
Abstract
Background
The recent rise in popularity of minimally invasive facial aesthetic procedures has resulted in the overall heightened patient interest in lip rejuvenation. There is a variety of techniques and modifications for surgical upper lip enhancement described in the literature but no single method is considered optimal. The aim of this literature review is to provide a comprehensive analysis of the studies dealing with surgical upper lip enhancement and evaluate their short- and long-term outcomes, as well as complication profiles.
Methods
A comprehensive review of the published literature through July of 2019 was performed. The PUBMED and Cochrane databases were searched for all English language articles on aesthetic surgical enhancement of the upper lip. Only articles dealing with the aesthetic aspect of the upper lip subunit were included. Preoperative assessment, patient selection and technique execution were assessed. Data were abstracted on all postoperative complications and outcomes.
Results
Overall, 52 articles were screened for inclusion, of which 17 met the inclusion criteria. The total number of patients treated in these studies was 2265. The average follow-up period was 30 months. The most commonly used surgical method across the studies was the subnasal lip lift (93.6%). The bull’s horn excision pattern was utilized to perform the subnasal lip lift in 71.7% of the cases, and the wavy ellipse excision was used in 18.1% of patients. Lip advancement by vermillion border excision pattern was the technique of choice for 49 patients (2.2%). Across all patients the most common complication was a non-aesthetically appealing result or adverse scarring with a mean incidence of 7.23%. Overall, the studies reported improvement in the aesthetic appearance of the upper lip after surgical enhancement, along with few but promising reports of high patient satisfaction. There is a relative paucity of high-quality data regarding complication profiles, patient selection, indications and contraindications.
Conclusions
This review provides an overview of several techniques and modifications for upper lip enhancement. It highlights the paucity of high-quality data on their application and optimizing patient selection. Promising satisfaction rates and relatively low complication rates suggest a more prominent role for surgical cheiloplasty in facial rejuvenation.
Level of evidence III
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The recent rise in popularity of soft tissue fillers and other minimally invasive facial aesthetic procedures has resulted in the overall heightened patient interest in lip rejuvenation [1,2,3]. Currently, minimally invasive treatment modalities are the overwhelming treatment of choice for upper lip rejuvenation. However, the limitations of these modalities are well known. Product resorption and a short-lived effect are major concerns as they lead to a need for multiple treatments and escalating costs over time. In the context of these concerns it is thus pertinent to revisit the role of surgical upper lip rejuvenation and enhancement.
Techniques in aesthetic surgical upper lip enhancement, also known as cheiloplasty, have traditionally focused on addressing the effects of aging and restoring youthful appearance [3]. However, the role of cosmetic lip enhancement has broadened. Patients of all ages now request upper lip interventions to obtain a desired look for aesthetic, physiognomic and cultural purposes, or as part of gender confirmation surgery [4, 5]. Surgical upper lip enhancement, performed in isolation or concomitantly with other facial aesthetic procedures, provides superior versatility compared to minimally invasive treatments in order to meet the demands of modern facial aesthetics and the aforementioned patient goals.
There is a variety of excisional techniques and modifications for surgical upper lip enhancement described in the literature but no single method is considered optimal. Given the anatomic and functional complexity of the upper lip subunit and the central face, the clinical indications, contraindications and complication profiles of these techniques warrant examination. The aim of this literature review is to provide a comprehensive analysis of the studies dealing with surgical upper lip enhancement and evaluate their short- and long-term outcomes, as well as complication profiles.
History
Upper lip soft tissue lengthening is a prominent event that occurs with aging in both men and women, and surgeons focused on upper lip lift techniques since the early 1970s. Fundamentally, the two main approaches described originally were the subnasal lip lift and the vermilion border lip advancement. In the subnasal lip lift technique the skin incision is made at or just inferior to the alar base, nasal sills and columellar footplates to achieve a direct vertical lift (Figs. 1 and 2). The lip advancement techniques place the incision along the vermillion border to achieve a more radial vector of lift (Fig. 3). These methods formed the foundation for most of the advancements and modifications that followed, including placement of incisions within the nasal sill and nostrils, suspension techniques, and orbicularis oris muscle plication or excision. Most recently, the adjunctive use of fat grafting has constituted a significant advancement [9].

