
Abstract
Background
Compared to the traditional transcutaneous approach, a safe and effective lower eyelid blepharoplasty has been recognized. In 2007, Sadove first reported a series of patients treated with transconjunctival septal suturing, but the inferior orbitopalpebral sulcus was not totally improved.
Purpose
Orbital septal fat release and preservation through the transconjunctival approach was used to treat 20 young patients with bulging bags and inferior orbitopalpebral sulcus.
Method
The orbital septal fat was released and transferred to infraorbital rim to be a base for the inferior orbitopalpebral sulcus.
Result
Obvious bulging fat was released, and the orbitopalpebral sulcus was flattened by released and excessive orbital septal fat. Satisfactory results were achieved.
Conclusion
The results achieved from this series of patients indicate that orbital septal fat release and preservation through the transconjunctival approach for reducing the orbitopalpebral sulcus is a safe and effective treatment for bulging fat and orbitopalpebral sulcus in young patients.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Lower eyelid blepharoplasty is a popular cosmetic procedure [1]. Multiple techniques have been advocated in this procedure. The debates mainly focus on whether the best approach is transcutaneous or transconjunctival, fat resection or preservation [2, 3] and orbital repair or tightening the orbicularis oculi. The transconjunctival approach in lower lid blepharoplasty was popularized by Tessier for blepharoplasty after congenital malformations [4]. From the 1970s to early 1980s, the preliminary technique of transconjunctival blepharoplasty was the advocation of the utility of fat removal as conservative treatment for periorbital aging [5, 6]. Some recommended transconjunctival access to expose orbital fat for resection, pedicled fat repositioning or septal suturing [7–9].
We conducted an approach of orbital septal fat release and preservation through the transconjunctival route for reducing the inferior orbitopalpebral sulcus in lower eyelid blepharoplasty, which has brought us good results. This technique is best suited for patients with bulging fat of the lower eyelids and inferior orbitopalpebral sulcus, but no significant dermatochalasis, skin wrinkles or folds in the lower eyelid. The key concept of our technique is to incise open the orbital septal, release and preserve the orbital septal fat for reducing the bulging bags, and to transplant part of the fat to flat inferior orbitopalpebral sulcus.
Many young people in China present with visible bulging bags and an apparent inferior orbitopalpebral sulcus because of many factors including smoking, beer, staying up all night or genetic factors. They require cosmetic contouring with minimal injury. Thus, transconjunctival orbital septal fat release and preservation is a better choice for them instead of the transcutaneous approach, and the results were satisfactory. This is a report of a series of patients treated with the transconjunctival orbital septal fat release and preservation for reducing the inferior orbitopalpebral sulcus in lower eyelid blepharoplasty. It is a safe and reliable technique that achieves excellent cosmetic results.
Patients and Methods
Case Series
Between June of 2006 and April of 2016, 20 patients were included in this study (2 males and 18 females). Their ages ranged from 20 to 35 years (mean, 29 years). All patients presented with visible bulging fat of the lower eyelid and inferior orbitopalpebral sulcus; none had significant dermatochalasis or skin wrinkles in the lower eyelid. Patients with these conditions of dermatochalasis and skin wrinkles were excluded from the study and treated by other procedures. All cases were treated for the transconjunctival orbital septal fat release and preservation, and all patients included in the study ranged in follow-up from 2 months to 24 months (mean follow-up, 12 months). Photographs and clinical information were taken to evaluate the preoperative and postoperative outcome. All patients gave their informed consent prior to being treated.
Anatomy of Lower Eyelid
Our anatomical drawing provides an illustration of the surgical anatomy of the lower eyelid (Fig. 1). The formation of lower eyelid bags was related to orbicularis oculi muscle, orbital septal fat and eyelid skin. Loose eyelid skin and orbicularis oculi muscle or accumulated orbital septal fat lead to presentation with bulging fat of the lower eyelids. According to this anatomical structure, we conducted an operation by releasing and redistributing orbital septal fat through a conjunctival incision to reduce the apparent inferior orbitopalpebral sulcus and baggy fat. The key procedure was to incise open the conjunctiva and release and suture the fat to the rim of the periosteum of the orbital bone, reconstructing a strong support for the lower eyelid.

The anatomy of lower eyelid. The releasing and redistributing of orbital fat through conjunctiva incision was a key procedure for our patients
Surgical Techniques
The incision was designed on the conjunctiva of the lower eyelid. After infraorbital compression, a subtle color change from red to paler on the conjunctiva below the inferior edge of the tarsal plate will indicate the level at which the incision should be placed. The incision line was about 10 mm, which was placed 1–2 mm away from the lower edge of the lower eyelid tarsus (Fig. 2a). The conjunctiva was infiltrated with an injection of 1% lidocaine with 1:200,000 epinephrine along the incision line. After local anesthesia of about 5 min, the conjunctiva was incised. Using a combination of ophthalmic scissors, forceps and skin retractor, blunt and sharp dissection was done between the orbicularis oculi muscle and orbital septal (Fig. 2b). The orbital septal was cut open and the orbital septal fat was released on the periosteum (Fig. 2c). The dissection was conducted along the surface of the periosteum, which was inferior about 5–8 mm to the infraorbital rim (Fig. 3a).

