blindness and cerebral infarction, as well as skin necrosis. Danesh‐Meyer et al. reported temporary neurological and permanent vision problems after the injection of filler into the nose. Filling materials injected into the dorsal nasal artery can travel retrogradely into the ophthalmic and internal carotid arteries; they can then migrate distally into the middle cerebral, central retinal, and posterior ciliary arteries [17]. Park et al. reported vision complications after injection of autologous fat into the nasolabial fold. They also considered the dorsal nasal artery to be the main cause of this problem, because injection of foreign materials into the dorsal nasal artery may occlude the short posterior ciliary artery from the ophthalmic artery [18].
Many studies have shown that nasal major blood vessels, including the dorsal nasal artery, are located in the fibromuscular or subcutaneous fat layers. Therefore, the deep fatty layer located between the fibromuscular layer and the periosteum or perichondrium is considered a safe layer for nose filler injection. However, Tansatit et al. demonstrated that bilateral dorsal nasal arteries existed in only 34% of the cadaveric specimens in their study, while 28% had only a single, large dorsal nasal artery. Moreover, in 14% of their specimens, the dorsal nasal artery crossed the midline in the middle third of the nose. Their findings demonstrated that injection perpendicular to the midline would puncture the artery in patients where the artery travels across the midline [19].
Choi et al. showed that the medial branch of the dorsal nasal artery was located near the midline in patients who exhibited an artery with two branches, corresponding to 34.1% of patients in that study. In addition, 82.4% of the patients in that study exhibited a communicating branch, which connected the bilateral dorsal nasal arteries, in the nasal dorsum [20]. In an investigation using Doppler ultrasonography, Lee et al. demonstrated that the dorsal nasal artery was present at the midline of the nose in 10 patients (20%). In four patients (8%), the artery traveled immediately beneath the preperiosteal layer, which is underneath the nasalis muscle. The diameter of the dorsal nasal artery was approximately 1.2 mm (range, 1.0–2.0 mm) [21]. Therefore, during the injection of filler into the nose, there is a high probability of encountering the dorsal nasal artery in the midline of the nose.
Because the dorsal nasal artery is located in the fibromuscular or subcutaneous layers, the deep fatty layer in the periosteum is considered a safe site for injection of filler into the nose. Two methods are available for injection of filler into the preperiosteal layer: (1) insertion of a sharp needle into the nasal dorsum at right angles from the skin on the midline of the nose, and (2) injection into the deep fatty layer using a long, blunt cannula. For injection from the midline of the nose using a needle, a 27–30-gauge (G) needle is often used. Many physicians prefer to perform the injection with the needle at a right angle to the skin, while using the tip of the needle to detect hard bone or cartilage. This method may be safe, but can cause bleeding if there is a blood vessel in the path through which the needle passes; it can cause vascular embolism if there is a blood vessel in the deep fatty layer. Regular needles have a beveled tip. For a 27G needle, this bevel is 1.2 mm long. Therefore, when the needle is inserted at right angles and injected into the periosteum, the filler can be injected into the blood vessel (through the bevel of the needle) if the blood vessel is located within 1.2 mm from the periosteum. In this study, there were three patients in whom the dorsal nasal artery was located 1.2 mm above the periosteum on the midline of the nose in such patients, there is a possibility of a vascular embolism when the filler is injected into the periosteum in a direction perpendicular to the skin on the midline of the nose. Alternatively, a long, blunt cannula can be used to inject filler into the nose. The use of a blunt cannula can improve patient comfort and alter the injection technique [22]. In addition, the use of a blunt cannula simplifies filler injection and results in less bruising and pain, with more rapid recovery [23].
The cannula is usually inserted through a single puncture site. Usually caudocranially approaches from the infralobular region, and the puncture is performed between the nostril. The cannula can be safely positioned in the deep fatty layer by gliding along the bottom of the nasal dorsum, while searching for hard cartilage or bone at its tip. Injection is performed retrogradely to minimize pressure at the cannula tip, while simultaneously controlling the effect of the filler for volumization.