adapted from Lee et al. [4]
Subnasal lift. Bull’s horn excision;

adapted from Austin [6]
Subnasal lift. a Tradition wavy excision. b Wavy ellipse excision with vertical extension;

The subnasal upper lip lift was first described by Cardosa and Sperli in 1971, and the first large series was published by Rozner and Isaacs, mainly as an adjunct to facelift, in 1981 [10, 11]. They reported good outcomes with excision of the subnasal skin to shorten the upper lip and vertically lift the entire upper lip subunit. Several modifications of the subnasal lift approach were subsequently published, the most popular of which being Austin’s wavy ellipse technique [6]. Austin’s 83-patient case series was published in 1986 and demonstrated very satisfactory results in terms of hiding the final incision within the caudal nasal border via a wavy ellipse form of upper lip skin excision [6]. The bull’s horn pattern of excision was a direct modification of Austin’s wavy ellipse [1, 9, 12].
Fanous presented the first case series consisting of 32 cases of vermillion advancement in 1983 [7]. Austin utilized this novel technique soon after, only to eventually abandon it in favor of the subnasal lift technique. This approach never truly gained considerable popularity due to visible scarring at the vermillion border and disruption of the white roll [8, 13].
There is a relative paucity of literature reports during the 1990s. However, in the past twenty years there has been a gradual increase in the popularity of surgical upper lip enhancement, which coincided with the emergence of numerous new techniques and modifications [4, 14, 15]. Modifications included Jung et al.’s [16] (short scar) technique sparing the columella, philtral columns and groove (Fig. 4), and the orbicularis oris muscle plication or excision (Fig. 5) [17].

adapted from Jung et al. [16]
Subnasal lift sparing the columella, philtral columns and groove (short scar). Two subnasal incisions are made, extending into the nostril and allowing a wide field of dissection for tissue movement;

adapted from Pan [17]
Subnasal bull’s horn excision with T-shaped muscle resection;
The most recent major advancement was the introduction of the endonasal suspension suture technique, first described by Echo et al. in 2011 [18]. The technique, also called the “no scar lip lift”, consists of small, hidden endonasal incisions allowing for a suspension suture incorporating the orbicularis oris muscle and fascia to transfix the upper lip to the anterior nasal spine or the septal cartilage (Fig. 6). The suspension suture technique can be combined with traditional forms of subnasal lift [12, 19].

adapted from Echo et al. [18]
Endonasal suspension lift;
Methods and Materials
A comprehensive review of the published literature through July of 2019 was performed. The PUBMED and Cochrane databases were searched for all English language articles on aesthetic surgical enhancement of the upper lip. Search terms used were “Lip”, “Upper Lip Subunit”, “Lip Aging”, “Lip Surgery”, “Upper Lip Lift”, “Upper Lip Enhancement”, and “Upper Lip Augmentation”. The search strategy also included procedure related MeSH terms: “Upper Lip Lift” and “Surgical Enhancement of the Upper Lip”.
Articles that met the inclusion criteria were case studies, case series and retrospective data review studies on techniques specific to the upper lip. Articles that focused on the placement of implants or grafts, autologous or otherwise, were not included. Also excluded were articles on surgical techniques aiming solely on providing lip augmentation. Dental and orthognathic studies were excluded, as were articles discussing congenital lip malformations or reconstructive procedures. Studies that did not provide adequate descriptions or details of the technique employed were excluded.
Selected articles were carefully assessed for content and data related to the surgical technique of aesthetic upper lip enhancement. The techniques were categorized and grouped for the purpose of this review according to the authors’ descriptions, schematics and photographs. Preoperative assessment, patient selection and technique execution were assessed. Data were abstracted on all postoperative complications and outcomes. Each selected article’s reference listing was examined to identify additional articles, which were further similarly assessed for content.
Results
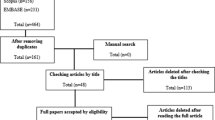
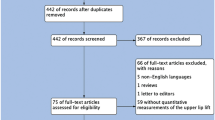
Overall, 52 articles were screened for inclusion, of which 17 met the inclusion criteria (Fig. 7). The total number of patients treated in these studies was 2265 (Table 1). The average follow-up period was 30 months (range of 2–120 months). Evaluation of the demographic characteristics revealed that the majority of the patients were female (88.3%), and male patients comprised 11.7% of the cohort. The mean age of the patients was 45 year (range 30–81 years). The studies did not provide sufficient data on patient ethnicity.