The operation design and dissection. a The incision line about 10 mm was designed on the conjunctiva. b Dissection between the orbicularis oculi muscle and orbital septal. c Orbital septal fat was released and sutured on the surface of the periosteum

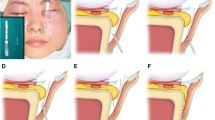
Intraoperative photograph of surgical procedures. a The dissection on the surface of the periosteum was inferior 5–8 mm to the infraorbital rim. b Exposure of three fat pads through cutting open the orbital septal. c The released fat was sutured and fixed on the infraorbital periosteum with 5–0 absorbable suture. d The needle was incised through fat. e The needle was incised back through the fat, and the fat was guided to fill the inferior orbitopalpebral sulcus. f A buried knot was tied
The orbital septal was exposed completely and cut open by ophthalmic scissors to release orbital septal fat pads. The orbital septal fat including medial, middle and lateral fat pads (Fig. 3b) will herniate itself due to the gravity and semi-mobile state of the fat tissue. Partial orbital septal fat was transferred to be a base below the inferior orbitopalpebral sulcus. After flattening the inferior orbitopalpebral sulcus, the redundant portion of fat was removed. With this procedure, the previous bulging fat was released to be a flat correction, and the inferior orbitopalpebral sulcus was also based fully. After being adjusted in the appropriate position, the released fat was sutured and fixed on the infraorbital periosteum with 5–0 polyglactin 910 (Vicryl, Ethicon) by a half-circle, round-bodied needle (Fig. 3c). The details of the method were that the suture was fixed through the infraorbital periosteum and the needle with suture incised through the fat, incised back through the same fat and tied in a buried knot (Fig. 3d–f). In this way, the middle, medial and lateral orbital septal fat was released and fixed over the infraorbital periosteum, separately. Completion of the release and fixation created a flat correction of the previously bulging fat and inferior orbitopalpebral sulcus. Once satisfactory contour was achieved, ophthalmic antibiotic ointment was instilled across the wound, and no suture was required for closure.
Results
All patients included in this study underwent transconjunctival orbital septal fat release and preservation. In this operation, appropriate patient selection was a key component. The included patients presented with visible bulging fat of the lower eyelids and inferior orbitopalpebral sulcus without apparent dermatochalasis, or skin wrinkles in the lower eyelid (Figs. 4a, 5a, 6a). After postoperative follow-up, previous bulging fat was released to be flat, and the inferior orbitopalpebral sulcus was flattened by released and excessive orbital septal fat (Figs. 4b, 5b, 6b). Stable results were achieved at 2 months and these results proved to be durable when assessed at 12 and 24 months. No complications such as hematomas, chemosis, infections or eyelid ectropion occurred. Patients were satisfied with the results.

A 25-year-old woman underwent transconjunctival orbital septal fat release and preservation for reducing the orbitopalpebral sulcus. a Preoperative frontal view. b 2-week postoperative frontal view

A 25-year-old woman underwent transconjunctival orbital septal fat release and preservation in bilateral lower eyelid blepharoplasty for reducing the orbitopalpebral sulcus. a Preoperative left oblique view. b 1-month postoperative left oblique view

