
Abstract
Background
Hyaluronic acid (HA) injection is popular in cosmetic surgery because of its minimal invasion and immediate recovery. However, few injection techniques are specifically designed for Asians, considering their aesthetic and structural differences from those of Caucasians.
Methods
The midline volume injection technique was performed on 37 Asian females and 3 males at sites including the forehead, glabella, nasal dorsum, nasal base and chin. The treatment focused on improving the facial profile projection. 3D image data were collected, and facial aesthetic angles were calculated. Volume changes in facial parts were analyzed before injection and during follow-up. Patient satisfaction was assessed using the visual analog scale (VAS).
Results
The average injected filler volume was 6.14 ± 2.82 ml. The treatment optimized the facial contour and produced instant facial rejuvenation. On 3D images, the average midline volume increased by 6.02 ± 2.23 ml. An average volume decrease of 3.92 ± 1.94 ml was observed in the cheeks and was positively related to the increased midline volume. The average nasolabial and nasal facial angles were increased from 100.00 ± 7.37° to 107.93 ± 9.01° and 28.78 ± 3.28° to 31.78 ± 2.97°, while the mentolabial angle was decreased from 146.55 ± 7.83° to 141.13 ± 6.23°. The mean VAS scores were 2.28 ± 1.27 immediately after injection and 2.56 ± 1.20 after 6 months.
Conclusions
The midline volume injection technique of HA fillers is suitable for Asians. It greatly enhances the facial profile, as illustrated by volume changes in 3D images, leading to a more attractive facial appearance.
Level of Evidence V
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Currently, influenced by the Western culture, Asians prefer a more three-dimensional face, of which the determining factor is the degree of the midline projection of the face. Unlike Caucasians, Asians typically have a flattened facial contour, consisting of a flat forehead, low supraorbital ridge, depressed nasal dorsum, blunt nasal tip and retrusive chin [1]. Additionally, wide zygomatic and mandible bones aggravate the flat contour and make a person look older than he/she actually is. Several online questionnaire surveys have shown that in recent years, nonsurgical rhinoplasty and mentoplasty have become popular procedures in Asia for achieving a more three-dimensional face. Currently, injectable hyaluronic acid (HA) fillers are more frequently employed because of their minimal invasiveness, convenience and lack of convalescence.
There are some guidelines for HA injection techniques in Caucasian patients. In a clinical study by Jones and Murphy [2], 235 subjects with age-related midface volume deficits received treatment with the injection of a total mean of 6.65 ml of HA filler. The effect was obvious and long-lasting, as observed after 2 years. Research by Glaser et al. [3] showed that the duration of the effect was closely related to the injection volume. These guidelines show that a large injection volume could achieve a stable effect, but the mentioned injection sites may not be completely suitable for Asians, considering the anatomical and aesthetic differences between races. For example, it seems effective to perform a lateral cheek injection over the zygomatic bone to correct volume loss with aging [4]. However, this injection method might result in a wider midface, which caters to Caucasian aesthetics, whereas a wider midface is considered an unattractive feature in Asian culture.
Thus, the author aims to present a more appropriate facial rejuvenation and contouring injection technique for Asians, i.e., midline volume injection, which requires approximately 3–16 ml of HA filler to augment the volume of the midline and improve the protrusion of the forehead, nose and chin. Modification of the midline produces marked changes in facial appearance, causing the face to look younger, slimmer and more three dimensional.
Materials and Methods
The study was carried out from June 2017 to May 2019. The patients included 37 Asian females and 3 males, aged from 21 to 45 years (average age 31.55 ± 6.43 years), seeking a younger and more appealing appearance. All 40 patients were given combined treatment with multisection injections along the midline. Considering the need for sufficient support to augment the forehead, nose and chin, high concentrations of HA (from 22 to 24 mg/ml) were used. The follow-up times ranged from 6 to 24 months. The longest time between pre- and postinjection 3D image acquisition was 6 months.