Overview of the article selection process
The most commonly used surgical method across the studies was the subnasal lip lift (93.6%). The bull’s horn excision pattern was utilized to perform the subnasal lip lift in 71.7% of the cases, and the wavy ellipse excision was used in 18.1% of patients. The short scar technique was utilized in 4.0% of patients. Combination of wavy ellipse excision and endonasal flap was performed in 311 patients (13.7%). Synchronous orbicularis oris muscle resection took place in 84 patients (3.7%). Combination of endonasal fascial suspension and subnasal bull’s horn excision was performed in 823 patients (36.3%). Endonasal fascial suspension without skin excision took place in 92 patients (4.1%). Lip advancement by vermillion border excision pattern was the technique of choice for 49 patients (2.2%). A total of 500 patients underwent micro-fat grafting in combination with skin excision although this data were collected from the one study that reported concomitant use of fat grafting. A summary of all the surgical techniques is provided in Table 2.
The outcomes and complications are presented in Table 3. Across all patients the most common complication was a non-aesthetically appealing result or adverse scarring with a mean incidence of 7.23% and a range from 3.2 to 10.5%. When comparing complications by techniques lip asymmetry and alar distortion occurred in highest incidence following endonasal flaps (12.2%) and lip advancement (6.3%) procedures. Wound infection and dehiscence were reported in less than or equal to 2.8% of cases among all procedures. Orbicularis oris resection was associated with nostril show, philtrum scarring and animation deformity at rates of 4%, 1.3% and 1.3%, respectively, in the one study describing this technique in combination with bull’s horn subnasal lift. Revision rates were found to be under-reported and further conclusions could not be made.
There is a relative paucity of data with regards to patient satisfaction. Three studies reported patient satisfaction rates, which represented 14% of the cohort. Following bull’s horn excision, patients stated being ‘satisfied’ or ‘very satisfied’ at a 92.1% rate. High satisfaction rates approached 100% when the short scar excision technique was utilized but were lower in patients who had undergone orbicularis oris resection (74.0%).
Discussion
The surgical techniques of aesthetic upper lip enhancement have evolved significantly over the years. Overall, the included studies reported improvement in the aesthetic appearance of the upper lip after surgical enhancement, along with few but promising reports of high patient satisfaction. However, it is apparent there is a relative paucity of high-quality data regarding complication profiles. Analyses on patient selection, indications and contraindications with regard to each technique are lacking.
Relying solely on the classical facial ratios is not sufficient for planning surgical lip enhancement, as there are numerous variables to consider in modern upper cheiloplasty [22, 23]. In order to optimize patient and technique selection, an individualized approach incorporating the patient’s anatomy and features, previous or concomitant facial procedures, as well as the aesthetic goal is necessary. In addition, one technique cannot fit all patients, therefore detailed knowledge of the intricacies and execution of these techniques and their application is of utmost importance. Careful technique selection and application is especially important in younger male and female patients, as well as in surgery for facial feminization as the desired aesthetic outcomes may be particularly variable [5, 24, 25].
The applicability of the various techniques in addressing ethnic and other anatomic variations among patients, such as the nasal base to upper lip width ratio, is not clearly described in the literature. Similarly, there is little data on the long-term effect of these techniques on upper lip projection and the correction of vermilion thinning. From an anatomic perspective, the treatment effect of the majority of the techniques remains empiric. Despite the inconsistency and scarcity of reports, it appears the addition of technical variables such as orbicularis oris resection, suspension and endonasal flaps is associated with inferior outcomes. As their indications are not clear or established, routine use of these modifications is not supported by the data.
As with most facial aesthetic procedures, for upper cheiloplasty a non-aesthetically appealing final scar or adverse scarring are a major concern for patients and surgeons. Various studies have shown the rates of adverse scarring to be 1–5% [6, 18, 20]. This review found the incidence of these complications to be higher. The lip advancement techniques are associated with the lowest rate of adverse scarring (3.2%), whereas the subnasal lift techniques have higher rates of the adverse scarring (6.7–10.5%). Given the lack of standardization of technique and approach among the studies, these rates might be falsely elevated. There is a tendency for surgeons to master a small number of upper cheiloplasty techniques and apply them broadly. It is proposed that expanding the armamentarium to allow for an individualized approach would improve patient selection and technique application, which would potentially reduce the scarring burden and further improve outcomes.