This is a safe procedure, but requires considerable experience to achieve proficiency. In particular, if a hump is present, the cannula moves from the deep fatty layer to the subcutaneous layer while advancing beyond the hump; in patients with abundant subcutaneous tissue at the tip of the nose, it may be difficult to locate the cannula on the cartilage, and the cannula may move forward along the subcutaneous layer. The most important consideration in this procedure is the selection of the appropriate cannula diameter. A previous study found that the diameter of the dorsal nasal artery was 1 mm [24]. Another study using Doppler ultrasound reported that the diameter of the dorsal nasal artery was approximately 1.2 mm (range, 1.0–2.0 mm) [21]. Moreover, a recent cadaveric study reported that a cannula < 27G is similar to a needle in terms of penetration ability; notably, a 20G cannula can penetrate the walls of the superficial temporal and facial arteries [25]. Theoretically, a cannula with a diameter ≥ 19.5G can be considered relatively safe because it may not cannulate the lumen of the dorsal nasal artery.
When performing filler dorsal augmentation for patients with a hump, it is difficult to retain the cannula tip in the preperiosteal layer; when the cannula is advanced beyond the hump, its cannula tip can easily be positioned in the subcutaneous layer. Therefore, when traveling from the infralobular direction to the glabellar direction, the cannula should be advanced until immediately prior to the hump. The location above the hump (i.e., the radix) can receive an injection into the preperiosteal layer using a sharp needle to pierce the skin in a manner perpendicular to the nasal bone. In the present study, no blood vessels were observed in the space 1.2 mm above the periosteum in the radix. However, care is needed because the intercanthal vein may be encountered during the advancement of the needle from the skin to the periosteum. In addition, the filler can be injected into the upper part of the hump by using a cannula, instead of a needle. In this instance, the puncture is performed between the eyebrows; then the cannula is then advanced to the hump.
However, most of the above studies have been described based on anatomical studies of Asian races. In general, Western people have thinner skin with the richness of sebaceous and sweat glands than Asians. It may be more difficult to perform filler rhinoplasty on patients with thick, oily skin because they may experience severe post-procedure edema more often, and creating a pleasing 3-D shape is challenging. On the other hand, in such patients, minute irregularities or asymmetry is camouflaged more easily compared with patients with thin skin [3]. Therefore, the actual filler rhinoplasty should be conducted in consideration of ethnic variability.
Finally, physicians should have a good understanding of the physical properties of the filler material. When the preperiosteal deep fatty layer is the target layer for filler injection—this layer is compressed by the fibromuscular layer, subcutaneous layer, and skin—a filler with high lifting capacity is needed to maintain the shape of the nose after filler injection into the deep fatty layer. This is especially relevant for Asians, who require sufficient raising of the height of the nose. The Elastic modulus (G′) is a measure of the elastic behavior of the filler gel (i.e., its ability to recover its shape after shear deformation) [26]. If G′ is high, it is considered suitable for deep tissue lifting. The results of the rheological evaluation of a series of fillers, which are frequently considered in nasal dorsum augmentation in Korea, were compared in a previous study [27].
The limitation of this article is that since this study population consists only of Asians, the anatomical variability between races was not generally considered. Also, there is a limitation in not being able to confirm the layer where blood vessels are located by dissecting the cadaver after ultrasound is performed on the cadaver.
Conclusion
After the filler injection for nose augmentation vascular compromise had been reported in many cases. Especially during dorsal augmentation with filler, the dorsal nasal artery may be located close to (i.e., within 1.2 mm) the periosteum in the rhinion region. Therefore, the needle tip bevel may enter the blood vessels, allowing the injection of filler into the vasculature. To prevent vascular embolism, injection of filler using a sharp needle on the nasal midline into the preperiosteal layer in the rhinion region should be avoided. When performing dorsal augmentation in patients with nasal humps, the filler can be injected into rhinion and supratip region by using a blunt cannula, while injection can be performed into the preperiosteal space in the radix by introducing a needle perpendicular to the periosteum from the skin.