Measurement and Effect Evaluation
Two-dimensional (2D) photographs were taken preinjection and immediately postinjection in the anteroposterior, oblique, and lateral positions, and three-dimensional (3D) images were acquired using a 3D camera (LifeViz, Inc., France) from four positions, followed by computer-assisted reconstruction (Quantificare LifeViz, Inc., France). During the imaging process, the patient should remain motionless; otherwise, calculation of the volume changes might be inaccurate. Through 3D imaging technology, full facial morphology data were collected. Based on the data, the 3D image of a patient was modified during the consultation stage to mimic the effect of the HA filler injection treatment. After consent was obtained, the total dosage of HA was calculated using the 3D imaging system.
The measurement points and angles were marked to evaluate the postinjection effects (Fig. 1). In the sagittal view, the measurement points marked included the following: (1) glabella (g): the most prominent point between the eyebrows; (2) nasion (n): intersection of the frontal and two nasal bones; (3) pronasale (prn): the most protruded point of the apex nasi; (4) subnasale (sn): the midpoint of the angle at the base of the columella where the lower border of the nasal septum and the surface of the upper lip meet; (5) labrale superius (ls): midpoint of the upper vermillion line; (6) labrale inferior (li): midpoint of the lower vermillion line; (7) supramentale (sm): the most posterior midline point above the chin; and (8) pogonion (pg): the most anterior midpoint of the chin, located on the skin surface in the front of the identical bony landmark of the mandible. Important aesthetic angles were also measured, including the nasolabial angle, nasofrontal angle, nasal facial angle and mentolabial angle, to evaluate the effects observed in this study.

Measurement points marked on 3D images
Analysis of the 3D images (Quantificare LifeViz, Inc., France) clearly showed the effect of the midline injections in terms of the soft tissue volume in the pre- and postinjection images [5]. In the 3D figures, warm tones indicate regions of increased volume, while cold tones indicate regions of decreased volume. Accurate volume differences in specific regions were calculated to evaluate the effect, and volume changes were analyzed with SPSS version 22.0 (SPSS, Inc., Chicago, IL, USA).
The effects were also evaluated using a visual analog scale (VAS), which is a subjective scale of the patient’s feelings about the treatment [6]. Patients were asked to grade their degree of satisfaction (0 = very satisfied, 10 = very dissatisfied) immediately after injection and after 6 months.
Injection Technique
Nasal Injections
The nasal injection was performed in the following order: (1) nasal spine, (2) columella, (3) nasal tip, (4) nasal dorsum and (5) nasion.
Sharp needles (27 G) were used in each step. First, the needle was inserted through the junction of philtrum and columella, and a supraperiosteal bolus was injected into the anterior nasal spine. After the needle was aspirated, HA was injected very slowly with low pressure. The next insertion was made in the middle of the columella, and HA was injected into the space behind the columella on either side of the anterior septum cartilage. The placement of filler at these two sites elevated the nasal base and increased the nasolabial angle. Based on the results reported by Armijo BS, Brown M, and Guyuron B [7], the ideal nasolabial angle is 93.4° to 98.5° for men and 95.5° to 100.1° for women. Some surgeons added filler directly at the nasal tip, just beneath the skin, to adjust the tip shape and redefine the tip presentation point. This procedure is not applicable to all patients because it does not create a sufficient projection, especially in those patients with a plump, soft nose tip. Injecting filler deeper in the perichondrium between the alar cartilages is more effective for reshaping the tip. Eventually, the injection for filling the nasal dorsum and nasion was accomplished by inserting a needle deeply at multiple points to precisely cover the total length. Correction of the inadequate dorsum provided a nasofrontal angle of approximately 115° to 125°, which catered to the aesthetic standard of an ideally proportioned face [8].
Forehead and Glabella Injections
A forehead is considered beautiful if it has a gentle vertical convex ogee curve from the trichion to the supraorbital ridge. A flattened or sloping brow greater than 15° from vertical is often considered an undesirable forehead appearance in Asian female.