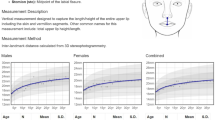
Thorough understanding of centrofacial aging may alter the surgical planning and treatment, therefore it warrants discussion. Effective individualized surgical planning is exceptionally challenging without a comprehensive understanding of the anatomic concepts of the centrofacial area and the upper lip subunit. Recently, Lambros demonstrated with three-dimensional imaging that aging is almost identical in men and women [26]. The entire upper lip subunit elongates, recesses and thins with aging, and the nasolabial folds become more prominent [26, 27]. Aging also results in bony resorption, which is most profound at the maxilla and the alveolar ridge. Histologically, the elastin and collagen fibers are degraded in time, and the orbicularis oris muscle fibers atrophy [27, 28]. Similar anatomic observations were made following photometric and radiologic magnetic resonance imaging (MRI) analysis [9, 29, 30]. In addition, it was found that the parasagittal portion of the lip is lengthened to a lesser degree than in its sagittal plane [30]. The significant difference in changes between sagittal and parasagittal measurements can be explained by the difference in mobility between these two planes, corresponding to the landmarks separating the medial and lateral upper lip subunits.
The most profound thinning occurs at the vermilliocutaneous junction [9, 30]. Tonnard et al. expertly described their approach by utilizing multiple fat grafting techniques, each tailored to restore gross projection, lip volumization, lip definition and rhytid effacement [9, 30,31,32]. As in the case of cheiloplasty by skin excision, more data are warranted in order to better characterize the role of micro- and nanofat grafting as an adjunct to surgical upper lip enhancement. Nonetheless, a multimodal approach should be considered in order to address the gestalt of facial aging. Upper cheiloplasty techniques and adjuvant procedures in relation to the dynamic aging process should be the focus of further studies.
We acknowledge the limitations of this systematic review, such as the lack of standardization of the studies and the variability of the data. Our results were restricted by the lack of strength of the available data. Inter-study comparisons were not possible. On the other hand, this is the first study to examine the literature on the surgical techniques and outcomes of upper lip enhancement.
Conclusions
This review provides an overview of several techniques and modifications for upper lip enhancement. It highlights the paucity of high-quality data on their application and optimizing patient selection. Promising satisfaction rates and relatively low complication rates suggest a more prominent role for surgical cheiloplasty in facial rejuvenation. Advances in the understanding of facial aging support the use of surgical lip enhancement. The utilization of adjunct procedures such as fat grafting merits further investigation.
References
Marques A, Brenda E (1994) Lifting of the upper lip using a single extensive incision. Br J Plast Surg 47(1):50–53
American Society of Plastic Surgeons. 2018 Cosmetic plastic surgery statistics. https://www.plasticsurgery.org/documents/News/Statistics/2018/plastic-surgery-statistics-full-report-2018.pdf. Accessed 3 Apr 2020
Gondes-Ulloa M (1976) The ageing upper lip. Transactions of the 6th International Congress of Plastic and Reconstructive Surgery, 1975. Ed. Marchac D and Hueston JT. Paris. Masson
Lee DE, Hur SW, Lee JH, Kim YH, Seul JH (2015) Central lip lift as aesthetic and physiognomic plastic surgery: the effect on lower facial profile. Aesthet Surg J 35(6):698–707
Salibian AA, Bluebond-Langner R (2019) Lip lift. Facial Plast Surg Clin North Am 27(2):261–266
Austin HW (1986) The lip lift. Plast Reconstr Surg 77(6):990–994
Fanous N (1983) Correction of thin lips: "lip lift". Plast Reconstr Surg 74(1):33–41