A 25-year-old woman underwent transconjunctival orbital septal fat release and preservation for reducing the orbitopalpebral sulcus. a Preoperative right oblique view. b 2-month postoperative right oblique view
Discussion
Many factors contribute to the formation of bulging fat of the eyelid. Enlargement and accumulation of orbital septal fat among young patients was caused usually by genetic factors. Followed by age, the elasticity of eyelid skin is reduced, and the tension in the orbicularis oculi muscles and orbital septal is weak, which at last leads to the presentation of bulging bags. In addition, the gravity of orbital septal fat pushes the infraorbital superficial soft tissues toward the cheek, presenting with a shallow and narrow orbitopalpebral.
The transcutaneous approach is the traditional operative method for lower eyelid blepharoplasty. However, a potential issue about this procedure is that some patients complain of visible scarring on skin [10]. In some older patients with redundant eyelid skin, excessive orbital septal fat and a visible inferior orbitopalpebral sulcus, the transcutaneous incision designed by Hamra [3, 11] was generally used to preserve and release orbital fat, lift the orbicularis oculi muscle and remove loose and redundant skin. The transconjunctival technique undergoes a temporary period of swelling measured only by days and provides patients with a simple, low-risk and high-satisfaction procedure of correction of lower eyelid bags [9]. Furthermore, during the progress of the follow-up, ranging from 2 months to 24 months (mean follow-up, 12 months), the view of the lower eyelid was stable 2 months after the operation, and there was no significant difference between 2 months and 6 months or 8 months in the lower lid. Moreover, there was no cosmetic complaint about scarring.
It is commonly understood that the fat surrounding the eyes contributes to the normal and cosmetic appearance. Preservation of partial but not excessive fat is important for the eye’s youthful appearance. Fat pedicles and free fat transplantation could be placed over the infraorbital rim to fill and flatten the inferior orbitopalpebral sulcus. There is no risk of under correction or over correction of fat in bulging bags and depression. And the orbicularis muscle is not denervated and thus retains its strength. An attention is directed to release and fill appropriate fat over the infraorbital rim for the base of the inferior orbitopalpebral sulcus. Through effective redistribution of orbital septal fat, the deformity of the orbitopalpebral is corrected with a natural and youthful eye appearance. However, fat resection via the transcutaneous approach is followed by age appearance. And fat resection carries the risk of removing too much or little orbital fat, resulting in infraorbital depression and remaining bulging bags. Moreover, with the fat reset procedure via the transcutaneous approach, the risk of denervation of the orbicularis results in lid-tightening canthopexy or muscle plasty [12]. Disorders associated with orbicularis muscle paralysis denervated by muscle flaps [13] affect the anatomical position of the eyelid margin. These risks do not exist in transconjunctival repositioning of fat.
In our study, orbital septal fat release via the transconjunctival approach was applied in patients with an orbitopalpebral sulcus, dermatochalasis caused by redundant fat without redundant skin or wrinkles. Satisfactory results were achieved. Compared to the conventional way, transconjunctival orbital septal release and preservation selectively preserves fat to avoid infraorbital depression, lower eyelid ectropion and other complications due to excess removal of fat. At the same time, no treatment is required for the skin and orbicularis muscle, and the procedure has less bleeding with better and fast recovery.
In summary, the lower blepharoplasty described in this paper is most suitable for patients with visible bulging fat of the lower eyelid, a significant inferior orbitopalpebral sulcus, but without significant dermatochalasis or skin wrinkles in the lower eyelid.
References
Dupuis D, Rees TD (1971) Historical notes on blepharoplasty. Plast Reconstr Surg 47:246–249
Goldberg RA, Edelstein C, Balch K, Shorr N (1998) Fat repositioning in lower eyelid blepharoplasty. Semin Ophthalmol 13:103–106
Hamra ST (1995) Arcus marginalis release and orbital fat preservation in midface rejuvenation. Plast Reconstr Surg 96(2):354–362
Tessier P (1973) The conjunctival approach to the orbital floor and maxilla in congenital malformation and trauma. J Maxillofac Surg 1:1–3
Tomlison FB, Hovey LM (1975) Transconjunctival lower lid blepharoplasty for removal of fat. Plast Reconstr Surg 56:314–318
Cardosa de Castro CC (2004) A critical analysis of the current surgical concepts for lower lid blepharoplasty. Plast Reconstr Surg 111:794–796
de la Plaza R, Arroyo JM (1988) A new technique for the treatment of palpebral bags. Plast Reconstr Surg 81:677–687
Kawamoto HK, Bradley JP (2003) The tear “TROUF” procedure: transconjunctival repositioning of orbital unipedicled fat. Plast Reconstr Surg 112:1903–1907
Sadove RC (2007) Transconjunctival septal suture repair for lower lid blepharoplasty. Plast Reconstr Surg 120:521–529
DeMartelaere SL, Perman KI, Shore JW (2007) Orbital septal resection and the hanging curtain of fat. Ophthal Plast Reconstr Surg 23:349–354
Hamra ST (1996) The use of orbital fat preservation in facial aesthetic surgery a new concept. Clin Plast Surg 23:17–28
Glat PM, Jelks GW, Jelks EB, Wood M, Gadangi P, Longaker MT (1997) Evolution of the lateral canthoplasty: techniques and indications. Plast Reconstr Surg 100:1396
Ramirez OM, Santamarina R (2000) Spatial orientation of motor innervation to the lower orbicularis oculi muscle. Aesthetic Surg J 20:107
Acknowledgements
No competing financial interests exist.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chen, JL., Liu, CH. & Yi, CG. Transconjunctival Orbital Septum Fat Release and Preservation for Orbitopalpebral Sulcus in Lower Eyelid Blepharoplasty. Aesth Plast Surg 41, 568–572 (2017). https://doi.org/10.1007/s00266-017-0809-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-017-0809-z