To alter the frontal contour, the author emphasized three injection sites along the midline: two points at the upper and middle parts of the forehead and one at the glabella. A supraperiosteal bolus injection was performed using a sharp 27-G needle. The needle was aspirated before injection, and the tip was kept deep to avoid the supratrochlear and supraorbital vessels. It was necessary to massage the injection sites to achieve a smooth contour; inadequate massage could lead to a rugged forehead surface that is not aesthetically appealing [9].
Chin Injections
For Asians, an oval and more delicate chin along with a narrower mandible is preferred over traditional Caucasian chin features. As a general rule, the anterior projection of the chin in women should be slightly behind or just at the line drawn through the nasion and perpendicular to the Frankfort horizontal plane. An appropriate chin projection and a compact jawline are considered the standards of youth and beauty.
With regard to chin augmentation, primarily regarding the position of the sharp 27-G needle at the pogonion, the needle was aspirated before injection and then inserted deeply to access the avascular plane. The needle was maintained at the midline to deliver a supraperiosteal bolus injection. Subsequently, the filler was supplemented at two sites on either side of the pogonion to ensure a smooth jawline. Attention was paid not to overfill the site, which could lead to the chin appearing heavy and artificial.
Results
Case Report
Case 1
A 42-year-old female who had an ideal oval frontal facial contour but a defective side profile and aged appearance with an insufficient projection (Fig. 3) desired to look younger. HA was injected at a volume of 1.8 ml to elevate the nasal tip; 0.7 ml was injected in the nasal dorsum and nasion to mold a prominent profile. Next, 1 ml was injected into both the glabella and the frontal periosteum to achieve a youthful upper face façade. Then, 2 ml was injected into the chin to conform to the aesthetic plane, and an additional 0.5 ml was injected into the underlip. Volume changes are shown on 3D images, including a 7.1-ml increase in the midline and a 3.1-ml decrease in the cheeks (Fig. 4).
Case 2
A 38-year-old female with a short, round and sagging face (Fig. 5) complained of flatness of the face that aggravated the appearance of aging. During the initial and following touch-up treatments, a total of 8 ml of HA was used to create a plump forehead; 3 ml of HA was injected to prolong the chin, and 5 ml was injected to project the nose. Meanwhile, an embedded-suture double-eyelid procedure was performed to enlarge the eyes. The face was prolonged, and it looked slimmer and much younger after the treatment. At 2 years after the procedure, the rejuvenation effect was still stable and satisfactory.
Case 3
A 25-year-old female demonstrated a complanate facial contour (Fig. 6). The patient requested an improvement in her facial profile and tightening her face. The unpleasant side profile consisted of an insufficient nose, a flat forehead and a receding chin. A total of 4 ml of HA was injected to raise the nose; 3 ml was placed in the nasal base, and 1 ml was placed in the nasal dorsum. Meanwhile, 3.5 ml of HA was injected in the whole forehead, and 3.5 ml was injected in the chin to coordinate these parts. Supplementary injections of 4 ml in the chin and 6 ml in the tempus were given 10 days later. After 6 months, the 3D volume images showed that little material had been absorbed, i.e., approximately 0.6 ml in the nose and 0.7 ml in the forehead (Fig. 7). The patient still maintained a stereoscopic profile and a youthful appearance.
Data Analysis
An average of 6.14 ± 2.82 ml of filler was used per patient. The 3D volume figures clearly showed the location and dose of the filler. The data for volume augmentation of the frontal, nasal and chin areas were statistically analyzed. The average volume of the nose, forehead, and chin increased by 3.10 ± 1.37 ml, 1.80 ± 1.01 ml, and 2.71 ± 1.52 ml, respectively.
The average nasolabial angle increased from 100.00 ± 7.37° to 107.93 ± 9.01°, which indicated correction of the depressed nasal tip and sunken nasal base. The average nasal facial angle also increased from 28.78 ± 3.28° to 31.78 ± 2.97°. The nasofrontal angle was 141.08 ± 6.21° preinjection and was not significantly changed postinjection, indicating that the projection of the nose was integrally augmented but the nasal dorsum was not overfilled. The mentolabial angle decreased from 146.55 ± 7.83° to 141.13 ± 6.23° due to the protruding chin.