Change history
11 June 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00266-021-02408-y
References
Constantinidis J, Daniilidis J (2005) Aesthetic and functional rhinoplasty. Hosp Med 66:221–226
Murray CA, Zloty D, Warshawski L (2005) The evolution of soft tissue fillers in clinical practice. Dermatol Clin 23:343–363
Moon HJ (2016) Use of fillers in rhinoplasty. Clin Plast Surg 43:307–317
Moon HJ (2018) Injection rhinoplasty using filler. Facial Plast Surg Clin North Am 26:323–330
Han X, Hu J, Cheng L, Li F (2015) Multiplane hyaluronic acid (EME) in female Chinese rhinoplasty using blunt and sharp needle technique. J Plast Reconstr Aesthet Surg 68:1504–1509
DeLorenzi C (2013) Complications of injectable fillers, part I. Aesthet Surg J 33:561–575
Funt D, Pavicic T (2013) Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol 6:295–316
Humphrey CD, Arkins JP, Dayan SH (2009) Soft tissue fillers in the nose. Aesthet Surg J 29:477–484
Kim SN, Byun DS, Park JH, Han SW, Baik JS, Kim JY, Park JH (2014) Panophthalmoplegia and vision loss after cosmetic nasal dorsum injection. J Clin Neurosci 21:678–680
Beleznay K, Carruthers JD, Humphrey S, Jones D (2015) Avoiding and treating blindness from fillers: a review of the World Literature. Dermatol Surg 41:1097–1117
Jung DH, Kim HJ, Koh KS, Oh CS, Kim KS, Yoon JH, Chung IH (2000) Arterial supply of the nasal tip in Asians. Laryngoscope 110:308–311
Baptista C, Nguyen PS, Desouches C, Magalon G, Bardot J, Casanova D (2013) Correction of sequelae of rhinoplasty by lipofilling. J Plast Reconstr Aesthet Surg 66:805–811
Schuster B (2015) Injection rhinoplasty with hyaluronic acid and calcium hydroxyapatite: a retrospective survey investigating outcome and complication rates. Facial Plast Surg 31:301–307
Kim YJ, Kim SS, Song WK, Lee SY, Yoon JS (2011) Ocular ischemia with hypotony after injection of hyaluronic acid gel. Ophthal Plast Reconstr Surg 27:e152-155
Kubota T, Hirose H (2005) Permanent loss of vision following cosmetic rhinoplastic surgery. Jpn J Ophthalmol 49:535–536
Lazzeri D, Agostini T, Figus M, Nardi M, Pantaloni M, Lazzeri S (2012) Blindness following cosmetic injections of the face. Plast Reconstr Surg 129:995–1012
Danesh-Meyer HV, Savino PJ, Sergott RC (2001) Case reports and small case series: ocular and cerebral ischemia following facial injection of autologous fat. Arch Ophthalmol 119:777–778
Park SH, Sun HJ, Choi KS (2008) Sudden unilateral visual loss after autologous fat injection into the nasolabial fold. Clin Ophthalmol 2:679–683
Tansatit T, Moon HJ, Rungsawang C, Jitaree B, Uruwan S, Apinuntrum P, Phetudom T (2016) Safe planes for injection rhinoplasty: a histological analysis of midline longitudinal sections of the Asian nose. Aesthetic Plast Surg 40:236–244
Choi DY, Bae JH, Youn KH, Kim W, Suwanchinda A, Tanvaa T, Kim HJ (2018) Topography of the dorsal nasal artery and its clinical implications for augmentation of the dorsum of the nose. J Cosmet Dermatol 17:637–642
Lee W, Kim JS, Oh W, Koh IS, Yang EJ (2019) Nasal dorsum augmentation using soft tissue filler injection. J Cosmet Dermatol
Zeichner JA, Cohen JL (2012) Use of blunt tipped cannulas for soft tissue fillers. J Drugs Dermatol 11:70–72
Fulton J, Caperton C, Weinkle S, Dewandre L (2012) Filler injections with the blunt-tip microcannula. J Drugs Dermatol 11:1098–1103
Kleintjes WG (2007) Forehead anatomy: arterial variations and venous link of the midline forehead flap. J Plast Reconstr Aesthet Surg 60:593–606
Pavicic T, Webb KL, Frank K, Gotkin RH, Tamura B, Cotofana S (2019) Arterial wall penetration fForces in needles versus cannulas. Plast Reconstr Surg 143:504e–512e
Pierre S, Liew S, Bernardin A (2015) Basics of dermal filler rheology. Dermatol Surg 41(Suppl 1):S120-126
Lee W, Hwang SG, Oh W, Kim CY, Lee JL, Yang EJ (2020) Practical guidelines for hyaluronic acid soft-tissue filler use in facial rejuvenation. Dermatol Surg 46:41–49
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to disclose.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Moon, HJ., Lee, W., Do Kim, H. et al. Doppler Ultrasonographic Anatomy of the Midline Nasal Dorsum. Aesth Plast Surg 45, 1178–1183 (2021). https://doi.org/10.1007/s00266-020-02025-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-020-02025-1