Holden PK, Sufyan AS, Perkins SW (2011) Long-term analysis of surgical correction of the senile upper lip. Arch Facial Plast Surg 13(5):332–336
Tonnard PL, Verpaele AM, Ramaut LE, Blondeel PN (2019) Aging of the upper lip: part II. evidence-based rejuvenation of the upper lip—a review of 500 consecutive cases. Plast Reconstr Surg. 143(5):1333–1342
Cardoso AD, Sperli AE (1971) Rhytidoplasty of the upper lip. In: Hueston JT (ed): Transactions of the 5th International Congress of the IPRS. Melbourne: Butterworth
Rozner L, Isaacs GW (1981) Lip lifting. Br J Plast Surg 34(4):481–484
Talei B (2019) The modified upper lip lift. Facial Plast Surg Clin North Am 27(3):385–398
Felman G (1993) Direct upper-lip lifting: a safe procedure. Aesthet Plast Surg 17(4):291–295
Santanch P, Bonarrigo C (2004) Lifting of the upper lip: personal technique. Plast Reconstr Surg 113(6):1828–1835
Li YK, Ritz M (2018) The modified bulls horn upper lip lift. J Plast Reconstr Aesthet Surg 71(8):1216–1230
Jung J-A, Kim K-B, Park H, Dhong E-S, Han S-K, Kim W-K (2019) Subnasal lip lifting in aging upper lip. Plast Reconstr Surg 143(3):701–709
Pan B-L (2017) Upper lip lift with a “T”-shaped resection of the orbicularis oris muscle for Asian perioral rejuvenation: a report of 84 patients. J Plast Reconstr Aesthet Surg 70(3):392–400
Echo A, Momoh AO, Yuksel E (2011) The no-scar lip-lift: upper lip suspension technique. Aesthetic Plast Surg 35(4):617–623
Mommaerts MY, Blythe JN (2016) Rejuvenation of the ageing upper lip and nose with suspension lifting. J Craniomaxillofac Surg 44(9):1123–1125
Raphael P, Harris R, Harris SW (2014) The endonasal lip lift: Personal technique. Aesthet Surg J 34(3):457–468
Waldman SR (2007) The subnasal lift. Facial Plast Surg Clin North Am 15(4):513–516
Farkas LG, Munro IR (1987) Anthropomorphic facial proportions in medicine. Charles C Thomas Publisher, Springfield, IL, pp 25–79
Powell N, Humphreys B (1984) Proportions of the aesthetic face. Thieme-Stratton Inc, New York, NY
Morrison SD, Vyas KS, Motakef S, Gast KM, Chung MT, Rashidi V, Satterwhite T, Kuzon W, Cederna P (2016) Facial feminization: systematic review of the literature. Plast Reconstr Surg 137:1759–1770
Georgiou CA, Benatar M, Bardot J, Santini J, Sicard BC (2014) Morphologic variations of the philtrum and their effect in the upper lip lift. Plast Reconstr Surg 134(6):996e–e997
Lambros V (2020) Facial aging: a 54-year, three-dimensional population study. Plast Reconstr Surg 145(4):921–928
Lambros V, Amos G (2016) Three-dimensional facial averaging: A tool for understanding facial aging. Plast Reconstr Surg 138:980e–982e
Glaser DA, Lambros V, Kolodziejczyk J, Magyar A, Dorries K, Gallagher CJ (2018) Relationship between midface volume deficits and the appearance of tear troughs and nasolabial folds. Dermatol Surg 44(12):1547–1554
Iblher N, Kloepper J, Penna V, Bartholomae JP, Stark GB (2008) Changes in the aging upper lip: a photomorphometric and MRI-based study (on a quest to find the right rejuvenation approach). J Plast Reconstr Aesthet Surg 61:1170–1176
Ramaut L, Tonnard P, Verpaele A, Verstraete K, Blondeel P (2019) Aging of the upper lip: part I: a retrospective analysis of metric changes in soft tissue on magnetic resonance imaging. Plast Reconstr Surg 143(2):440–446
Zeltzer AA, Tonnard PL, Verpaele AM (2012) Sharp-needle intradermal fat grafting (SNIF). Aesthet Surg J 32(5):554–561
Tonnard PL, Verpaele AM, Zeltzer AA (2013) Augmentation blepharoplasty: a review of 500 consecutive patients. Aesthetic Surg J 33(3):341–352
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yamin, F., McAuliffe, P.B. & Vasilakis, V. Aesthetic Surgical Enhancement of the Upper Lip: A Comprehensive Literature Review. Aesth Plast Surg 45, 173–180 (2021). https://doi.org/10.1007/s00266-020-01871-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-020-01871-3