The author detected a thought-provoking phenomenon in which the filling of the midline was always accompanied by a volume reduction in some other regions covering the infraorbital bone and the cheeks. The average increase in volume was 6.02 ± 2.23 ml after midline filling. The average decrease in volume of the cheeks was 3.92 ± 1.94 ml. A scatter plot was made, and a best-fit line was drawn to observe the relationship between the decreased volume of the cheeks and increased volume of the midline (Fig. 2). Linear regression analysis yielded significant results (F < 0.05, ANOVA), and applying the T-test to the independent variables resulted in a P value < 0.05; thus, the linear relationship between the decrease in cheek volume and increase in midline volume was confirmed. The regression equation was Y = 0.36 + 0.59X.

Scatter plot and best-fit line of the increased midline volume and decreased cheek volume. Linear regression analysis verified that they were positively correlated
Patients who underwent treatment with midline injection exhibited marked immediate alterations (Fig. 3), as illustrated by volume changes in the 3D images (Fig. 4). During the follow-up period, the author also found that the rejuvenation and contouring effects were still obvious at 2 years postinjection (Fig. 5). As shown in the photographs (Fig. 6) and 3D volume figures (Fig. 7), the HA filler was slightly absorbed, and the volume change mentioned was still present 6 months postinjection.

Photographs obtained preinjection (a, c) and immediately postinjection (b, d)

3D volume figure showing the volume augmentation of the nose, forehead and chin, as well as a decrease in the volume of the cheeks compared to preinjection

Photographs obtained preinjection (a, c) and at 2 years postinjection (b, d)

Photographs obtained preinjection (a, c), and at 6 months after supplementary injection (b, d)

3D volume images immediately after supplementary injection showing volume augmentation of the nose, forehead and chin and the volume decrease in the cheeks compared to the preinjection volumes (left). The effect was stable after 6 months of follow-up compared to preinjection (right)
No serious adverse events were observed during the follow-up period. The mean VAS scores were 2.28 ± 1.27 immediately postinjection and 2.56 ± 1.20 after 6 months. There was no significant difference in the VAS score between immediately and 6 months postinjection, indicating that most patients remained satisfied with their results during the follow-up period.
Discussion
Currently, Asian aesthetics are partly influenced by the Western culture. “Blended aesthetic” Asian ethnic features mixed with the 3D facial contours of Caucasian features are popular in Asia. However, there are still some differences in aesthetic standards between Asians and Caucasians. For example, in terms of rejuvenation, Caucasian patients are more likely to choose filler injections in the cheeks and achieve satisfactory results [10]. However, with regard to Asian patients, cheek augmentation is rarely performed separately. Based on our clinical experience, plump cheeks do not meet the aesthetic standards of Asian patients, whereas a smaller and slimmer face is preferred.
Typically, Asians have flattened faces because of the lack of projection of several sites from the midline. These features make the individual look older and make the face look larger. Based on the anatomical characteristics and the aesthetic standard, the author developed the midline volume injection technique, which is specifically designed for Asians. The author regards the most projected structures on the midline of the face to serve as the hallmarks of facial beauty, and this technique focuses on integrally improving the facial stereoscopic degree for facial rejuvenation. Through the augmentation of these structures, an exotic appearance is made, and the goals of contouring can be achieved.
Reshaping the nose, which is the most crucial component of the whole procedure, should be considered primarily. Unlike Caucasians, Asians usually have a low nasal dorsum, bulbous and poorly projected tips, a small septum, a short nasal columella, wide nostrils and an acute nasolabial angle [11]. Furthermore, the facial skeleton changes with aging because of bone absorption [12]. Receding of the pyriform aperture and maxilla results in a lengthened philtrum and sunken nasal base. The nasal tip rotates downward, leading to a decreased nasolabial angle. These features make the midface look depressed, which aggravates the perception of aging. The majority of the filler is distributed to increase the nasolabial angle and raise the nasal base while projecting the nasal tip [13]. Elevation of the tip narrows the nostrils and the alae nasi, making the nasal shape look slimmer and more exquisite.
To match the prominent nose, a plump forehead is necessary. During injection of the forehead and the glabella, the placement of filler is emphasized in the middle area because a sunken glabella is regarded as a feature of elderly people. Caution must be used to not inject too much on the lateral sides of the forehead; the consequence might be a larger forehead and a wider upper face, features that are not favored by Asians. Like a continuous mountain chain, the glabella extends bilaterally as the arcus superciliaris. Filling of this part is implemented to fit the projection of the frontal bone. A study by Lambros [14] showed that volumizing the brow with HA fillers had a long-lasting effect on peri-orbital rejuvenation. On the 3D volume images, the author discovered a volume decrease in the orbital region when the upper face padding was fulfilled, showing that the orbits became deeper. Perhaps this result is due to the lifting of the upper eyelids, but exactly how the frontal injections affect the orbital soft tissue deserves further research.
Chin retrusion is common in Asians and is considered an unsatisfactory facial feature. Severe retrusion has a significant impact on the lower facial contour, making a person look obtuse and cowardly. Slight retrusion is identified as a characteristic of youthful faces and is acceptable, but retrusion over 4 mm is considered to require treatment [15]. Correct injection leads to the inferior positioning of the pogonion, making it adapt to the aesthetic line in the lateral view. The combination of nasal and chin filling is suitable for a set of patients who have a sagging face, double chin and slack jawline, contributing to the lift of the lower face [16].
Recently, combined treatments with botulinum toxin and HA have been commonly performed. Several relevant articles have recommended injection doses. Injection into the depressor septi nasi muscle with 2–6 units of onabotulinumtoxin A can elevate the nasal tip [17, 18], and the injection of 4–8 units of botulinum toxin into the mentalis can augment chin protrusion [19]. The author has made some attempts to assist the midline HA injections with botulinum toxin. This method relaxes the mimetic muscles and may contribute to the tightening of soft tissues around the midline HA injection by facilitating sliding of the superficial musculo-aponeurotic system (SMAS), but the injection points and most suitable dosages require further research.
Throughout the entire procedure, sharp needles were applied to place the filler in the deep plane to achieve a better effect. Such an injection technique results in precise filler placement, simulating the natural bone structure to create a natural and pleasing appearance. Fillers remain stable under the pressure of surrounding dense tissues and do not shift along with mimetic muscle movement, which minimizes shape distortion. The deep injection of HA filler avoids defects, such as swelling and displacement, which can be observed following traditional injections into superficial layers of the deep dermis or subcutaneous injections [20].
Another advantage of the deep-plane midline injection technique is that it reduces the risk of vessel complications. Park et al. [21] summarized HA-filler-related complications, including nodular masses, inflammation, tissue necrosis and dyspigmentation. Among them, filler emboli can lead to the most serious complications, such as skin necrosis and blindness [22, 23]. Midline injection has enhanced the safety because the incidence of large arteries crossing the midline is quite rare—less than one in 45 [24].
Throughout the injection process, 3D imaging technology was used. It not only captured the aesthetic improvements posttreatment, showing 360° of the facial aspect, but also definitively tracked the injection sites and accurately assessed the volume augmentation or reduction. On the 3D images, the HA injections demonstrated amazing instantaneous and long-term effects in terms of contouring and rejuvenation, as shown by the volume increase along the midline and decreases in other regions. During the subsequent follow-up period, 3D images were taken so that the absorption volume of the HA filler could be calculated. Thus, the author found a stable long-term effect after 6 months due to reduced absorption.
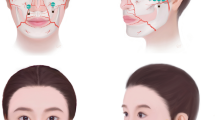
The relationship between midline volume augmentation and cheek volume reduction based on the 3D data was mentioned and mathematically described above, but the mechanism remains undetermined. The traction of adjacent soft tissue might be a reasonable explanation. Schenck et al. [25] described the presence of distinct subcutaneous facial fat compartments, including superficial nasolabial, medial cheek, middle cheek, lateral cheek, superficial superior temporal, superficial inferior temporal, jowl, superficial central and superficial lateral compartments. Among them, the superficial nasolabial, medial cheek and jowl compartments undergo significant inferior displacement with age [26]. The author speculated that fillers placed deeply on the midline create tension, dragging the soft tissues, especially the fat compartments, toward the midline. The displacement of fat compartments greatly relies on the presence of facial soft tissue spaces situated between the SMAS and periosteum. The spaces that are meaningful to our research include the prezygomatic space [27], the premasseter space [28] and the premaxillary space [29]. Because of these spaces, fat compartments can easily slide with the SMAS on the periosteum and become centralized relative to the midline of the face (Fig. 8). Therefore, further research should be performed to anatomically verify this theory.

Asians have flattened facial contours (left). After HA filler was injected into the midline, the fat compartments and other soft tissues were tensioned and centralized based on soft tissue space, making the face appear slimmer, more three dimensional and more youthful (right)
Conclusion
HA injection is popular among patients who are reluctant to undergo surgery. However, there are few techniques for filler injection that are specifically suitable for Asians in view of their aesthetic and structural differences from Caucasians. Considering the facial features of Asians, especially the flatness and width of the face, the midline volume injection technique, which focuses on correcting the flat forehead, depressed nose and retrusive chin, can greatly enhance the facial profile and yield a youthful appearance. The treatment resulted in fantastic instant and long-term facial rejuvenation effects, as illustrated by the 3D volume measurements, leading to a younger, slimmer, more 3D and more attractive facial appearance.
References
Wirthlin J, Kau CH, English JD, Pan F, Zhou H (2013) Comparison of facial morphologies between adult Chinese and Houstonian Caucasian populations using three-dimensional imaging. Int J Oral Maxillofac Surg 42:1100–1107
Jones D, Murphy DK (2013) Volumizing hyaluronic acid filler for midface volume deficit: 2-year results from a pivotal single-blind randomized controlled study. Dermatol Surg 39:1602–1612
Glaser DA, Kenkel JM, Paradkar-Mitragotri D, Murphy DK, Romagnano L, Drinkwater A (2015) Duration of effect by injection volume and facial subregion for a volumizing hyaluronic acid filler in treating midface volume deficit. Dermatol Surg 41:942–949
de Maio M, DeBoulle K, Braz A, Rohrich RJ (2017) Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the midface. Plast Reconstr Surg 140:540e–550e
Skvara H, Burnett P, Jones J, Duschek N, Plassmann P, Thirion JP (2012) Quantification of skin lesions with a 3D stereovision camera system: validation and clinical applications. Skin Res Technol 19:e182–e190
Voutilainen A, Pitkaaho T, Kvist T, Vehvilainen-Julkunen K (2016) How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J Adv Nurs 72:946–957
Armijo BS, Brown M, Guyuron B (2012) Defining the ideal nasolabial angle. Plast Reconstr Surg 129:759–764
Swift A, Remington K (2011) BeautiPHIcation: a global approach to facial beauty. Clin Plast Surg 38:347–377
de Maio M, Swift A, Signorini M, Fagien S (2017) Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the upper face. Plast Reconstr Surg 140:265e–276e
Kestemont P, Cartier H, Trevidic P, Rzany B, Sattler G, Kerrouche N, Dhuin JC (2012) Sustained efficacy and high patient satisfaction after cheek enhancement with a new hyaluronic acid dermal filler. J Drugs Dermatol 11:s9–s16
Han X, Hu J, Cheng L, Li F (2015) Multiplane hyaluronic acid (EME) in female Chinese rhinoplasty using blunt and sharp needle technique. J Plast Reconstr Aesthet Surg 68:1504–1509
Mendelson B, Wong CH (2012) Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthet Plast Surg 36:753–760
Beer K, Solish N (2006) Reshaping the nose with injectable agents. Cosmet Dermatol 19:745–752
Lambros V (2009) Volumizing the brow with hyaluronic acid fillers. Aesthet Surg J 29:174–179
Wilson MJV, Jones IT, Butterwick K, Fabi SG (2018) Role of nonsurgical chin augmentation in full face rejuvenation: a review and our experience. Dermatol Surg 44:985–993
Braz AV, Louvain D, Mukamal LV (2013) Combined treatment with botulinum toxin and hyaluronic acid to correct unsightly lateral-chin depression. An Bras Dermatol 88:138–140
Dayan SH, Kempiners JJ (2005) Treatment of the lower third of the nose and dynamic nasal tip ptosis with Botox. Plast Reconstr Surg 115:1784–1785
Redaelli A (2008) Medical rhinoplasty with hyaluronic acid and botulinum toxin A: a very simple and quite effective technique. J Cosmet Dermatol 7:210–220
Hsu AK, Frankel AS (2017) Modification of chin projection and aesthetics with onabotulinumtoxin A injection. JAMA Facial Plast Surg 19:522–527
Xue K, Chiang CA, Liu K, Gu B, Li Q (2012) Multiplane hyaluronic acid rhinoplasty. Plast Reconstr Surg 129:371e–372e
Park TH, Seo SW, Kim JK, Chang CH (2011) Clinical experience with hyaluronic acid-filler complications. J Plast Reconstr Aesthet Surg 64:892–896
Ozturk CN, Li Y, Tung R, Parker L, Piliang MP, Zins JE (2013) Complications following injection of soft-tissue fillers. Aesthet Surg J 33:862–877
Beleznay K, Carruthers JD, Humphrey S, Jones D (2015) Avoiding and treating blindness from fillers: a review of the world literature. Dermatol Surg 41:1097–1117
Tansatit T, Moon HJ, Rungsawang C, Jitaree B, Uruwan S, Apinuntrum P, Phetudom T (2016) Safe planes for injection rhinoplasty: a histological analysis of midline longitudinal sections of the Asian nose. Aesthet Plast Surg 40:236–244
Schenck TL, Koban KC, Schlattau A, Frank K, Sykes JM, Targosinski S, Erlbacher K, Cotofana S (2018) The functional anatomy of the superficial fat compartments of the face: a detailed imaging study. Plast Reconstr Surg 141:1351–1359
Gierloff M, Stohring C, Buder T, Gassling V, Acil Y, Wiltfang J (2012) Aging changes of the midfacial fat compartments: a computed tomographic study. Plast Reconstr Surg 129:263–273
Mendelson BC, Muzaffar AR, Adams WP Jr. (2002) Surgical anatomy of the midcheek and malar mounds. Plast Reconstr Surg 110: 885–896 (discussion 897–911)
Mendelson BC, Freeman ME, Wu W, Huggins RJ (2008) Surgical anatomy of the lower face: the premasseter space, the jowl, and the labiomandibular fold. Aesthetic Plast Surg 32:185–195
Wong CH, Mendelson B (2013) Facial soft-tissue spaces and retaining ligaments of the midcheek: defining the premaxillary space. Plast Reconstr Surg 132:49–56
Funding
The authors received no financial support for the research and authorship of this article.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The author has no conflicts of interest to declare with respect to the authorship and publication of this article.
Ethical Approval
This study was reviewed and approved by the Ethics Committee of Shanghai Ninth Hospital, Shanghai Jiao Tong University School of Medicine. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
The patients were fully informed about the treatment procedure and possible side effects. An informed consent form was signed by all patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xiong, Z., Jiang, Z. & Liu, K. Midline Volume Filler Injection for Facial Rejuvenation and Contouring in Asians. Aesth Plast Surg 43, 1624–1634 (2019). https://doi.org/10.1007/s00266-019-01498-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-019-01498-z